


Abstract
Chronic renal failure (CRF) patients on dialysis frequently show reduced heart rate variability (HRV), which has been reported to be corrected by renal transplantation. Recently, 123I-metaiodobenzylguanidine (123I-MIBG) scintigraphy has been used to evaluate cardiac sympathetic innervation, and uremic patients often show marked abnormalities of cardiac 123I-MIBG uptake. We investigated whether renal transplantation can improve cardiac 123I-MIBG uptake in patients with CRF on dialysis. Methods: We analyzed time- and frequency-domain measures of 24-h HRV and cardiac 123I-MIBG scintigraphy before and 1–3 mo after renal transplantation in 13 CRF patients on dialysis and in 10 control subjects. Results: Both 24-h HRV and cardiac 123I-MIBG uptake were significantly abnormal in the patients before transplantation compared with the control subjects. After transplantation, 123I-MIBG washout rate from the myocardium significantly decreased from 46% ± 21% to 20% ± 22% (P = 0.006), and the heart-to-mediastinum ratio of 123I-MIBG uptake in the late image significantly increased from 1.74 ± 0.39 to 2.06 ± 0.39 (P = 0.006). On the other hand, HRV measures tended to increase after transplantation but the changes did not reach statistical significance (P > 0.05). Conclusion: Renal transplantation provides the improvement of uremic cardiac sympathetic neuropathy assessed by 123I-MIBG imaging, which may be a more sensitive or at least an earlier marker than HRV.
- kidney transplantation
- metaiodobenzylguanidine
- heart rate variability
- sympathetic nervous system
- autonomic nervous system
The analysis of heart rate variability (HRV) and myocardial 123I-metaiodobenzylguanidine (123I-MIBG) scintigraphy have demonstrated that cardiac autonomic nervous system dysfunction is striking in patients with chronic renal failure (CRF) (1–7) as well as in those with congestive heart failure (8–11). Effective medical therapy has been reported to ameliorate HRV (12–14) and myocardial 123I-MIBG uptake (15–18) in patients with congestive heart failure, although little is known about the recovery process of cardiac autonomic nervous system function after effective treatment against congestive heart failure. On the other hand, several studies (5,19–21) have reported that successful kidney transplantation corrects the reduced HRV in most CRF patients on dialysis, suggesting that uremic cardiac autonomic neuropathy may be reversed by the normalization of renal function. However, it remains unclear whether kidney transplantation can also correct uremic cardiac sympathetic neuropathy assessed with 123I-MIBG imaging. Therefore, this study was designed to examine whether kidney transplantation can improve cardiac sympathetic nervous system function assessed by myocardial 123I-MIBG imaging.
MATERIALS AND METHODS
Subjects
The study performed on 13 patients with CRF on dialysis who were candidates for living related-donor renal transplantation and on 10 control subjects (age, 32 ± 12 y vs. 34 ± 9 y, P = 0.68; female/male, 4/9 vs. 0/10, P = 0.10). None of the control subjects had either a history or a laboratory finding of heart disease, renal dysfunction, hypertension, and diabetes mellitus. The underlying cause of CRF was glomerulonephritis in 10 patients, pyelonephritis in 2, and diabetes mellitus in 1. Ten patients were on antihypertensive drugs, with which blood pressures were well controlled. Of the 10 hypertensive patients, 2 had dilated cardiomyopathy—that is, diffuse hypokinesis of the left ventricle without coronary artery disease—and 1 had prior inferior myocardial infarction with a significant stenosis of the left circumflex artery (Table 1). These 3 patients showed no apparent signs of congestive heart failure during this study. Except for a patient (patient 13, Table 1) on continuous ambulatory peritoneal dialysis, the remaining 12 underwent hemodialysis 3 times weekly. In the 13 CRF patients, HRV analysis and 123I-MIBG scintigraphy were performed before renal transplantation, and the 12 on hemodialysis underwent these studies in the interdialytic days. Both studies were repeated 1–3 mo after transplantation in the 13 CRF patients. The Institutional Review Board on Human Research approved the study protocol, and informed consent was obtained from each patient and control subject.
Patient Characteristics
HRV Analysis
We performed 24-h ambulatory electrocardiographic recording using Marquette 2-channel recorders (Marquette Electronics) on the control subjects and patients. The 24-h recordings were digitized using a Marquette Series 8000 Holter analysis system; then the data were annotated using an automatic arrhythmia detection algorithm (version 5.8). The beat annotations were reviewed by visual inspection to detect and correct any errors in QRS labeling. Using a Marquette HRV program (version 002A), we calculated the 24-h mean of normal RR intervals (mNN, ms) and 4 time-domain measures of HRV: the 24-h SD of normal RR intervals (SDNN, ms), the 24-h SD of 5-min average of normal RR intervals (SDANN, ms), the 24-h average of 5-min SDs of normal RR intervals (SDNN index, ms), and the square root of the mean of the squared differences between adjacent normal RR intervals (rMSSD, ms) (7,22). Moreover, low-frequency (LF) and high-frequency (HF) powers (ms2) were computed for the 0.04- to 0.15-Hz and 0.15- to 0.40-Hz bands, respectively, and their normalized powers and the ratio of LF to HF power (LF/HF ratio) were also calculated (22).
123I-MIBG Scintigraphy
We performed myocardial scintigraphy with 123I-MIBG (Daiichi Radioisotope Laboratory; specific activity, 1.85 GBq/mg [50 mCi/mg]) on the control subjects and patients. Anterior planar images of 180-s acquisition were obtained over the whole thorax 15 min (early) and 150 min (late) after intravenous injection of 123I-MIBG (111 MBq), using a large-field-of-view γ-camera (ZLC 7500; Siemens Gammasonics, Inc.) equipped with a low-energy, all-purpose, parallel-hole collimator and interfaced with a computer system (Scintipac 2400; Shimadzu Corp.) (2,7,22). Energy discrimination was provided by a 20% window centered on the 159-keV photopeak. On these images, mean 123I-MIBG activities per pixel were measured over the heart (H), background (BG) around the heart, and upper mediastinum. The heart-to-mediastinum activity ratio (H/M ratio) was calculated in the early and late images. The washout rate (%) from the heart was calculated using the following formula: ([early H − early BG] − [late H − late BG]) × 100/(early H − early BG).
Statistics
All measures were expressed as mean ± SD. The Fisher exact test was used to determine the significance of differences in rates of occurrence. Comparisons of continuous data between 2 groups were made using an unpaired t test or Mann-Whitney U test. Intragroup comparisons of continuous data were performed by using a paired t test or Wilcoxon signed-rank test. Statistical significance was defined as P < 0.05.
RESULTS
In the patient group, the duration from the first 123I-MIBG study to the transplantation (35 ± 30 d) was similar to that from the first HRV study to the transplantation (38 ± 33 d, P = 0.407). Similarly, the duration from the transplantation to the second 123I-MIBG study (50 ± 16 d) was not significantly different from that to the second HRV study (53 ± 21 d, P = 0.558). Blood pressure measured around 123I-MIBG studies did not significantly change from before to after transplantation (systolic blood pressure, 134 ± 14 mm Hg vs. 136 ± 11 mm Hg, P = 0.983; diastolic blood pressure, 80 ± 13 mm Hg vs. 80 ± 12 mm Hg, P = 0.912), although it was measured without discontinuing antihypertensive drugs.
Patients Before Transplantation Versus Control Subjects
Compared with the control subjects, the patients before renal transplantation had significantly lower early and late H/M ratios of 123I-MIBG with a significantly higher washout rate of 123I-MIBG, as well as significantly lower HRV (SDNN, SDANN, SDNN index, rMSSD, LF power, HF power, and normalized HF power) (Table 2). On the other hand, the mNN, normalized LF power, and LF/HF ratios were not significantly different between the 2 groups. Even when 3 patients with cardiac diseases (patients 1, 7, and 8, Table 1) were excluded from the patient group, the washout rate (41% ± 19%) was significantly higher and the late H/M ratio (1.79 ± 0.40) was significantly lower in the remaining 10 patients than those in the control subjects (P < 0.001), but the early H/M ratio (2.03 ± 0.30) was not significantly different from that of the control subjects (P = 0.054).
Comparisons Between Control Subjects, Patients Before Renal Transplantation, and Patients After Renal Transplantation
Patients Before Versus After Transplantation
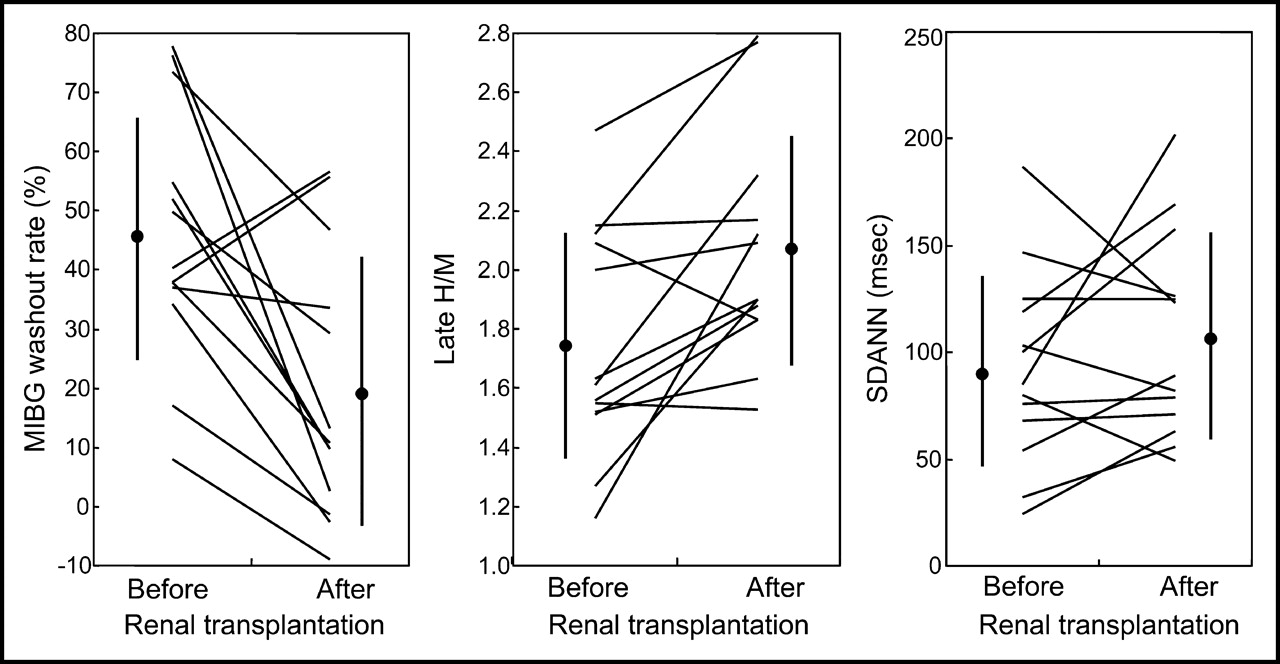
From before to after renal transplantation, the late H/M ratio of 123I-MIBG significantly increased and the washout rate of 123I-MIBG from the heart significantly decreased, whereas the early H/M ratio of 123I-MIBG showed almost no change (Table 2; Fig. 1). On the other hand, the mean of mNN and LF/HF ratio decreased, and those of SDNN, SDANN, and rMSSD increased, but all of these changes did not reach the level of statistical significance and the LF and HF powers, including their normalized values, were similar before and after transplantation (Table 2; Fig. 1). In 10 patients without cardiac diseases (except patients 1, 7, and 8, Table 1), also the late H/M ratio and washout rate of 123I-MIBG significantly changed from before to after transplantation: The late H/M ratio increased from 1.79 ± 0.40 to 2.09 ± 0.43 (P = 0.029) and the washout rate decreased from 41% ± 19% to 16 ± 23% (P = 0.020).

Individual data of 13 CRF patients: 123I-MIBG washout rate, late H/M 123I-MIBG activity ratio, and SDANN before and after renal transplantation. After transplantation, washout rate significantly decreased (P = 0.006), late H/M ratio significantly increased (P = 0.006), and SDANN did not significantly increase (P = 0.24). Data are expressed as mean ± SD.
After renal transplantation, the 123I-MIBG washout rate decreased from 17% to −1% in the patient with diabetes mellitus but no heart disease (patient 10, Table 1) and markedly decreased from 73% to 47% even in the patient with diabetic nephropathy and coronary artery disease (patient 7). Furthermore, the improvement in 123I-MIBG washout rate after transplantation was remarkable in one of the 2 patients with dilated cardiomyopathy (from 78% to 13%, patient 8, Table 1), whereas it was minimal in another (from 37% to 34%, patient 1). On the other hand, the patient on continuous ambulatory peritoneal dialysis showed a marked reduction in 123I-MIBG washout rate (from 76% to 2%, patient 13, Table 1).
Compared with the control subjects, the patients after transplantation had a significantly lower HRV (SDNN, SDANN, SDNN index, rMSSD, LF power, HF power, and normalized HF power), although the difference of means of some HRV measures was smaller between the control subjects and patients after transplantation than that between the control subjects and patients before transplantation (Table 2). Similarly, the washout rate of 123I-MIBG was significantly higher and the early and late H/M ratios were significantly lower in the patients after transplantation than in the control subjects, but both the means of the late H/M ratio and washout rate in the patients after transplantation were intermediate between those in the control subjects and in the patients before transplantation, respectively.
DISCUSSION
This study has demonstrated that kidney transplantation may provide CRF patients on dialysis with dramatic improvement in cardiac sympathetic innervation assessed by myocardial 123I-MIBG kinetics. It has also demonstrated that the improvement may appear at an earlier stage (<3 mo) compared with cardiac autonomic nervous system function assessed by HRV analysis.
Uremic Autonomic Neuropathy and Renal Transplantation
Renal transplantation has been reported to ameliorate uremic autonomic neuropathy (23,24) as well as uremic peripheral neuropathy. Röckel et al. (23) showed that autonomic function such as the pupillary reaction to tyramine was significantly better in 16 patients who had received transplants 3–18 mo earlier than that in 25 hemodialysis patients. Agarwal et al. (24) studied autonomic function tests such as an expiration-to-inspiration ratio of RR interval before and after kidney transplantation in 12 CRF patients and found a significant reversal of all abnormal autonomic tests 12–56 wk after renal transplantation.
HRV and Renal Transplantation
Recently, several investigators (5,19–21) have demonstrated that kidney transplantation improves HRV in most CRF patients on dialysis. In 12 CRF patients, Strano et al. (19) observed that the LF component of short-term HRV significantly increased 8–12 mo after kidney transplantation. Yildiz et al. (20) studied the time-domain and frequency-domain measures of 24-h HRV before and after kidney transplantation in 14 CRF patients and suggested that kidney transplantation may reverse the uremic sympathetic and parasympathetic neuropathy simultaneously and at a relatively early stage (as early as 3–6 mo after transplantation). Furthermore, in 90 CRF patients, Cashion et al. (21) showed that the time- and frequency-domain measures of 24-h HRV partially improved at 6 mo after kidney transplantation and all of them improved by 12 mo, compared with those before transplantation. In 4 hemodialysis patients who underwent kidney transplantation, Rubinger et al. (5) observed that 2 of them showed a dramatic increase in 24-h HRV values (≥3 mo) after transplantation, suggesting that uremic autonomic dysfunction is caused by humoral factors reversed by the normalization of renal function.
These studies (5,19–21) interpreted the LF power and its normalized power as a marker of sympathetic modulation on the sinus node and the LF/HF ratio as a marker of sympathovagal balance or sympathetic modulation. However, it has been reported that both the LF power and its normalized power were not directly related to cardiac norepinephrine spillover measured using 3H-norepinephrine (25). Furthermore, in dogs with healed myocardial infarction, neither the LF power nor its normalized power may reflect changes in cardiac sympathetic activity (26). On the other hand, spectral analysis of simultaneous recordings of muscle sympathetic nerve activity and RR interval in patients with severe congestive heart failure demonstrated that marked sympathetic excitation was associated with reductions in LF power, normalized LF power, and LF/HF ratio (10). Thus, the frequency-domain measures of HRV do not provide a reliable measurement of cardiac sympathetic activity (27), which may explain why the HRV measures, including frequency-domain measures, did not significantly change with kidney transplantation despite the remarkable improvement of 123I-MIBG measures in the present study.
Kidney transplantation can thus improve cardiac autonomic—particularly parasympathetic—nervous system function in CRF patients on dialysis. On the other hand, HRV was not examined earlier than 3 mo after transplantation in these patients, whereas the present study demonstrated that HRV showed only an insignificant increase earlier than 3 mo after transplantation, when the significant change of 123I-MIBG measures appeared. At least, the previous studies do not deny the possibility that kidney transplantation may restore 123I-MIBG measures earlier than HRV measures.
123I-MIBG and Uremic Sympathetic Neuropathy
Previously we reported that the washout rate of 123I-MIBG from the heart was significantly higher in 21 CRF patients on dialysis without diabetes mellitus and coronary artery disease than that in control subjects (2). Similarly, in 11 CRF patients with autonomic dysfunction such as orthostatic hypotension, Miyanaga et al. (3) showed a decreased H/M ratio of 123I-MIBG with rapid cardiac clearance. Moreover, in 44 CRF patients on hemodialysis, we demonstrated heterogeneous myocardial 123I-MIBG distribution, as well as rapid 123I-MIBG clearance from the heart, and found that these 123I-MIBG variables were similar between 26 patients without and 18 with hypertension (7). Although only a few reports (2,3,7) have been published on the utilization of 123I-MIBG scintigraphy for evaluating uremic sympathetic neuropathy, these studies have demonstrated that cardiac sympathetic innervation assessed by myocardial 123I-MIBG scintigraphy may be extremely abnormal in most CRF patients on dialysis.
Earlier studies (2,3,7) and this study have shown that uremic cardiac sympathetic neuropathy may be characterized by rapid 123I-MIBG washout from the heart, for which several mechanisms have been proposed (28). First, a reduction in the number of myocardial sympathetic neurons or in neuronal 123I-MIBG uptake may accelerate myocardial 123I-MIBG clearance, because 123I-MIBG efflux from extraneuronal sites is more rapid than that from intraneuronal sites (29). However, extraneuronal 123I-MIBG uptake may be negligible in the case of 123I-MIBG of a high specific activity (30) and, in humans, extraneuronal 123I-MIBG uptake may account for only a minor part of the total myocardial uptake (31). Second, the rapid clearance may be due to a high plasma concentration of norepinephrine (22,32), but the concentrations in most uremic patients are not high enough to explain rapid 123I-MIBG clearance (7). Furthermore, a plasma concentration of norepinephrine in 123I-MIBG studies did not significantly change from before to after transplantation (405 ± 286 pg/mL vs. 467 ± 249 pg/mL, P = 0.637), although it was measured in only 9 patients. Third, rapid cardiac 123I-MIBG clearance may result from increased 123I-MIBG release from cardiac sympathetic neurons, which may be due to an impairment in vesicular storage (33), due to an increase in nonexocytotic release (34), or due to increased cardiac sympathetic nerve activity (35). Fourth, 123I-MIBG kinetics may reflect something other than sympathetic nerve function; for instance, impaired vesicular storage may partially explain the rapid clearance in CRF patients, since intracytoplasmic but extravesicular 123I-MIBG is released more rapidly than intravesicular 123I-MIBG (29). Thus, the rapid cardiac 123I-MIBG clearance in uremic patients is likely to arise from cardiac sympathetic overactivity with or without impaired vesicular storage.
123I-MIBG and Renal Transplantation
In CRF patients on dialysis, intrarenal accumulation of uremic toxins or of other chemical substances may stimulate renal afferent nerves, along which increased signals may mediate sympathetic overactivity (36). If cardiac sympathetic overactivity is the main mechanism for 123I-MIBG abnormalities in CRF patients on dialysis, the removal of nerve stimulants by kidney transplantation may promptly reduce sympathetic overactivity and, therefore, 123I-MIBG abnormalities. This may partially explain the speed of improvement of 123I-MIBG measures in the present study, and the decrease in 123I-MIBG washout rate and consequent increase in late H/M ratio with no significant change in early H/M ratio after transplantation are consistent with reduction in sympathetic overactivity by transplantation (22,35). If kidney transplantation restores 123I-MIBG measures earlier than HRV measures, the reduction in sympathetic overactivity by transplantation is likely to lead to normalization of sympathovagal balance, which may subsequently cause the improvement in HRV.
Improvement of myocardial 123I-MIBG uptake or clearance has been demonstrated after successful treatment with β-blockers and angiotensin-converting enzyme inhibitors in patients with congestive heart failure. In 18 patients with dilated cardiomyopathy, Merlet et al. (37) observed that the H/M ratio of 123I-MIBG significantly increased from 1.29 ± 0.10 to 1.38 ± 0.17 after 6 mo of therapy with metoprolol. Similarly, in 22 patients with chronic heart failure, Agostini et al. (17) observed that the H/M ratio of 123I-MIBG improved from 1.45 ± 0.23 to 1.70 ± 0.25 after 6 mo of carvedilol treatment. On the other hand, in 19 patients with heart failure, Takeishi et al. (15) showed a significant reduction of myocardial 123I-MIBG washout rate from 38% ± 11% to 30% ± 7% as well as a significant increase of the H/M ratio from 1.63 ± 0.28 to 1.82 ± 0.33 after 9.1 ± 3.0 mo of enalapril therapy. Furthermore, in 10 patients with chronic heart failure, Soeki et al. (16) showed that the H/M ratio of 123I-MIBG significantly increased from 1.86 ± 0.44 to 2.09 ± 0.51 and the washout rate of 123I-MIBG from the heart slightly decreased from 29.1% ± 9.1% to 25.4% ± 7.0% after 3–15 mo (mean, 7 mo) of enalapril treatment. Thus, the rates of improvement in the H/M ratio and washout rate of 123I-MIBG found in the present study may be much greater than those reported in these studies of patients with congestive heart failure. In addition, the correction of occult heart failure after kidney transplantation is unlikely to be one of the main mechanisms for the improvement in 123I-MIBG kinetics by transplantation, because 123I-MIBG abnormalities in patients with no apparent heart failure were too marked to be attributable to occult heart failure and all patients before transplantation, including those with cardiac diseases, were well controlled with dialysis. Moreover, the left ventricular ejection fraction assessed with echocardiography did not significantly change from before to after transplantation (69.5% ± 11.3% vs. 68.7% ± 9.0%, P = 0.676), although it was measured in only 10 patients. However, the involvement of occult heart failure cannot completely be denied until systematic assessment of cardiac function excludes this possibility.
Limitations
In the present study and previous studies (2,3,7), some CRF patients on dialysis showed results of myocardial 123I-MIBG scintigraphy that were comparable with those of healthy control subjects, although most of them showed extremely abnormal values. Similarly, some CRF patients showed HRV results that were comparable with those of control subjects despite a statistically significant difference in mean values. Tamura et al. (38) reported that factors such as hematocrit and duration of hemodialysis were associated with 24-h HRV in hemodialysis patients, but other investigators reported contradictory findings (1,4,7,39). On the other hand, a recent study (40) has demonstrated that increased muscle sympathetic nerve activity is observed in renal transplant recipients with diseased native kidneys, suggesting that afferent impulses from the failing kidneys may cause an increase in efferent sympathetic nerve activity independent of correction of uremia. The clinical implication of abnormal 123I-MIBG results may not be established until factors responsible for sympathetic neuropathy are elucidated in CRF patients on dialysis. Second, not all CRF patients in this study showed the significant improvement of 123I-MIBG measures. There are few reports investigating what is involved in improvement after transplantation. At least one study (5) has reported that kidney transplantation corrects HRV abnormalities in most patients but that HRV may remain suppressed even after transplantation in uremic patients with amyloidosis. Further studies in a large number of patients are needed to determine the clinical and prognostic differences between patients with and without improvement after transplantation. Third, we analyzed frequency-domain measures of HRV in 24-h ambulatory electrocardiographic recordings. Since mechanisms responsible for heart period modulations of a certain frequency are not stationary during long-term recordings, physiologic mechanisms responsible for LF and HF powers cannot be well defined in this study. However, recent studies (5,20,21) that have reported the improvement of HRV after kidney transplantation frequently evaluated 24-h HRV, and we evaluated 24-h HRV for comparison with them.
CONCLUSION
Renal transplantation provides improvement of uremic cardiac sympathetic neuropathy assessed by 123I-MIBG imaging, which may be a more sensitive, or at least an earlier, marker than HRV. The observation of improvement in myocardial 123I-MIBG uptake by renal transplantation may afford excellent insight into the pathophysiology of uremic cardiac sympathetic neuropathy as well as the recovery process of cardiac sympathetic nervous system function.
Acknowledgments
This research was conducted at Hamamatsu University School of Medicine, Hamamatsu, Japan
Footnotes
Received Oct. 10, 2003; revision accepted Jan. 26, 2004.
For correspondence or reprints contact: Chinori Kurata, MD, Yamaha Health Care Center, 10-1 Nakazawa-cho, Hamamatsu 430-8650, Japan.
E-mail: kurata-c{at}post.yamaha.co.jp
REFERENCES
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.