


Abstract
In chronic heart failure, elevated plasma norepinephrine (NE) levels and a disparity between the neuronal release and the effective reuptake of NE lead to an increased concentration of NE in the presynaptic cleft, causing a downregulation of the myocardial β-adrenoceptors. The clinical and prognostic effectiveness of β-blocker therapy has been shown in patients with chronic heart failure in several large trials. The purpose of this study was to investigate the effect of long-term β-blocker therapy on the cardiac adrenergic nervous system as assessed by the myocardial uptake of 123I-metaiodobenzylguanidine (MIBG), an analog of NE, in idiopathic dilated cardiomyopathy (IDC). Methods: In 10 patients with IDC and stable chronic heart failure the myocardial MIBG uptake was measured at baseline and at 1 y (median, 11.5 mo) after treatment with β-blockers (metoprolol, n = 5; bisoprolol, n = 1; and carvedilol, n = 4) in addition to standard medication. In parallel with the changes in MIBG uptake, the New York Heart Association functional class, the left ventricular ejection fraction (LVEF), and the left ventricular end-diastolic diameter (LVEDD) were documented before and after 1 y of therapy with β-blockers. Results: During the 1-y follow-up, a significant increase in myocardial 123I-MIBG uptake (P = 0.005) in parallel with an improved LVEF (P = 0.005) and a reduced LVEDD (P = 0.019) was found. A trend toward an improvement of the New York Heart Association functional class under the β-blocker therapy (P = 0.139) was also found. Conclusion: Assessment of the myocardial 123I-MIBG uptake is a useful noninvasive tool for evaluating changes in cardiac sympathetic nerve activity under medical therapy. Long-term treatment with β-blockers in IDC causes a recovery of the cardiac adrenergic nervous system concomitantly with a clinical and hemodynamic improvement.
In chronic heart failure the increased adrenergic drive is reflected by an elevated concentration of circulating norepinephrine (NE) (1–3), an enhanced neuronal release of NE (4,5), and an impaired efficiency of NE reuptake and storage (6–8). This disproportion leads to enhanced NE levels in the synaptic cleft and induces the downregulation and uncoupling of the β-receptors in chronic heart failure (9–11). The myocardial neuronal uptake of 123I-metaiodobenzylguanidine (MIBG), a transmitter analog of NE with the same affinity for sympathetic nerve endings (12,13), can be used to evaluate the cardiac sympathetic nervous system (12,14).
Recently, in several large-scale trials, hemodynamic improvements (15,16) and prognostic benefits of β-blocker therapy in chronic heart failure have been clearly shown (17–19). β-Blockers such as metoprolol and bisoprolol are known to interact with the cardiac sympathetic activity in the failing heart and to cause an upregulation of β-adrenergic receptors (20–23). Others such as carvedilol can produce β2-receptor blockade (24), leading to a lower cardiac adrenergic activity, but no upregulation in the β-receptor density (21,22).
The purpose of this study was to investigate the effect of long-term β-blocker therapy on the cardiac adrenergic nervous system as assessed by the time course of myocardial neuronal MIBG uptake, calculated according to a new method (25), in patients with idiopathic dilated cardiomyopathy (IDC) during a 1-y follow-up period, and to relate the scintigraphic changes to the clinical and hemodynamic course of these patients.
MATERIALS AND METHODS
Patients and Study Design
We included prospectively patients according to the following criteria: stable chronic heart failure associated with IDC with left ventricular ejection fraction (LVEF) < 55% (range, 17%–40%); on permanent medication, including angiotensin-converting enzyme (ACE) inhibitors and digitalis, for at least 3 mo; and no previous treatment with β-blockers. Exclusion criteria were coronary artery disease, valvular heart disease, a history of arterial hypertension, insulin-dependent diabetes mellitus, neuropathy, and treatment with other drugs affecting MIBG kinetics. Aside from the routine clinical examinations, echocardiography and coronary angiography with left and right heart catheterization, including left ventricular endomyocardial biopsies, were performed on all patients to exclude acute myocarditis according to the Dallas criteria (26).
The study design included assessment of myocardial 123I-MIBG uptake at baseline and at 1 y after treatment with β-blockers in patients with IDC. In parallel, the time course of the New York Heart Association functional class and the hemodynamic parameters (LVEF and left ventricular end-diastolic diameter [LVEDD]) were determined by an experienced physician according to the recommendations of the American Society of Echocardiography (27,28). The local ethics committee approved this study, and written informed consent was obtained from all patients.
β-Blocker Therapy
In addition to the standard therapy with ACE inhibitors, diuretics, and digitalis for chronic heart failure, β-blockers were administered to each patient taking into consideration the individual medical history and any other accompanying diseases. Thus, the initial recommended starting doses for the three β-blockers approved for treatment of chronic heart failure (15–18) were as follows: metoprolol, 5 mg twice daily; bisoprolol, 1.25 mg once a day; and carvedilol, 3.125 mg twice daily, respectively. The dosage was gradually increased according to the recommended biweekly titration (15,17,18). The daily target doses were as follows: metoprolol, 100–150 mg; bisoprolol, 5–10 mg; and carvedilol, 50 mg. Development of incompatibility was countered by individually adjusting the dose of the corresponding β-blocker.
Combined Myocardial 123I-MIBI and 99mTc-MIBG SPECT Protocol
The cardiac 123I-MIBG uptake was measured as the myocardial-to-left ventricular cavity density ratio of voxel values, the M/C ratio (25), according to a protocol using combined SPECT studies with 370 MBq 99mTc-methoxyisobutylisonitrile (MIBI) (DuPont, Pharma Radiopharmaceuticals, Billerica, MA) and 185 MBq 123I-MIBG (Nycomed Amersham, Buckinghamshire, UK) as described (29). Briefly, the position and contour of the heart were initially determined by means of cardiac 99mTc-MIBI imaging. After a 4-h rest period, when an equilibrium in cardiac 123I-MIBG concentration existed, myocardial 123I-MIBG uptake was measured using a volume-of-interest technique to separate the myocardium from the left ventricular cavity according to the 99mTc-MIBI perfusion imaging in the short-axis slices obtained from the double radionuclide study with 99mTc-MIBI and 123I-MIBG. The M/C ratio was calculated, calibrating the left ventricular cavity activity by the 123I activity in a venous blood sample as a reference (25), according to the following equation:

This quantitation of the 123I-MIBG uptake was performed for all patients at baseline and after 1 y (median, 11.5 mo; range, 8–18 mo) of treatment with β-blockers by two independent observers who were unaware of the clinical and hemodynamic course of the patients. Differences were resolved by consensus. To exclude any influence of the accompanying medication on the cardiac neuronal uptake function as far as possible, an attempt was made to keep the patients on a constant fixed dosage of digitalis and ACE inhibitors, which are known to affect sympathetic activity (30,31) and the myocardial 123I-MIBG uptake (30), for 3 mo before administration of β-blockers and inclusion in the study.
Statistical Analysis
Continuous data are given as mean ± SD and categoric data are expressed as relative frequency (percentage). To compare data at baseline with those at 1-y follow-up, a Student t test for paired data and the χ2 test for the New York Heart Association functional class were used. Significant differences were defined by P < 0.05.
RESULTS
Patients
According to the inclusion criteria, 10 patients with IDC were enrolled in the study. Table 1 shows the clinical characteristics, including medication and hemodynamic parameters, of the patients. The ACE inhibitor had to be withdrawn in one patient because of incompatibility and was replaced by an angiotensin-II type 1 receptor antagonist. Five patients received metoprolol, one patient had bisoprolol, and four patients had carvedilol. The β-blocker therapy was not discontinued completely in any patient because of adverse side effects during the 1-y follow-up period. At the time of the second myocardial 99mTc-MIBI and 123I-MIBG scintigraphy after 1 y, the average daily dosage of metoprolol (n = 5) was 65 ± 39 mg (range, 25–100 mg); of bisoprolol (n = 1), 5 mg; and of carvedilol (n = 4), 39 ± 22 mg (range, 12.5–50 mg).
Clinical Baseline Characteristics and Hemodynamic Parameters
One-Year Follow-Up Under β-Blocker Therapy
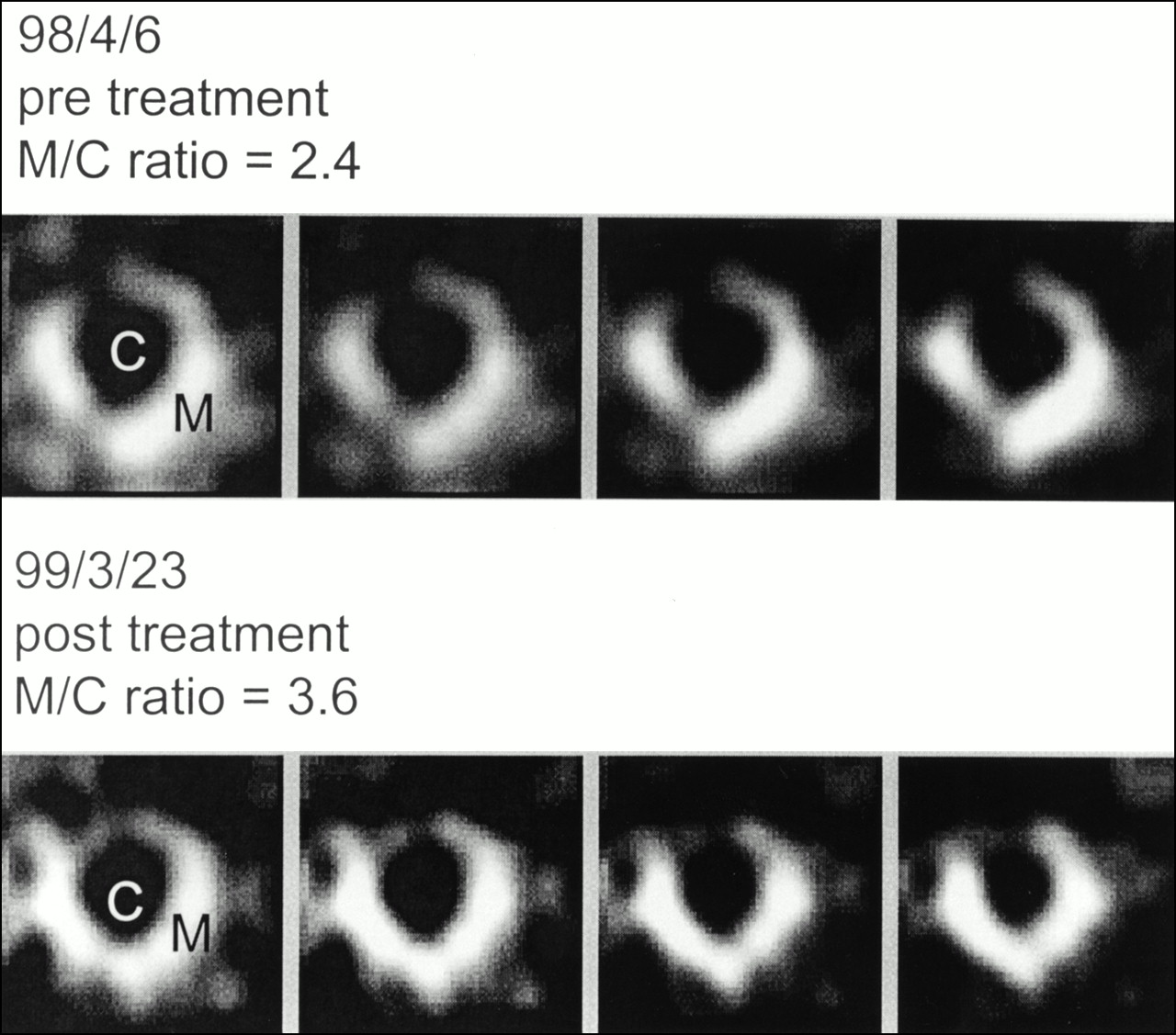
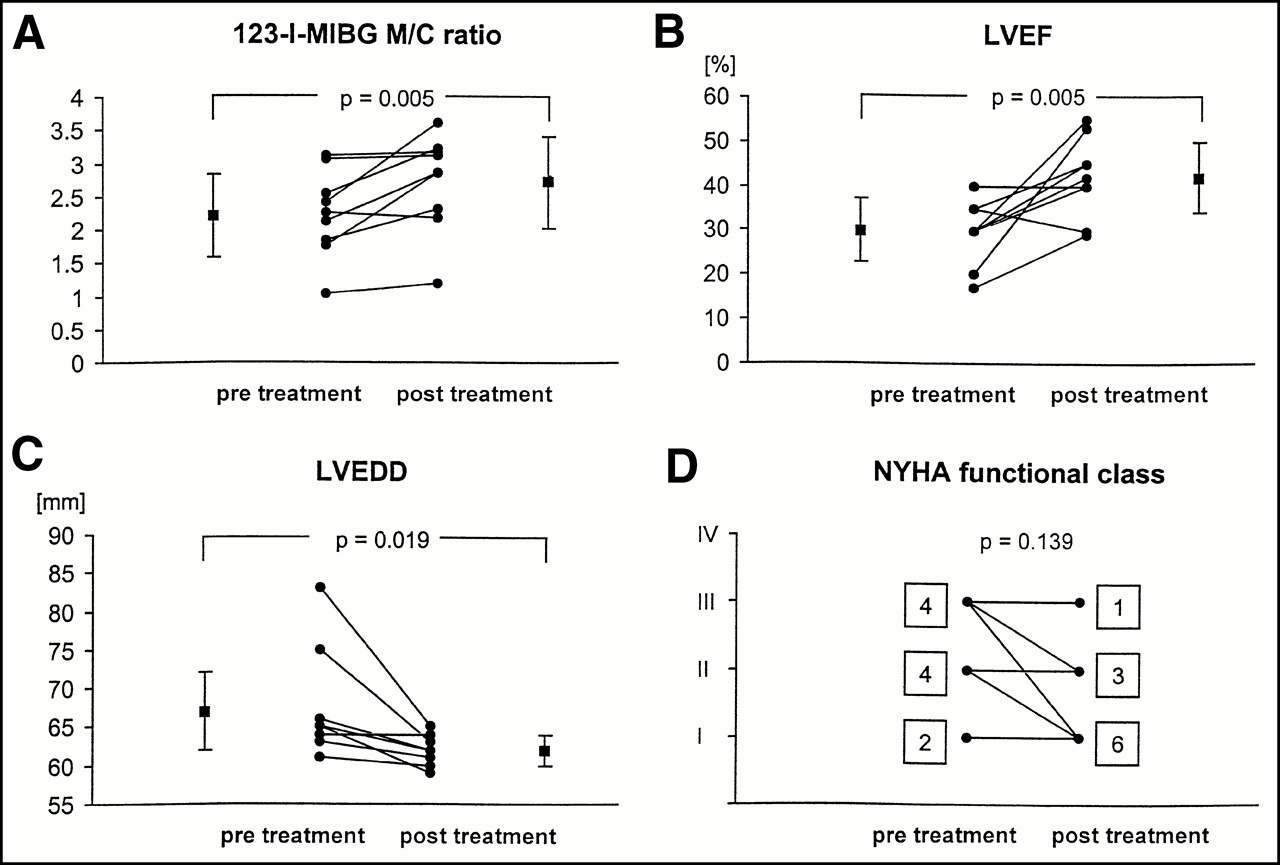
Table 2 shows the changes in the data from baseline compared with the 1-y follow-up after treatment with β-blockers. There was a significant increase in the M/C ratio reflecting the myocardial 123I-MIBG uptake from 2.21 ± 0.62 to 2.72 ± 0.69 (P = 0.005) and in LVEF from 30% ± 7% to 42% ± 7% (P = 0.005). Furthermore, LVEDD decreased significantly from 67 ± 7 mm to 62 ± 2 mm (P = 0.019). The distribution of the New York Heart Association functional class on entry and after 1 y also indicates a trend toward a clinical improvement under β-blocker therapy (P = 0.139). Figure 1 shows an example of the improved 123I-MIBG uptake after long-term β-blocker therapy, in this case with bisoprolol. Changes of the four parameters are summarized in Figure 2. Furthermore, the individual course of LVEF and the M/C ratio showed a good relationship between the changes in LVEF and those in the M/C ratio (Fig. 3).

123I-MIBG images obtained from short-axis reconstruction in patient with IDC. The M/C ratio reflecting myocardial 123I-MIBG uptake increased from 2.4 before treatment to 3.6 after treatment with β-blocker (bisoprolol) for about 1 y. C = left ventricular cavity; M = myocardium.
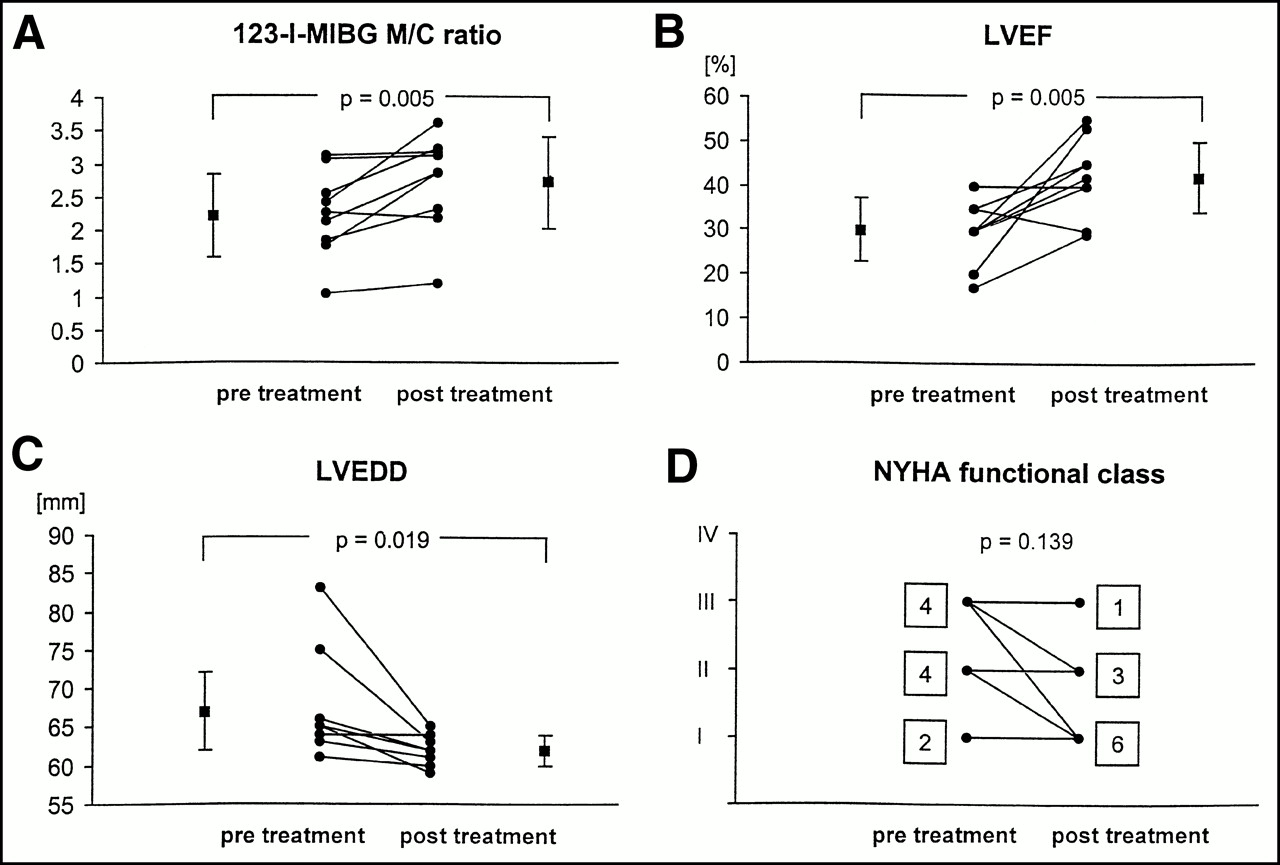
Changes in 123I-MIBG M/C ratio (A), LVEF (B), LVEDD (C), and New York Heart Association (NYHA) functional class (D) under β-blocker therapy for 1 y. Individual data points for each patient and mean values ± SD of four parameters measured at entry and after 1 y of treatment with β-blockers are shown.
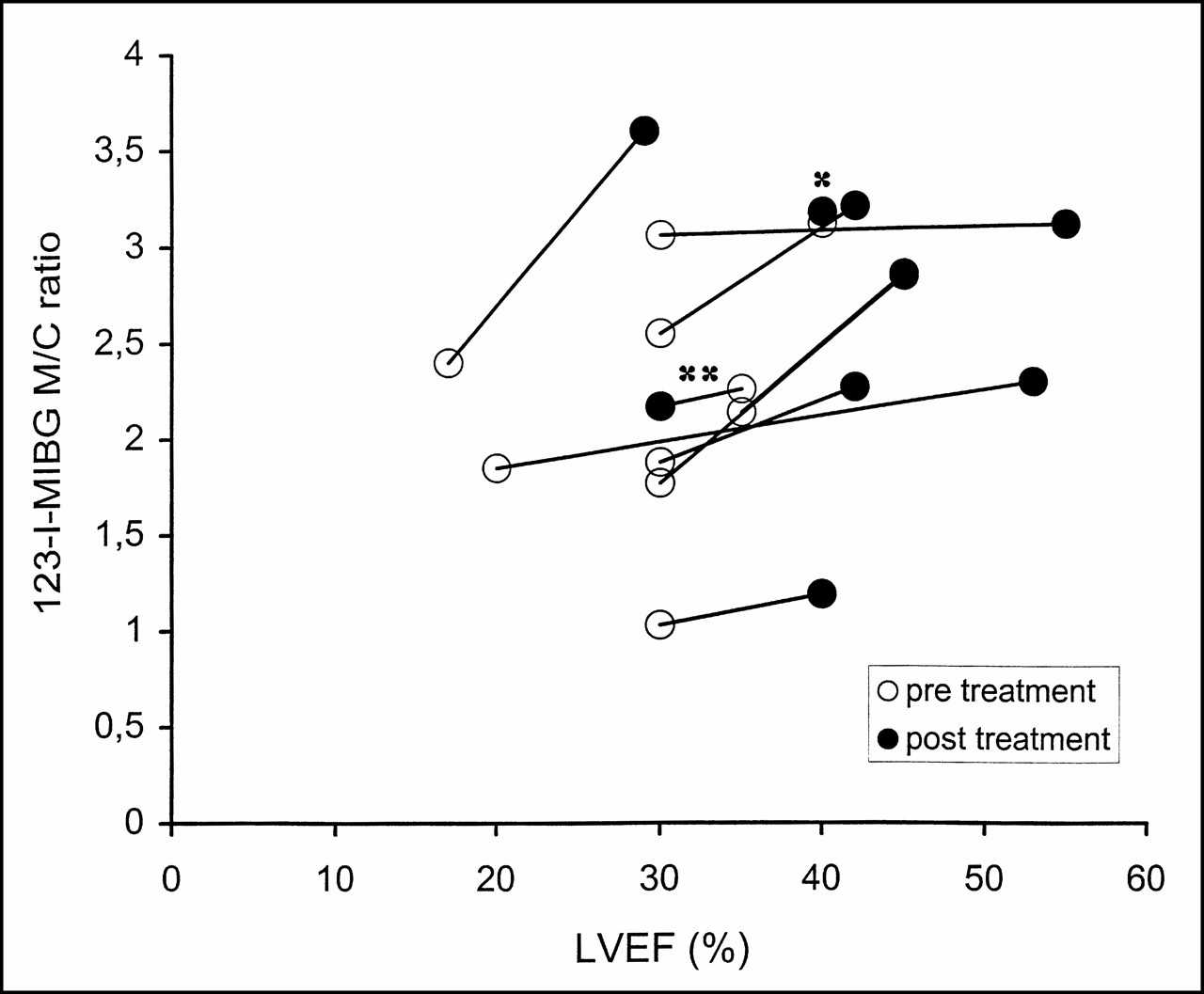
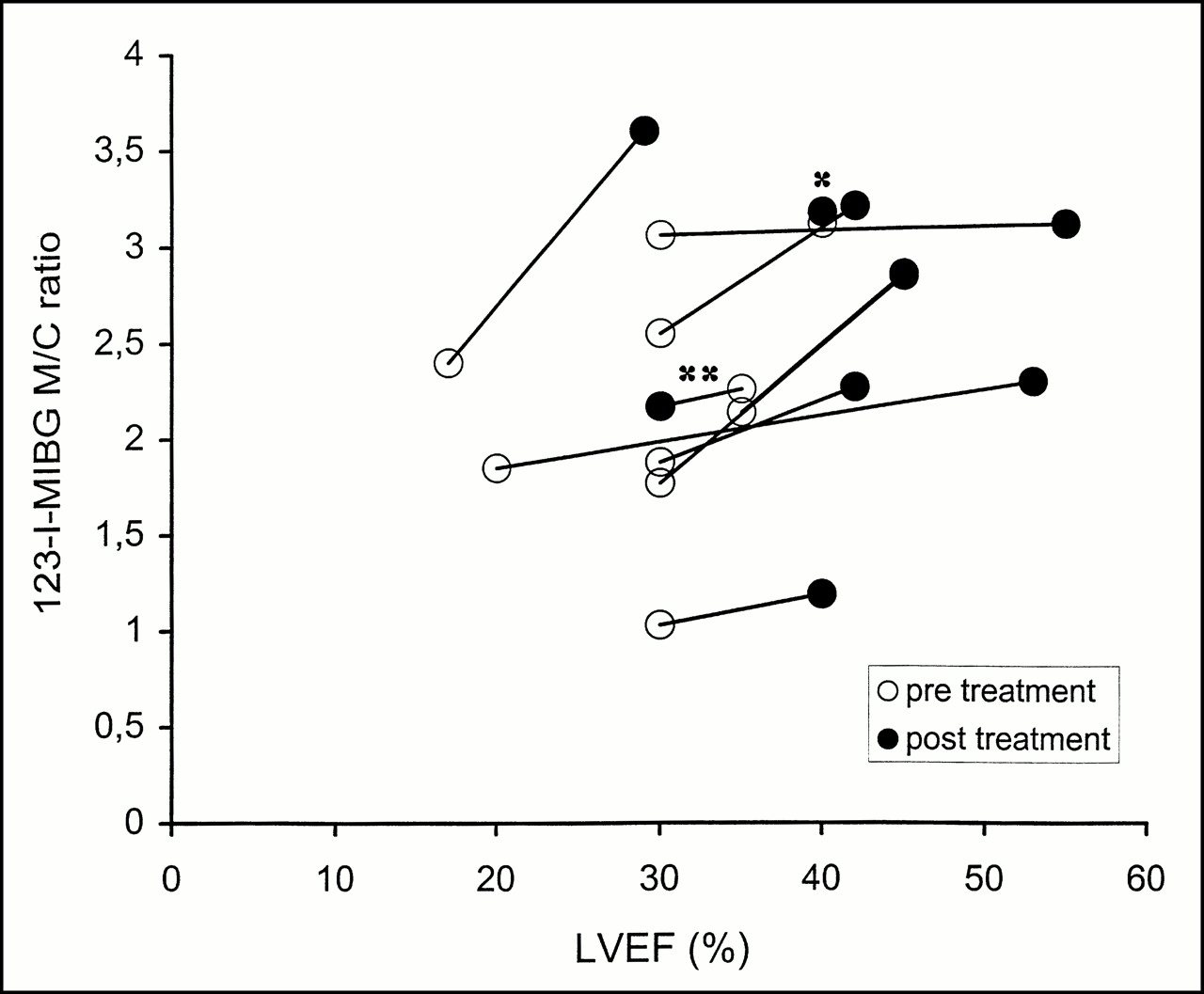
Individual course of LVEF and M/C ratio of patients shows good relationship between changes in LVEF (LVEF at follow-up examination − LVEF at baseline) and 123I-MIBG M/C ratio after 1 y of therapy with β-blockers. In one patient (*), LVEF remained unchanged at 40%, and M/C ratio only increased from 3.12 to 3.18. In another patient (**), LVEF showed small decrease in LVEF from 35% to 30% and in M/C ratio from 2.26 to 2.17. In the remaining eight patients, ascending lines indicate simultaneous increase in LVEF and in M/C ratio.
One-Year Follow-Up Under β-Blocker Therapy
DISCUSSION
In our study, we found an increase in myocardial 123I-MIBG uptake calculated as the M/C ratio, a new cardiac scintigraphic parameter (25), after 1 y of treatment with β-blockers in IDC, even though the number of patients studied was small. In parallel with the clinical and hemodynamic improvement, our findings also indicate a recovery of the cardiac neuronal uptake function associated with the long-term β-blockade. The simultaneous increase in LVEF and myocardial 123I-MIBG uptake reflecting cardiac NE content (12–14) is consistent with catecholamine determinations in endomyocardial biopsies from patients with IDC that showed a positive correlation between myocardial NE and LVEF (32). Our findings confirm the recent study by Toyama et al. (33), who showed that cardiac sympathetic activity assessed by the 123I-MIBG heart-to-mediastinum ratio and total defect score, LVEF, and New York Heart Association functional class improved after 1 y of β-blocker therapy (metoprolol, 30–60 mg/d) in patients with IDC. Moreover, our data agree with the results of Fukuoka et al. (34), who found a decrease in the initially enhanced regional and global 123I-MIBG washout rate considered to be consistent with an increased cardiac sympathetic activity (35–37) after short-term β-blocker therapy with metoprolol for 1 and 3 mo, respectively, in patients with IDC who had a >5% increase in LVEF.
The beneficial effect of long-term β-blocker therapy on the cardiac adrenergic nervous system may be explained by two mechanisms. First, chronic β-blockade may indirectly restore cardiac sympathetic activity by improving the hemodynamics in chronic heart failure (15,20) and thus reduce the cardiac adrenergic tone. Second, the improved cardiac neuronal uptake may be caused by a direct presynaptic effect of the β-blockers and could also be responsible for terminating the stimulation of NE through the postsynaptic β-receptors. This presynaptic effect of the β-blockade is consistent with the already proven upregulation of the β-receptors by metoprolol (20–22) and bisoprolol (21,23). In contrast to the two β1-selective β-blockers, carvedilol does not cause upregulation of the β-receptors (21,22) but causes an adrenergic β-blockade (21) and decreases cardiac adrenergic activity by blocking the β2-receptors (24), leading to a reduced release of NE from the presynaptic nerve endings. This relationship between the cardiac neuronal uptake function and regulation of the β-adrenergic receptors is supported by animal experiments in rats that have hypertensive heart failure (38). Nozawa et al. (38) found a simultaneous decrease in the uptake of myocardial 131I-MIBG and 125I-cyanopindolol, the latter reflecting the density of the β-receptors in the failing heart of Dahl salt-sensitive rats.
Somsen et al. (30) observed a similar increase in myocardial 123I-MIBG uptake after 6 wk of treatment with the ACE inhibitor enalapril in patients with chronic heart failure. Thus, this therapeutic effect of the β-blockers on the cardiac neuronal uptake of NE is not considered to be substance specific but is thought to be associated with hemodynamic improvement and interaction with the cardiac adrenergic activity, two mechanisms that are also known for ACE inhibitors (30,39).
Our data indicate that myocardial 123I-MIBG uptake calculated as the M/C ratio is a useful noninvasive method to evaluate changes in cardiac adrenergic nerve activity under medical treatment. Long-term therapy with metoprolol or bisoprolol, two β1-selective β-blockers, and carvedilol, a nonselective β-blocker with α1-receptor blocking properties, causes an improvement of cardiac neuronal uptake function. This effect is not considered to be a β-blocker–specific effect.
CONCLUSION
We conclude that, concomitantly with a hemodynamic (15–19) and prognostic benefit (17–19), the effectiveness of long-term β-blocker therapy in chronic heart failure associated with IDC is in part based on a recovery of the cardiac adrenergic nervous system at the presynaptic level, as measured by an increased myocardial 123I-MIBG uptake.
Acknowledgments
The authors are most grateful to Kerstin Hollstein for expert technical assistance.
Footnotes
Received Jan. 18, 2000; revision accepted Jun. 20, 2000.
For correspondence or reprints contact: Ulrich Lotze, MD, Klinikum der Friedrich-Schiller-Universität, Innere Medizin III, Erlanger Allee 101, D-07740 Jena, Germany.
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- 123I-MIBG SPECT for Evaluation of Patients with Heart Failure
- Myocardial Sympathetic Innervation and Long-Term Left Ventricular Mechanical Unloading
- Sympathetic Nervous System Activation in Human Heart Failure: Clinical Implications of an Updated Model
- Dobutamine Stress Testing as a Diagnostic Tool for Evaluation of Myocardial Contractile Reserve in Asymptomatic or Mildly Symptomatic Patients With Dilated Cardiomyopathy
- Left ventricular assist device support normalizes left and right ventricular beta-adrenergic pathway properties
- Improvement of Cardiac Sympathetic Innervation by Renal Transplantation
- Sympatholysis and cardiac sympathetic nerve function in the treatment of congestive heart failure
- Effects of Carvedilol on Cardiac Function and Cardiac Adrenergic Neuronal Damage in Rats with Dilated Cardiomyopathy