


Abstract
The clinical characteristics of reversible left ventricular dysfunction due to “takotsubo” cardiomyopathy have been described, but the origin of this condition remains unclear. This study investigated 123I-metaiodobenzlguanidine (123I-MIBG) myocardial scintigraphy in patients with takotsubo cardiomyopathy. Methods: Eight consecutive patients with takotsubo cardiomyopathy were studied. Left ventricular wall motion was monitored by echocardiography until wall motion normalized. 123I-MIBG myocardial scintigrams were performed within 3 d of admission (0 mo) and after the improvement of left ventricular dysfunction (3 mo). Early images were obtained at 30 min after radioisotope injection and delayed images were obtained after 4 h. The heart-to-mediastinum ratio (H/M ratio) and the washout rate were calculated. Results: The mean left ventricular ejection fraction improved significantly (from 42.8% ± 8.7% to 66.5% ± 7.9%; P < 0.0001) and normalized after 19.4 ± 5.4 hospital days. The early H/M ratio was significantly higher than the late ratio at 0 mo (2.16 ± 0.25 vs. 1.89 ± 0.24, respectively; P < 0.05), but not at 3 mo. The washout rate was significantly greater at 0 mo than at 3 mo (39.1% ± 10.2% vs. 25.4% ± 6.3%, respectively; P < 0.05). Conclusion: In patients with takotsubo cardiomyopathy, initial 123I-MIBG myocardial scintigraphy depicted a unique pattern of ventricular asynergy and indicated the existence of cardiac sympathetic hyperactivity, although coronary blood flow was maintained. These findings strongly suggest that takotsubo cardiomyopathy could be caused by neurogenic myocardial stunning.
- “takotsubo” cardiomyopathy
- reversible ventricular dysfunction
- 123I-metaiodobenzlguanidine
- stunned myocardium
- catecholamine
There have been several reports about reversible left ventricular (LV) dysfunction accompanied by ST segment elevation and symptoms similar to those of acute myocardial infarction in patients without coronary artery lesions, even during the acute phase (1–16). The wall motion of such patients returns to normal within a few weeks. During the acute phase, however, a “takotsubo” (Japanese octopus fishing pot)-shaped left ventricle is observed, which displays the features of apical akinesis and basal hyperkinesis. This type of cardiomyopathy (takotsubo cardiomyopathy [TC]) generally occurs in women >60 y old, and physical or mental stress often precedes the onset. Autonomic imbalance has been suggested to be related to the development of this condition and we have previously reported cases of TC that were possibly precipitated by catecholamine cardiotoxicity (11,12).
Metaiodobenzlguanidine (MIBG) has a structure similar to that of norepinephrine and is processed by the same uptake and storage mechanisms (17). MIBG is stored in the presynaptic vesicles and is secreted after stimulation by acetylcholine released from preganglionic neurons (18,19). 123I-MIBG scintigraphy was developed to evaluate cardiac sympathetic nervous function, and the usefulness of 123I-MIBG imaging has been demonstrated in many cardiac diseases (20–24). For example, decreased MIBG uptake on delayed images is closely related to LV dysfunction in patients with chronic heart failure (20,21,23). However, 123I-MIBG imaging has not been used to investigate TC because this disease is uncommon.
In this study, we analyzed clinical and radionuclide imaging data from 8 TC patients, in an attempt to determine the etiology of this unusual cardiomyopathy.
MATERIALS AND METHODS
Subjects
A total of 653 patients with the sudden onset of heart failure, including acute myocardial infarction–like abnormal Q waves and ST–T changes on the electrocardiogram (ECG), were admitted to our institution from January 1998 to December 2002. They included 637 patients with acute myocardial infarction, 13 patients (1.9%) with TC, and 3 patients with acute viral myocarditis. This study involved 8 patients who agreed to undergo 123I-MIBG myocardial scintigraphy in the acute phase of TC. Subjects with diseases known to influence the autonomic nervous system (such as severe diabetes mellitus, Parkinson’s disease, or Guillain–Barré syndrome) and subjects with atrial fibrillation were excluded from the study. For at least 12 h before 123I-MIBG imaging, the subjects were not allowed to smoke or to drink coffee, tea, or cola beverages. In addition, all medical therapy known to influence 123I-MIBG uptake was discontinued before the study.
A diagnosis of TC was made on the basis of the following findings: (a) sudden occurrence of heart failure accompanied by acute myocardial infarction–like symptoms, (b) a takotsubo-shaped hypokinetic left ventricle on echocardiography and left ventriculography, (c) absence of coronary artery disease on coronary angiography despite the presence of acute myocardial infarction–like ST segment abnormalities on the ECG, and (d) complete normalization of the LV dysfunction within a few weeks.
ECG and Echocardiography
A standard 12-lead ECG was recorded on admission as well as at 6, 12, 24, 48, and 72 h and at 1, 2, and 4 wk after admission. The locations of the precordial leads were marked on each patient’s chest wall with an indelible marker. Two-dimensional echocardiography (SSH-140A; Toshiba) was performed 2 or 3 times during the first week of hospitalization until LV wall motion was normalized.
Cardiac Catheterization
Cardiac catheterization was always performed within 1 h of admission using 6-French catheters for both coronary angiography and left ventriculography. The LV ejection fraction (LVEF) was calculated by Simpson’s method (25). A Swan–Ganz catheter was then placed at a suitable position and hemodynamics were monitored continuously throughout the stay of each patient in the coronary care unit.
In all patients, cardiac catheterization was repeated after LV function had normalized according to echocardiography. During this later coronary angiography study, an acetylcholine provocation test was also performed in all patients by injection of acetylcholine chloride over 30 s at a dose of 50 μg for the right coronary artery and 100 μg for the left coronary artery.
Radionuclide Studies
SPECT of the heart was performed using 123I-MIBG (123I-MyoMIBG; Daiichi Radioisotope Laboratory). Imaging was initially done within 3 d of hospitalization in the acute phase (0 mo) and was repeated after 3 mo in the chronic phase (3 mo). A dose of 123I-MIBG (111 MBq/0.03–0.10 mg) was injected into the left antecubital vein and scanning was started after 15 min to study early 123I-MIBG uptake. A second scan was obtained 4 h after injection using the same imaging settings to study delayed uptake.
Before the SPECT study, anterior and lateral planar images were acquired for 90 s, using a γ-camera equipped with a low-energy, high-resolution collimator and a 256 × 256 matrix. A triple-head γ-camera (GCA9300A/DI; Toshiba Medical) equipped with a low-energy, high-resolution collimator was used for 123I-MIBG imaging. Three detectors (3 × 120°) acquired 30 views for 40 s each in 6° steps using a 64 × 64 matrix. The energy window of 123I was centered at 159 keV with a 20% window.
Data Analysis
Raw imaging data were reconstructed using a Butterworth-filtered (order, 8; cutoff frequency, 0.20 cycle/pixel) backprojection technique. Transaxial slices were reconstructed and reoriented to represent coronal slices, after which horizontal long-axis and short-axis slices were produced by axis shift. On anterior planar images, regions of interest (ROIs) were drawn over the entire heart and upper mediastinum. Using the counts in these ROIs, the heart-to-mediastinum ratio (H/M ratio) and the global washout rate (WR) of 123I-MIBG were calculated as follows:

 Background or time decay correction was not done for calculating WR.
Background or time decay correction was not done for calculating WR.
Statistical Analysis
Results are expressed as the mean ± SD. To assess the significance of differences between groups, 1-way ANOVA was performed. Parameters between acute and chronic phase were compared using the paired t test. In all analyses, P < 0.05 was considered statistically significant.
Ethics
The study protocol consisted of electrocardiography and echocardiography, quantitative coronary angiography (including a provocation test), measurement of cardiac hemodynamics, routine blood tests, and 123I-MIBG studies in the acute and stable phases of TC. This study was approved by the Human Investigation Committee of St. Marianna University School of Medicine. The nature and purpose of the study and the risks involved were explained to all subjects before their enrollment, and written informed consent to participation in the study was obtained.
RESULTS
Clinical Characteristics of Subjects
Seven women and 1 man (75.1 ± 9.3 y old) participated in this study. None of them had a family history of TC or a past history of heart disease, but 6 patients had a history of hypertension. In 6 patients, a possible triggering event was detected, including pneumothorax, primary ventricular fibrillation (loss of consciousness), intestinal perforation, severe knee joint pain, bilateral leg numbness, and swimming (overexertion). The reason for admission was chest pain in 4 patients, loss of consciousness in 2, abdominal pain due to intestinal perforation in 1, and unexplained fatigue in 1. Patients 2, 4, 5, 6, and 8 suffered from physical and mental stress before the onset of TC.
Laboratory Findings
Laboratory test results are shown in Table 1. The white blood cell count was increased on admission (>8.0 × 109/L) in 6 patients. Cardiac enzymes, including creatinine kinase and its MB isoenzyme, were significantly increased in patient 5 but not in the other patients. Troponin T was increased above the normal range (0.00082 × 109/L vs. <0.0001 × 109/L). The plasma norepinephrine level was elevated in 5 patients (normal range, 0.00024–0.00057 × 109/L), and a marked increase of plasma brain natriuretic peptide was observed, with a mean value of 0.6296 × 109/L (normal range, <0.0184 × 109/L). Tests of paired serum samples for viral infection were negative in all patients. The laboratory findings returned to normal within 1 wk in most patients. Patient 5 developed sepsis due to a small bowel perforation. After small bowel surgery was performed, the patient underwent continuous hemodialysis and endotoxin capture therapy, but laboratory findings did not normalize until about 1 mo after admission.
Laboratory Data on Admission and Peak Cardiac Enzymes
ECG Changes
All 8 patients had acute myocardial infarction–like ECG changes, with ST segment elevation and Q waves, as well as inverted T waves in the chronic phase. ST segment elevation with abnormal Q waves persisted for 1 wk and then was converted to a non-Q and inverted T wave pattern without any ST segment change over the next 1 mo. The ECG changes were not specific to any lead. ST segment depression was observed in 1 patient, whereas ST segment elevation persisted for 1 wk or more in the remaining 7 patients. Ultimately, inverted T waves were observed in the leads that showed ST segment changes and Q waves, but the abnormal Q waves did not persist in all patients.
Cardiac Catheterization Data and Cardiac Function
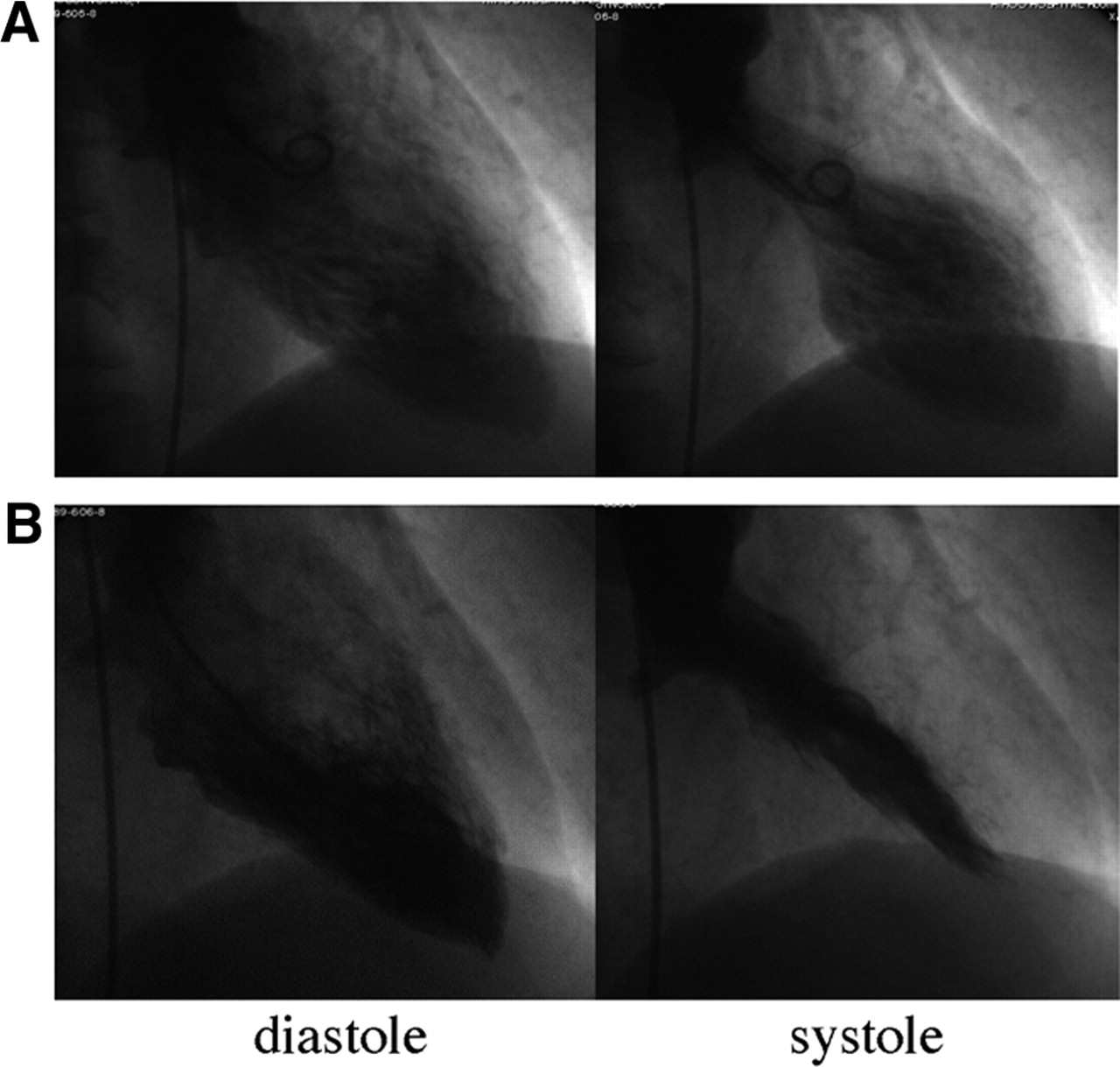
Cardiac catheterization was performed within 1 h of admission in all patients. Angiograms revealed the absence of coronary artery stenosis or obstruction, whereas the left ventricle had a takotsubo morphology (Fig. 1A).
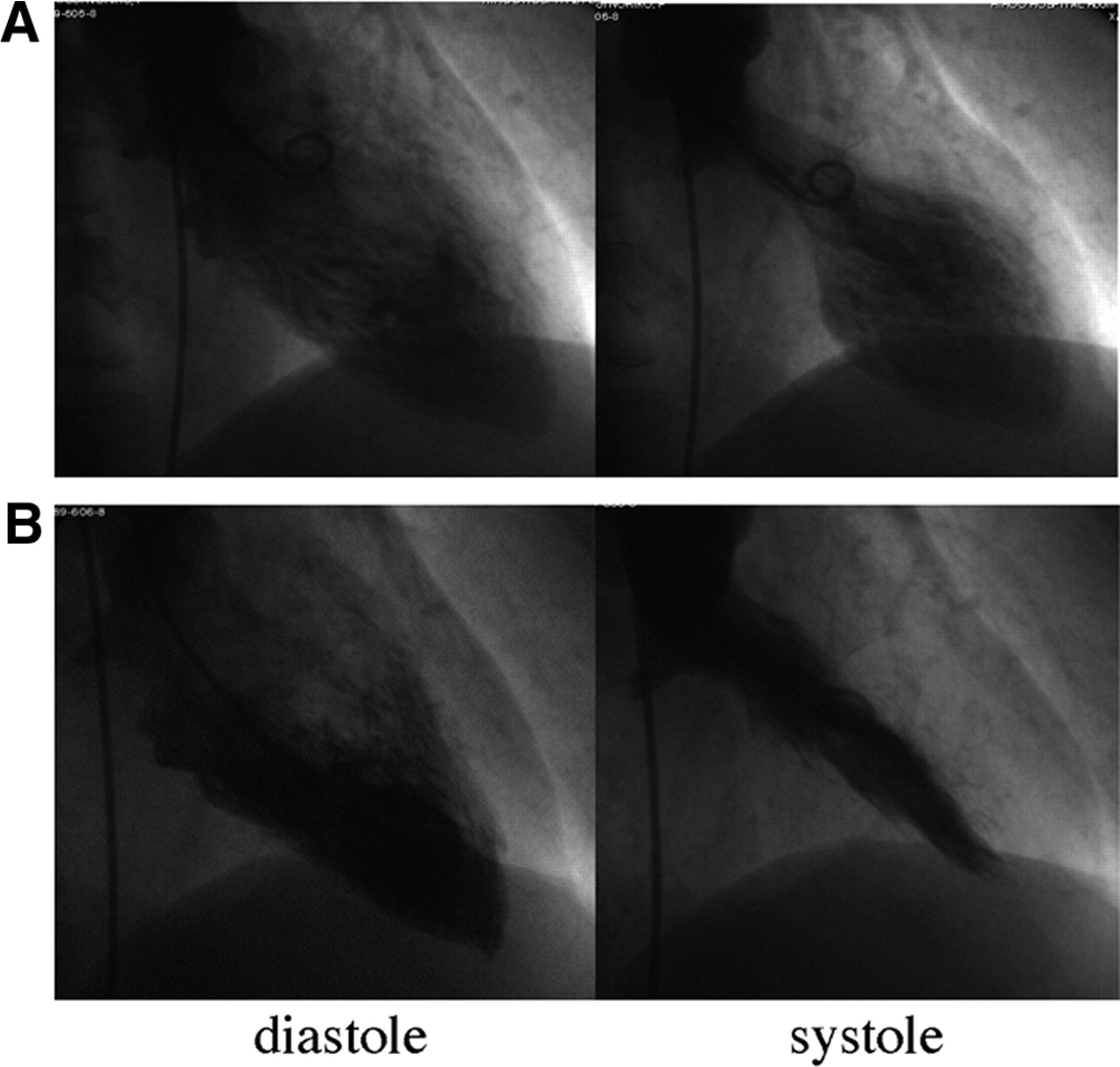
Patient 5: Changes on left ventriculography. (A) Asynergy associated with apical akinesis and basal hyperkinesis is evident on first hospital day. (B) On second hospital day, there is normal contraction and significantly improved ejection fraction.
The changes of hemodynamic parameters are shown in Table 2. Hemodynamic support was needed by 2 patients (patients 1 and 5) during the acute phase but not by the remaining 6 patients. The mean values of the LVEF, pulmonary capillary wedge pressure, cardiac output, and cardiac index were 42.8% ± 8.7%, 8.0 ± 3.9 mm Hg, 2.7 ± 0.8 L/min, and 2.0 ± 0.4 L/min/m2, respectively.
Initial Cardiac Catheterization Data, Hemodynamic Support, and Clinical Course
Cardiac catheterization was repeated after LV dysfunction had resolved on echocardiography, and cardiac function had improved in all patients (Fig. 1B). Furthermore, coronary angiography with acetylcholine provocation was performed in patients during this second catheterization study but did not induce coronary artery spasm in any of them.
Clinical Course
Table 2 also summarizes the clinical course of the patients. None of them received oral medications such as digitalis, angiotensin-converting-enzyme inhibitors, angiotensin II receptor antagonists, or β-blockers during their hospital stay. However, patient 1 required mechanical hemodynamics with intraaortic balloon pumping support for 3 d during the acute phase. Complete normalization of LV contraction was confirmed by 19.4 ± 5.4 hospital days (the LVEF improved to 66.5% ± 7.9%; P < 0.0001). In patients 1 and 4, therapy for arrhythmias was needed. Intravenous administration of magnesium sulfate (2 mg) was effective in suppressing the frequent occurrence of nonsustained ventricular tachycardia in patient 1; patient 4 was diagnosed as having idiopathic ventricular fibrillation, which required the implantation of a cardioverter defibrillator. During a follow-up period of 6 mo to 5 y, none of the patients had any further cardiac events.
123I-MIBG Myocardial Scintigraphy
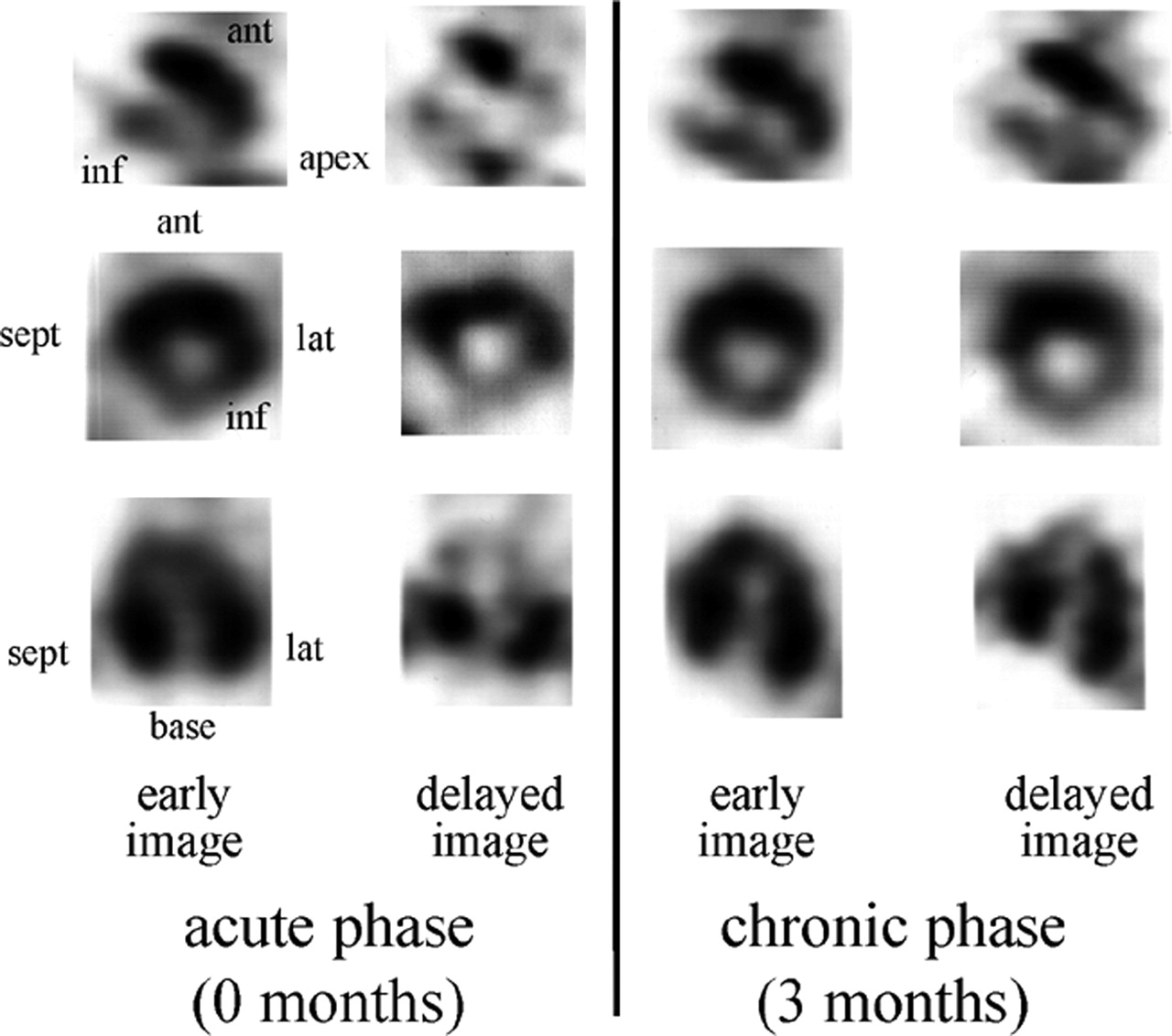
Typical 123I-MIBG SPECT findings of a patient are shown in Figure 2. At 0 mo, the early images showed decreased myocardial 123I-MIBG uptake in the distal anterior wall, apex, and inferior wall of the left ventricle. On delayed images, washout was increased. At 3 mo, the early images still revealed a decrease of uptake in the inferoposterior wall and apex, but washout was less prominent in the delayed images.

123I-MIBG SPECT images. Early images obtained at 0 mo show decreased myocardial perfusion in distal anterior wall, apex, and inferior wall. In 4-h delayed images, washout is increased. At 3 mo, early images still show decreased uptake of 123I-MIBG at inferoposterior wall and apex, although washout is less prominent than at 0 mo. Ant = anterior; inf = inferior; sept = septal; lat = lateral.
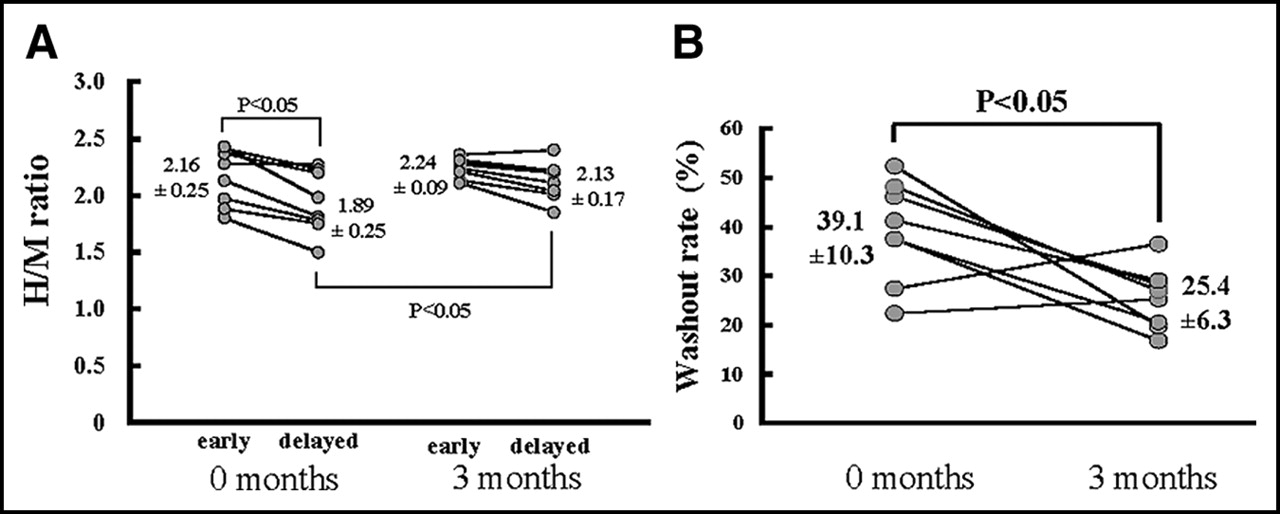
The H/M ratio and WR for each subject are shown in Table 3. At 0 mo, there was a significantly greater H/M ratio in the early images than in the delayed images (2.16 ± 0.25 vs. 1.89 ± 0.24; P < 0.05) (Fig. 3A). By 3 mo, however, there was no difference of the H/M ratio between the early images and the delayed images. Thus, the delayed images showed a significantly greater decrease of the H/M ratio at 0 mo than at 3 mo (P < 0.05), and the WR itself was significantly larger at 0 mo than at 3 mo (39.1% ± 10.3% vs. 25.4% ± 6.3%; P < 0. 05) (Fig. 3B).

Results of 123I-MIBG myocardial scintigraphy in early and chronic phases of TC (A) and 123I-MIBG myocardial WR (B). At 0 mo, H/M ratio shows significant decrease from 2.16 in early images to 1.89 in delayed images (P < 0.05). At 3 mo, H/M ratio does not decrease significantly. Delayed H/M ratio shows significant increase from 0 to 3 mo (P < 0.05). 123I-MIBG myocardial WR is significantly greater at 0 mo (39.1% ± 10.3%) than at 3 mo (25.4% ± 6.3%) (P < 0.05).
123I-MIBG Myocardial Scintigraphy Findings
DISCUSSION
To our knowledge, this study provides the first data about cardiac sympathetic nervous dysfunction in patients with TC. Our results strongly suggest that this condition might be caused by neurogenic myocardial stunning.
123I-MIBG Myocardial Scintigraphy Findings
In the 8 TC patients, 123I-MIBG myocardial scintigraphy revealed an increase of the H/M ratio and WR at the time when ventricular dysfunction was present. Because of lack of a control value for H/M and WR, we cited the references we acquired under the same condition—that is, photo peak energy, collimator used, matrix size, H/M ratio and WR calculation, and so on (26,27). A decrease of cardiac MIBG uptake is thought to reflect impaired adrenergic function or denervation in various cardiac diseases (17–23). The H/M ratio at 3–4 h after injection seems to be a good quantitative index of neuronal MIBG uptake in the clinical situation (17), but this index is not sensitive enough to detect a slight reduction of MIBG accumulation (28). In our patients, the delayed H/M ratio was decreased significantly at 0 mo and then increased significantly at 3 mo. These findings suggest that cardiac adrenergic nervous dysfunction was present in the acute phase, whereas the data at 3 mo indicate a gradual improvement of adrenergic function. Such adrenergic dysfunction was localized to the apex. Although apical 123I-MIBG uptake was not normalized at 3 mo, a longer observation period may have demonstrated complete recovery. Owa et al. (5) obtained radionuclide images over a period of 1 y in 4 patients with TC. They reported that the recovery of MIBG uptake was slower than that of other tracers and also suggested that TC was related to a disturbance of cardiac sympathetic innervation. Moriya et al. (8) observed that the H/M ratio obtained with 123I-MIBG did not fully recover after a 6-mo follow-up period in a TC patient. However, the H/M ratios of our patients improved despite a shorter follow-up period, suggesting that they have less severe cardiac adrenergic dysfunction than previously reported patients. Although a decrease of the H/M ratio is thought to be related to a poor prognosis in patients with ischemic or dilated cardiomyopathy (21), this ratio does not seem to be related to the prognosis in TC because of the good outcome in our series.
In patients with various types of cardiomyopathy, an increase in the WR of MIBG (5,10,11,23,24,29) has been demonstrated, but the WR behavior remains controversial in patients with diabetes mellitus (30). The cardiac MIBG washout rate is an index of sympathetic activity in relation to the ability to store norepinephrine (31). In our patients, the WR was increased at 0 mo. This increase of the WR might imply some kind of myocardial damage that resulted in an increase of cardiac sympathetic activity to compensate for the dysfunction. An increase of the WR for MIBG indicates that there is increased norepinephrine spillover from the sympathetic nerve endings or increased clearance of excess MIBG by extraneural tissues. In 5 of our patients, the plasma norepinephrine concentration was increased on admission, whereas it was within the normal range in the remaining patients. The patients with an increase of the WR corresponded to those with an increased plasma norepinephrine concentration. Ueyama et al. (10) found that experimentally induced emotional stress could cause ventricular hypocontraction in rats and they concluded that the mechanism was based on adrenoceptor hypereactivity. This may also be a plausible mechanism for the occurrence of TC.
Reversible Ventricular Dysfunction
Myocardial stunning is usually considered to be the mechanism underlying reversible ventricular dysfunction. Kurisu et al. (14) have suggested that disturbance of the coronary microcirculation was the cause of such reversible dysfunction, but the myocardial perfusion scintigraphy has revealed few abnormal findings. Stunning due to vasospastic angina might be one possible mechanism of reversible ventricular dysfunction, but none of our patients developed vasospasm in the provocation test. Another possible mechanism is some kind of inflammatory heart disease (13), which is suggested by the documented infiltration of small mononuclear cells in some patients. Such cellular infiltration has not been found in patients with ischemic stunning (32). Our subjects did not have acute viral myocarditis on the basis of tests of paired serum samples. One report has described histologic myocardial damage in the absence of coronary artery disease in fatal cases of subarachnoid hemorrhage (33). However, none of our subjects exhibited any such clinical features and their reversible ventricular dysfunction did not fit into any of these prior categories.
Limitations
We could not perform a large-scale prospective study because of the small number of patients due to the rarity of TC. Thus, further studies on a larger scale are necessary.
A high plasma catecholamine concentration or activation of cardiac catecholamine receptors was strongly suspected to be related to the development of TC. Because our study failed to elucidate why the asynergy was regional, the distribution of the catecholamine receptors in the myocardium should be examined to determine the mechanism of regional dysfunction.
Furthermore, we did not calculate the regional uptake of 123I-MIBG. Again, more detailed research into regional wall motion abnormalities is needed.
Finally, we used one radionuclide, 123I-MIBG. To clarify the pathogenesis of TC, further study using various radionuclides at the same period is necessary.
CONCLUSION
The features of 123I-MIBG myocardial scintigraphy were investigated in 8 patients with TC, who were identified among 653 patients with a sudden onset of LV dysfunction. An increase of the H/M ratio and WR were observed at 0 mo when ventricular dysfunction was present. These results strongly suggest that TC might be caused by neurogenic myocardial stunning.
Footnotes
Received Oct. 27, 2003; revision accepted Jan. 14, 2004.
For correspondence or reprints contact: Yoshihiro J. Akashi, MD, Division of Cardiology, Department of Internal Medicine, St. Marianna University School of Medicine, 2-16-1 Sugao Miyamae-ku, Kawasaki-City, Kanagawa-Prefecture, 216-8511, Japan.
E-mail: johnny{at}marianna-u.ac.jp
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Takotsubo syndrome: aetiology, presentation and treatment
- Pathophysiology of Takotsubo Syndrome
- 123I-MIBG Scintigraphy in the Subacute State of Takotsubo Cardiomyopathy
- Sexual dimorphism in cardiac norepinephrine spillover: a NET difference
- Takotsubo cardiomyopathy: a diagnostic challenge
- Takotsubo Cardiomyopathy: A Unique Cardiomyopathy With Variable Ventricular Morphology
- Tako-tsubo cardiomyopathy (apical ballooning)
- Stress cardiomyopathy: aetiology and management
- Tako-tsubo syndrome on the rise: a review of the current literature