


Abstract
Metaiodobenzylguanidine (MIBG) is a reliable marker for the detection of cardiac adrenergic neuronal damage in heart failure. The cardioprotective properties of carvedilol, a vasodilating β-adrenoceptor–blocking agent, were studied in a rat model of dilated cardiomyopathy after autoimmune myocarditis. Methods: Twenty-eight days after immunization, surviving rats (41/55, or 75%) were divided into 2 groups treated with carvedilol, 2 mg/kg/d (group C, n = 19), or vehicle alone (0.5% methylcellulose, group V, n = 22). After oral administration for 2 mo, heart weight, heart rate, left ventricular end-diastolic pressure (LVEDP), and myocardial fibrosis were measured and compared with those in untreated rats (group N, n = 19). Myocardial uptake of 125I-MIBG (differential absorption ratio) in the left ventricle was measured by autoradiography at 10, 30, or 240 min after tracer injection. Results: Four (18%) of 22 rats in group V died between days 28 and 84 after immunization. None of the rats in group C or N died. Heart weight, heart rate, LVEDP, and area of myocardial fibrosis in group C (1.14 ± 0.04 g, 345 ± 16 beats per minute, 7.6 ± 1.5 mm Hg, and 12% ± 1%) were significantly lower than those in group V (1.34 ± 0.04 g, 389 ± 10 beats per minute, 12.3 ± 1.3 mm Hg, and 31% ± 2%). Although the differential absorption ratio was lower at all time points in group V than in group N, uptake after treatment increased in group C, compared with group V, at 10 min (12.5 ± 1.0 vs. 7.6 ± 0.8, not significant), 30 min (10.1 ± 1.1 vs. 6.3 ± 0.9, not significant), and 240 min (6.5 ± 0.5 vs. 2.5 ± 0.2, P < 0.05). The late washout ratio from myocardial radioactivity between 30 and 240 min in group C was lower than that in group V (36% vs. 60%). Conclusion: These observations indicated that carvedilol has beneficial effects and protects cardiac adrenergic neurons in dilated cardiomyopathy.
Dilated cardiomyopathy, a set of heterogeneous diseases of left ventricular dysfunction of unknown etiology, has a variety of clinical courses and pathologic findings (1,2). One possible cause of dilated cardiomyopathy is myocarditis (3). Two mechanisms by which myocarditis develops into dilated cardiomyopathy have been proposed: One is persistent viral infection, and the other is progressive autoimmune myocardial injury (4,5). Human myocarditis can be classified into lymphocytic myocarditis and giant cell myocarditis according to the histopathologic findings. Giant cell myocarditis is more likely to progress into dilated cardiomyopathy than is lymphocytic myocarditis (4–6). Cells similar to human giant cells were seen in our rat model of myocarditis (7–9).
Carvedilol is a third-generation vasodilating β-blocker (10–13) that has recently been shown to reduce morbidity and mortality in patients with congestive heart failure (14,15). This reduction may occur in part through β- and α1-adrenoceptor blockade, the latter resulting in vasodilation. More important, carvedilol and several of its metabolites are potent antioxidants (16,17).
Radioiodinated metaiodobenzylguanidine (MIBG), an analog of norepinephrine, has been used to evaluate cardiac sympathetic nerve activity (18,19). Reduced myocardial accumulation and enhanced washout of MIBG have been reported in patients with heart failure of various causes (20–23). These abnormal findings have been considered to reflect decreased uptake and accelerated release of norepinephrine from adrenergic nerve endings. The effects of carvedilol on cardiac MIBG kinetics in animal models of heart failure have not been examined rigorously in vivo.
In this study, the effects of long-term treatment with carvedilol on the modification of myocardial damage were examined in a rat model, recently developed by our laboratory, with dilated cardiomyopathy after autoimmune giant cell myocarditis (7–9). We found that carvedilol had beneficial effects and protected cardiac adrenergic neurons in dilated cardiomyopathy.
MATERIALS AND METHODS
Animals and Medication
Seventy-four 9-wk-old male Lewis rats were obtained from Charles River Japan Inc. (Kanagawa, Japan). Cardiac myosin, which was prepared from the ventricular muscle of pig hearts according to a procedure described previously (7–9), was injected into the rats. The morbidity of experimental autoimmune myocarditis was 100% in rats immunized using this protocol (7–9). Nineteen Lewis rats were used as age-matched normal controls (group N).
Rats of the myosin-immunized group became ill and immobile on day 14, and then their activity gradually recovered beginning at the fourth week. Fourteen (25%) of 55 rats in the myosin-immunized group died between days 15 and 28. All hearts from these rats showed extensive myocardial necrosis and massive pericardial effusion. Twenty-eight days after immunization, the 41 rats were divided into 2 groups, which received oral administration of either carvedilol, at 2 mg/kg/d (group C, n = 19), or vehicle alone (0.5% methylcellulose, group V, n = 22) for 2 months. Administration of carvedilol or vehicle was stopped 24 h before hemodynamic and MIBG studies. Throughout the studies, all animals were treated in accordance with the guidelines for animal experimentation of our institute.
Hemodynamic Study
Eight rats from each group were anesthetized with 2% halothane in O2 during surgical procedures to measure the following hemodynamic parameters, and then the concentration was reduced to 0.5% to minimize hemodynamic effects. Mean blood pressure, central venous pressure, peak left ventricular pressure, left ventricular end-diastolic pressure (LVEDP), and the rate of intraventricular pressure rise and decline (±dP/dt) were measured according to a procedure described previously (9). After a stabilization period of 20 min, hemodynamic parameters were measured.
Heart Weight and Histopathology
After measurement of the hemodynamic parameters, the heart was removed and cleaned of the surrounding tissues. The heart weight (HW) was measured, and the ratio of HW to body weight (g/kg) was calculated.
The excised hearts were cut into transverse slices approximately 2 mm thick and fixed in 10% formalin. After embedment in paraffin, several transverse sections were cut from the midventricle slice and stained with the hematoxylin–eosin and azan methods. For the specimens stained with azan at the middle level of both ventricles, the area of myocardial fibrosis was quantified using a color image analyzer (CIA-102; Olympus, Tokyo, Japan), making use of the differences in color (blue fibrotic area as opposed to red myocardium). The results are presented as the ratio of the fibrotic area to the myocardial area (9).
125I-MIBG Imaging and Radioactivity
A dose of 0.8 MBq 125I-MIBG was intravenously injected into 9 rats from each group. Three rats from each group were killed at 10, 30, or 240 min after MIBG administration. The hearts were quickly excised, the apices of heart were stored in γ-counter tubes, and myocardial radioactivity was measured with a well scintillation counter (Autowell Gamma System ARC-2000; Aloka, Tokyo, Japan). The differential absorption ratio is defined as observed radioactive dose × weight of rat/injected radioactive dose × myocardial tissue weight (24).
The nonneuronal radioactivity rapidly decreased by 90 min after MIBG injection (23). Because sequential analysis of myocardial radioactivity in identical rats is impossible with our method, we subtracted the mean value at 30 min from the mean value at 10 min and designated this value as the early washout rate (WR-1) for the nonneuronal compartment. Similarly, the late washout rate (WR-2) for the neuronal compartment was calculated by subtraction of the value at 240 min from that at 30 min.
The hearts were cut into transverse slices approximately 2 mm thick, frozen in optimal-cutting-temperature compound (Tissue-Tek; Sakura, Tokyo, Japan), and stored at −20°C for 3 d. Sequential frozen sections 60 μm thick were cut on a cryostat. Radioactive images of the myocardium were recorded after autoradiography of the myocardial sections for approximately 6 h (BAS 5000; Fuji Film Co., Tokyo, Japan).
Statistical Analysis
Data are presented as the mean ± SEM. Statistical analysis was performed by 1-way ANOVA, followed by the Tukey test. Differences were considered significant at P < 0.05.
RESULTS
Clinical Course
Four (18%) of 22 rats in group V died between days 28 and 84. All hearts from these rats showed extensive myocardial fibrosis and massive pericardial effusion. None of the rats in group C or N died. Although pericardial effusion was observed in most of the rats in group V, little effusion was seen in group C.
Body Weight and HW
The body weight did not differ among the 3 groups. The HW and the ratio of HW to body weight in group V (1.34 ± 0.04 g and 3.32 ± 0.08 g/kg) were significantly greater than those in group N (1.02 ± 0.02 g and 2.45 ± 0.06 g/kg, P < 0.01 for both). The HW and the ratio of HW to body weight were significantly decreased in group C (1.14 ± 0.04 g and 2.88 ± 0.05 g/kg, P < 0.01 for both) compared with group V.
Hemodynamic Parameters
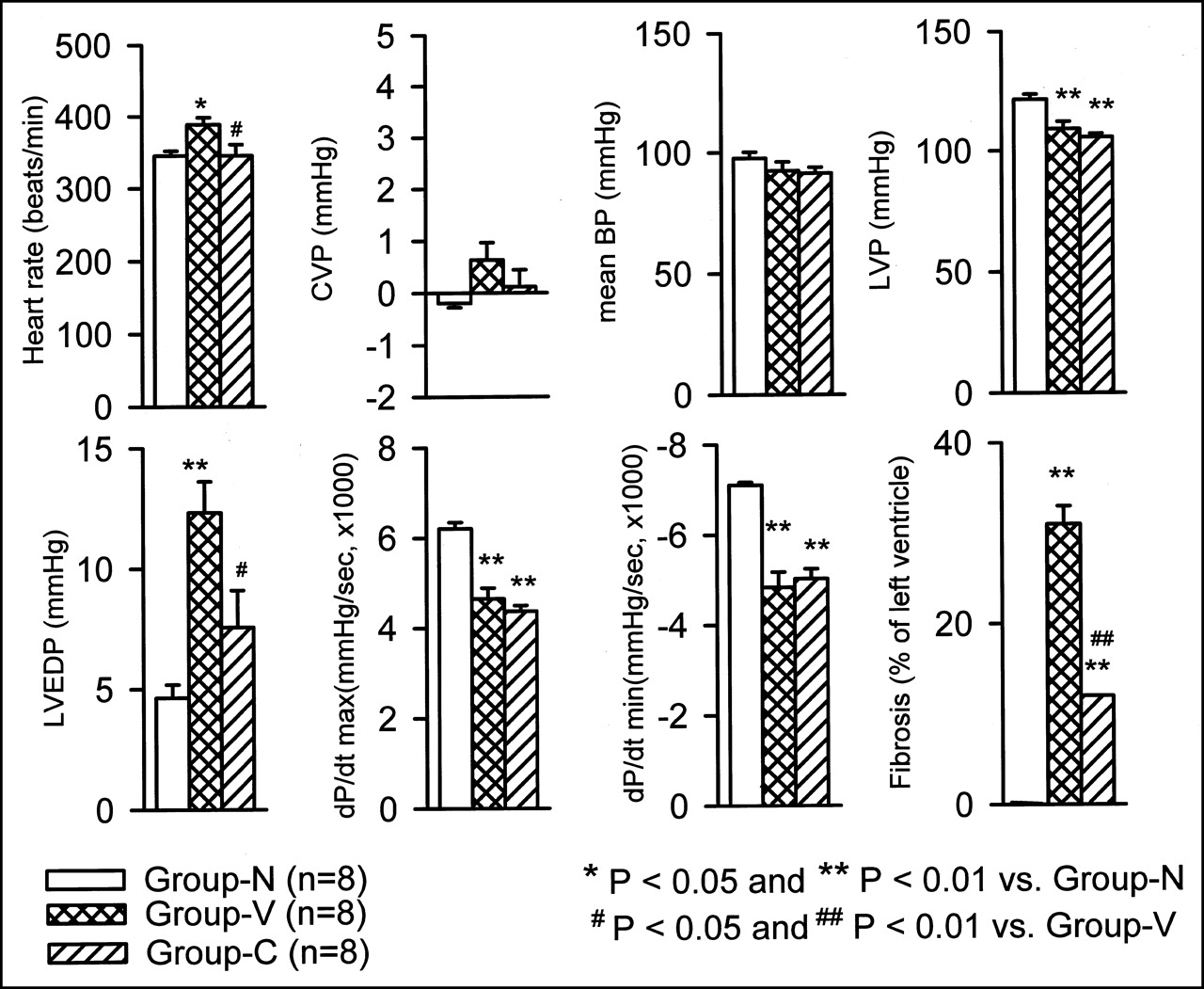
Figure 1 shows the hemodynamic parameters. HR was significantly lower in group C than in group V (345 ± 16 vs. 389 ± 10 beats per minute, P < 0.05). Central venous pressure and mean blood pressure did not differ among the 3 groups. Left ventricular pressure and ±dP/dt in group V (109 ± 3 mm Hg and +4,650 ± 236/−4,830 ± 344 mm Hg/s) were lower than those in group N (121 ± 2 mm Hg and +6205 ± 143/−7,105 ± 61 mm Hg/s, P < 0.01 for both). LVEDP in group V (12.3 ± 1.3 mm Hg) was higher than that in group N (4.6 ± 0.5 mm Hg, P < 0.01). LVEDP was lower in group C (7.6 ± 1.5 mm Hg, P < 0.05) than in group V.

Effects of carvedilol on hemodynamic parameters. Although central venous pressure, mean blood pressure, peak left ventricular pressure, and ±dP/dt did not differ between groups V and C, left ventricular end-diastolic pressure was significantly lower in group C than in group V. BP = blood pressure; CVP = central venous pressure; LVP = left ventricular pressure; max = maximum; min = minimum.
Quantitative Analysis of Myocardial Fibrosis
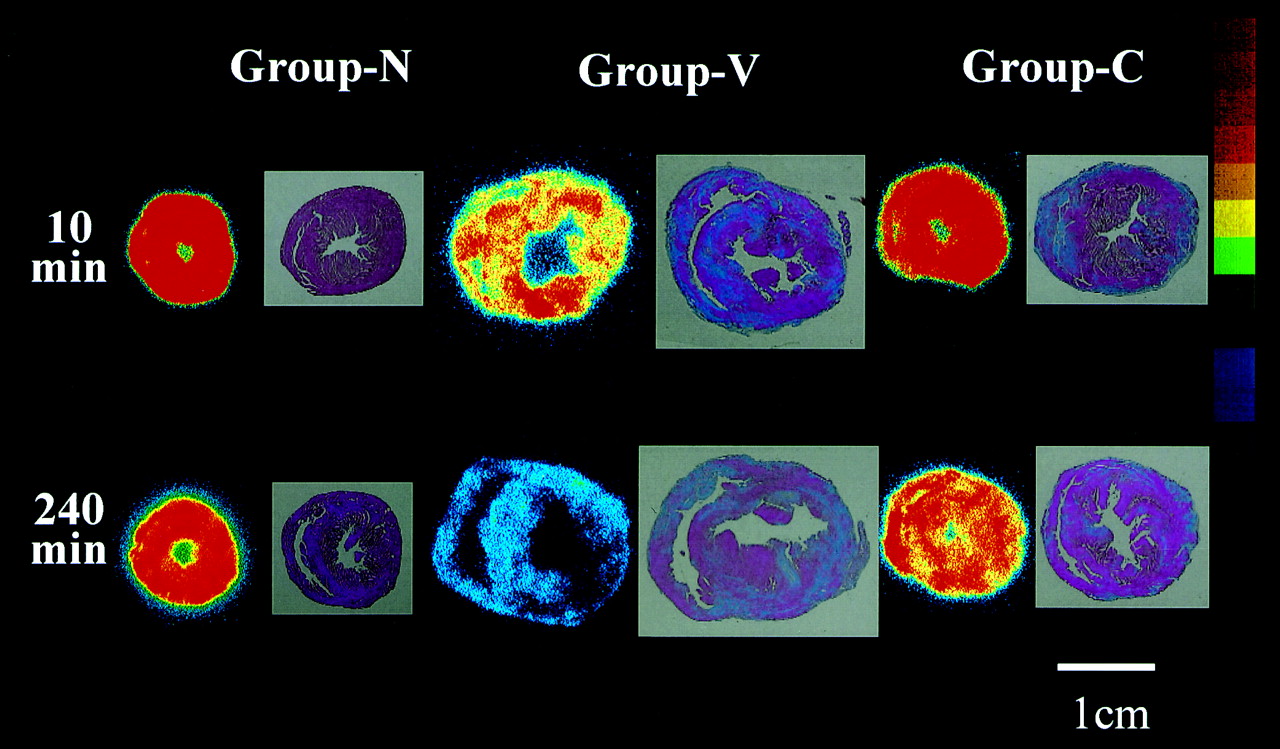
Figure 2 shows representative photographs of thin sections stained by the azan method. Normal hearts showed no fibrosis, but in group V, a blue-stained area indicating fibrosis was clearly observed. The fibrotic area in group C was smaller than that in group V. The area of myocardial fibrosis in group C was smaller than that in group V (12% ± 1% vs. 31% ± 2%, P < 0.01).

Effects of carvedilol on myocardial fibrosis, heart size, and myocardial uptake of 125I-MIBG. Figures are representative of each group. Blue (azan staining) indicates fibrosis determined by histology. Red and blue indicate high and low myocardial uptake of MIBG determined by scintigraphy. MIBG uptake in rats with dilated cardiomyopathy was decreased not only in area of fibrosis but also in intact area. Top shows MIBG scintigram at 10 min after tracer injection. Bottom shows MIBG scintigram at 240 min after tracer injection.
125I-MIBG Imaging and Radioactivity
As shown in Figure 2 and Table 1, the myocardial uptake of MIBG was higher in group N than in group V at 10, 30, and 240 min. Although the differential absorption ratio at 240 min was significantly decreased and WR-2 was increased in group V compared with group N, both were improved in group C.
Differential Absorption Ratio and Washout Ratio of MIBG
DISCUSSION
In this study, we examined the effects of carvedilol treatment on progression of heart failure and on myocardial uptake and washout of 125I-MIBG in a rat model of dilated cardiomyopathy induced by autoimmune myocarditis. We found that carvedilol reduced HW, myocardial fibrosis, LVEDP, and myocardial washout of MIBG.
Human dilated cardiomyopathy is thought to be caused by a variety of factors. Therefore, clinical courses and pathologic findings in dilated cardiomyopathy are not uniform. Cardiac myosin-induced autoimmune myocarditis, which is not exclusively related to viral infection, develops into a clinicopathologic state similar to dilated cardiomyopathy in the chronic phase (7–9). Thus, the current results provide some information on the effectiveness of carvedilol treatment against dilated cardiomyopathy.
Carvedilol is the only β-blocker that blocks β1-, β2-, and α1-receptors without producing an intrinsic sympathomimetic effect, such as an increase in cardiac norepinephrine level or upregulation of β-receptors (1–3). Hence, the use of this drug is associated with more complete antagonism of the sympathetic nervous system than is associated with other β-blockers. Although LVEDP and heart rate decreased in group C, mean blood pressure, left ventricular pressure, and ±dP/dt did not change between groups C and V in this study. The reason that ±dP/dt did not change may have been the negative inotropic action of carvedilol. The reason that mean blood pressure and left ventricular pressure did not change may have been the α-blocking action of carvedilol. Although massive pericardial effusion and increased LVEDP were observed in group V, little effusion and low LVEDP were observed in group C. These indicate that the cardiac function of rats with dilated cardiomyopathy, like that of humans with dilated cardiomyopathy, improved but did not return to normal through treatment with carvedilol. Regardless, the survival rate was increased and LVEDP was decreased in group C, indicating that carvedilol had beneficial effects in this animal model.
In addition to these actions as an adrenoceptor blocker, carvedilol has antioxidant and antiproliferative effects (3–5). These actions may play important roles in preventing the progressive loss of myocardial cells that is characteristic of a failing heart. In this study, the area of myocardial fibrosis after administration of carvedilol was smaller than that in the untreated control group, and carvedilol also reduced HW. The beneficial effects of carvedilol were very likely caused by its antioxidant and antiproliferative impact.
The sympathetic nervous system plays an important role in the development and progression of heart failure. The myocardial norepinephrine content decreases with progression of heart failure. A close relationship between myocardial norepinephrine content determined from transvenous myocardial biopsy and left ventricular function is found in dilated cardiomyopathy. Because MIBG shares many transport properties with norepinephrine, MIBG can be used to assess cardiac adrenergic nervous system dysfunction in human heart failure. Cardiac imaging with MIBG has been shown to be more sensitive for the prognosis of patients with heart failure than is evaluation of mechanical function, that is, left ventricular ejection fraction (22). This is probably because the decrease in MIBG uptake on delayed imaging (3 or 4 h after MIBG injection) reflects not only the sympathetic denervation but also the abnormal increase in washout caused by sympathetic acceleration (19,25). Thus, the measurement of MIBG washout can be used as a sensitive index to detect increased sympathetic activity in various cardiac diseases.
We were able to detect increased sympathetic tone in this model of heart failure by measuring the neuronal washout of MIBG. However, we cannot ignore the nonneuronal washout of MIBG in animal studies (26). Washout of MIBG in the early phase has been reported to be mainly nonneuronal, and this nonneuronal washout is largely over by as early as 90 min in rats (23,27,28). Therefore, we focused on the early-phase (WR-1; between 10 and 30 min) and late-phase (WR-2; between 30 and 240 min) washout rates of MIBG uptake to evaluate cardiac nonneuronal and neuronal washout, respectively. In this study, myocardial uptake of MIBG at 240 min was decreased and WR-2 was increased in rats with heart failure. Interestingly, these parameters were improved in the carvedilol treatment group. The improvement in neuronal function by carvedilol can be explained by 2 mechanisms. First, carvedilol may directly improve cardiac neuronal uptake of norepinephrine. This local effect may result in an increased exposure of myocytes to norepinephrine and a subsequent downregulation of myocardial β-receptors in rats and patients with heart failure. Second, hemodynamics were improved in the carvedilol group. This systemic effect may indirectly result in a reduced cardiac neuronal release and a restoration of neuronal uptake of norepinephrine.
As shown in this study, increased sympathetic tone correlates with the development and progression of heart failure, and evaluation of the late-phase MIBG washout is easier than the established methods and can be repeated during disease progression (19,22,25). This technique may be useful in assessing serial changes in sympathetic tone in patients with dilated cardiomyopathy.
CONCLUSION
Carvedilol increased survival rate and cardiac function and decreased myocardial fibrosis and HW in rats with dilated cardiomyopathy. Additionally, carvedilol reduced MIBG release and thus lowered cardiac sympathetic nerve activity. MIBG was helpful in evaluating the therapeutic effects of carvedilol on cardiac sympathetic nervous system activity.
Acknowledgments
This study was supported by grant 13670750 from the Ministry of Education, Science, Sports and Culture of Japan and a grant from the Promotion and Mutual Aid Corporation for Private Schools of Japan.
Footnotes
Received May 21, 2001; revision accepted Sep. 21, 2001.
For correspondence or reprints contact: Kenichi Watanabe, MD, Department of Clinical Pharmacology, Niigata College of Pharmacy, Kamisinei-cho, Niigata 950-2081, Japan.
E-mail: watanabe{at}niigata-pharm.ac.jp
REFERENCES
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Amiodarone Improves Cardiac Sympathetic Nerve Function to Hold Norepinephrine in the Heart, Prevents Left Ventricular Remodeling, and Improves Cardiac Function in Rat Dilated Cardiomyopathy
- Effect of spironolactone on cardiacsympathetic nerve activity and left ventricular remodeling in patients with dilated cardiomyopathy
- Myocardial Adrenergic Dysinnervation in Dilated Cardiomyopathy: Cornerstone or Epiphenomenon?