


Abstract
In patients with progressive metastatic (or recurrent) differentiated thyroid carcinoma (DTC) who do not respond to radioiodine therapy or do not show uptake on radioiodine scintigraphy, treatment options are few. Because these tumors may express somatostatin receptors, peptide receptor radionuclide therapy might be effective. We evaluated the therapeutic efficacy of the radiolabeled somatostatin analog 177Lu-1,4,7,10-tetraazacyclododecane-N,N′,N″,N‴-tetraacetic acid0 (DOTA), Tyr3-octreotate (177Lu-DOTATATE) in patients with DTC. The uptake of radioactivity in tumors was also studied in relation to treatment outcome. Methods: Five patients with DTC (3 with Hürthle cell thyroid carcinoma [HCTC], 1 with papillary thyroid carcinoma [PTC], and 1 with follicular thyroid carcinoma [FTC]) were treated with 22.4–30.1 GBq of 177Lu-DOTATATE. Response to therapy was evaluated with CT. Uptake on 177Lu-DOTATATE scintigraphy (24 h after treatment), expressed as percentage of injected dose, was compared with uptake on pretherapy 111In-octreotide scintigraphy (24 h after injection). Results: After the last treatment with 177Lu-DOTATATE, 1 patient with HCTC had stable disease as a maximum response, 1 patient with HCTC had minor remission (tumor shrinkage between 25% and 50%), and 1 patient with HCTC had partial remission (shrinkage ≥50%). The responses in PTC and FTC were stable disease and progressive disease, respectively. A decrease in serum thyroglobulin level was found in patients with HCTC. Patients with minor and partial remissions had the highest 177Lu-DOTATATE-to-111In-diethylenetriamine pentaacetic acid0-octreotide (111In-octreotide) uptake ratios (3.2 and 2.4, respectively) whereas the other patients had uptake ratios smaller than 1.5. Conclusion: 177Lu-DOTATATE therapy can be effective in patients with progressive DTC who have no therapeutic options and sufficient uptake of 111In-octreotide in tumor lesions as shown on 111In-octreotide scintigraphy. This finding is especially important in patients with HCTC, because they cannot benefit from radioiodine therapy because of non-iodine-avid lesions at diagnosis.
Standard therapy in patients with differentiated (follicular and papillary) thyroid carcinoma (DTC) involves total or near-total thyroidectomy, followed by ablation of the thyroid remnant with 131I. Although long-term prognosis with this combination of surgery and radioiodine therapy is generally quite good, tumor recurrences occur in about 20% of patients, sometimes decades after initial therapy (1,2). Follow-up in these patients is based on a combination of serum thyroglobulin (Tg) monitoring and radioiodine whole-body scans (WBSs). Whenever recurrence or metastatic disease is evident on the WBS, patients are retreated with radioiodine. However, in 20%–30% of these patients, additional 131I therapy is not effective because of the lack of radioiodine uptake in tumors (3,4). In addition, Hürthle cell thyroid carcinomas (HCTCs), which are assigned to the group of follicular thyroid carcinoma (FTC), are known to rarely take up iodine, even at the time of diagnosis (5).
Alternative treatments in patients with no uptake of radioiodine are few. Dedifferentiation is associated with a worse prognosis, which is largely because these patients cannot be treated with radioiodine (6). Patients with iodine-concentrating pulmonary metastases have a 5-y survival rate of 60% compared with 30% for patients with tumors that do not concentrate radioiodine (4,7). Therefore, any effective therapy would be welcome. As most of these patients have widespread metastatic disease, surgery is not an option. External beam radiotherapy can provide only regional control of localized recurrences. Studies on the effectiveness of chemotherapy have been disappointing (8,9).
In patients with elevated serum thyroglobulin levels with no evidence of disease on radioiodine scintigraphy, scintigraphy with the somatostatin analog 111In-diethylenetriaminepentaacetic acid0 (DTPA0)-octreotide (111In-octreotide, Octreoscan; Mallinckrodt) can be an alternative imaging modality. Several reports have demonstrated uptake of 111In-octreotide in metastatic or recurrent disease in the majority of these patients (10–13). As a consequence, the use of high doses of radiolabeled somatostatin analogs as targeted therapy in peptide receptor radionuclide therapy (PRRT) has become the focus of major interest as an alternative therapy. Patients with progressive DTC and tumor uptake on 111In-octreotide scintigraphy have been treated with various radiolabeled somatostatin analogs, including 111In-octreotide, 90Y-1,4,7,10-tetraazacyclododecane-N,N′,N″,N‴-tetraacetic acid0 (DOTA)-d-Phe1,Tyr3-octreotide (90Y-DOTATOC), and 90Y-DOTA-lanreotide (14–17). In this study, we report the results of treatment with the novel radiolabeled somatostatin analog 177Lu-DOTA0,Tyr3-octreotate (177Lu-DOTATATE) in 5 patients with DTC.
MATERIALS AND METHODS
Patients
Five patients with recurrent or metastatic differentiated thyroid carcinoma were treated with 177Lu-DOTATATE. Patient characteristics are summarized in Table 1. All patients had visible tumor uptake on 111In-octreotide scintigraphy before therapy. None of the patients had been treated with other radiolabeled somatostatin analogs in the past. All patients were on thyroid-stimulating hormone (TSH) suppressive thyroxin therapy. Prerequisites for treatment were: hemoglobin ≥5.5 mmol/L; white blood cell count ≥2 × 109/L; platelets ≥75 × 109/L; creatinine ≤150 μmol/L; Karnofsky performance status ≥50. All patients gave written informed consent to participate in the study, which was approved by the medical ethical committee of the hospital.
Patient Characteristics
Imaging
111In-octreotide.
Planar spot imaging was performed with a double-head γ-camera (Prism 2000XP; Philips Medical Systems). Windows with a 20% width were centered over each of the 2 111In photon peaks (245 and 172 keV). Fifteen-minute spot images were obtained 24 h after injection of 222 MBq of 111In-octreotide. A standard with a known aliquot of the injected dose was measured for dosimetry.
177Lu-DOTATATE.
Planar spot images of the chest, neck, and upper abdomen were obtained 24 h after injection of the therapeutic dose of 177Lu-DOTATATE. Upper abdomen images were also obtained on 2 occasions in the following days for kidney dosimetry. Counts (20% window width) from the 208 keV γ-peak were collected. The acquisition time was 15 or 7.5 min/view. For dosimetry, a standard with a known aliquot of the injected dose was also measured.
Therapy
DOTATATE was obtained from Mallinckrodt. 177LuCl3 was obtained from NRG and the Missouri University Research Reactor, distributed by IDB. 177Lu-DOTATATE was prepared as described in a previous publication (18). Three milligrams of granisetron were injected intravenously and an infusion of amino acids (2.5% lysine and 2.5% arginine in 1 L 0.9% NaCl at 250 mL/h) was started 30 min before administration of the radiopharmaceutical and lasting up to 3.5 h afterward. The radiopharmaceutical was coadministered through a second pump system. Treatment doses of 1.9 and 3.7 GBq were injected over 20 min and those of 5.6 GBq and 7.4 GBq were injected over 30 min. The interval between treatments varied from 6 to 15 wk. The number of treatments varied from 3 to 8. Some patients were included in the early phase of therapy with 177Lu-DOTATATE, when dose escalation was among the objectives. As a result of the time schedule, completion of all treatments varied from 3 to 12 mo for any individual. All patients were allowed to receive up to a cumulative dose of 30 GBq, which corresponded to a calculated bone marrow dose of 2 Gy, except in those individual cases in which kidney dosimetry indicated less (maximum allowed kidney dose was 23 Gy).
Routine hematology, liver and kidney function tests, hormone measurements, and serum tumor markers were measured 1 wk before each therapy, as well as at follow-up visits. CT or MR imaging was performed within 3 mo before the first therapy, and 6–8 wk, 3 mo, and 6 mo after the last treatment. Thereafter follow-up continued every 6 mo.
In Vivo Measurements
CT- or MR-assessed tumor measurements were scored according to the following criteria: progressive disease (PD), increase in measurable tumor mass volume ≥25%; stable disease (SD), tumor mass volume increase or decrease ≤25%; minor remission (MRe), decrease of tumor mass volume between 25% and 50%; and partial remission (PR), decrease of tumor mass volume ≥50%. Time to progression (TTP) was defined as the time interval between the first treatment and the earliest date of disease progression based on CT or MR imaging measurements. The amount of uptake on pretherapy 111In-octreotide and posttherapy 177Lu-DOTATATE scintigraphy was scored visually on planar images on a 4-point scale according to criteria previously described by Krenning et al. (19): lower than (grade 1), equal to (grade 2), or greater than (grade 3) normal liver tissue; and grade 4, higher than normal spleen/kidney uptake.
RESULTS
Five patients with metastatic DTC (3 with HCTC, 1 with papillary thyroid carcinoma [PTC], and 1 with FTC) were treated with 22.4–30.1 GBq of 177Lu-DOTATATE. The patients were either negative on 131I scintigraphy after therapy or proven unresponsive to 131I therapy. Metastatic disease was present in all patients based on conventional imaging (CT/MR imaging or sonagraphy), pathologic uptake of 111In-octreotide, and elevated serum Tg levels. Tumor response after therapy was monitored by CT/MR imaging and serum Tg levels (Table 2).
Results of 177Lu-DOTATATE Therapy
Patient 1 was diagnosed in 1995 with PTC with supraclavicular metastases. Initial treatment consisted of total thyroidectomy followed by radioiodine ablation. In April 1996, the patient was treated with radioiodine for recurrent disease. Because of a newly developed sarcomatoid carcinoma of the vocal chord, a total laryngectomy and bilateral nodal neck dissection was performed later that year. Lymph nodes were positive for DTC, and a third dose of 131I was given. In 1998, a fourth treatment of 131I was given because of a third recurrence. However, no uptake of 131I was visible on posttherapy scintigraphy. In contrast, 111In-octreotide scintigraphy showed uptake in the mediastinum. Subsequently, 177Lu-DOTATATE therapy was initiated. Eight treatments were given with a cumulative treatment dose of 25.7 GBq, which resulted in SD. TTP was documented 18 mo after the first treatment, with gradually increasing serum Tg levels. Thereafter, CT measurements showed PD. Four years after the first treatment, the patient died of the disease.
Patient 2 was diagnosed in 1990 with FTC. Within 1 y after total thyroidectomy and ablation, CT assessment showed lung metastases, which were treated with a therapeutic dose of 131I. However, posttherapy 131I scintigraphy did not reveal any uptake in tumor. Therefore, additional treatment consisted of local external radiotherapy and chemotherapy with adriamycine. However, the patient had PD, and her clinical condition worsened. In 2000, tumor progression led to airway obstruction, which was complicated with pneumonia and severe stridor, necessitating emergency tracheostomy. At that time, 111In-octreotide scintigraphy revealed numerous lesions in the chest, and, subsequently, 177Lu-DOTATATE therapy was started. Three treatments of 177Lu-DOTATATE with a total dose of 22.4 GBq could not stop tumor progression, which was obvious from both symptomatology and increased serum Tg levels. Two weeks after the last therapy, the patient died of tumor progression.
Patient 3 was diagnosed with HCTC and had undergone total thyroidectomy combined with a neck dissection. However, complete removal of the tumor mass was not possible because of intraoperative identification of tumor growth into the trachea. Surgery was followed by radioiodine therapy. Eighteen months later, an ultrasound of the neck revealed continued growth of the (para)tracheal mass, which did not accumulate any 123I. 111In-octreotide scintigraphy, however, showed uptake in the lower neck region. 177Lu-DOTATATE therapy was initiated, and the patient received 8 treatments with a cumulative dose of 27.4 GBq. Six months after the last therapy, the patient was found to be in MRe. Two years later progression was demonstrated. After an initial rise in serum Tg level after treatment, this decreased to a nadir of 46.6 μg/L, which reflected decrease of tumor mass volume (Fig. 1A).
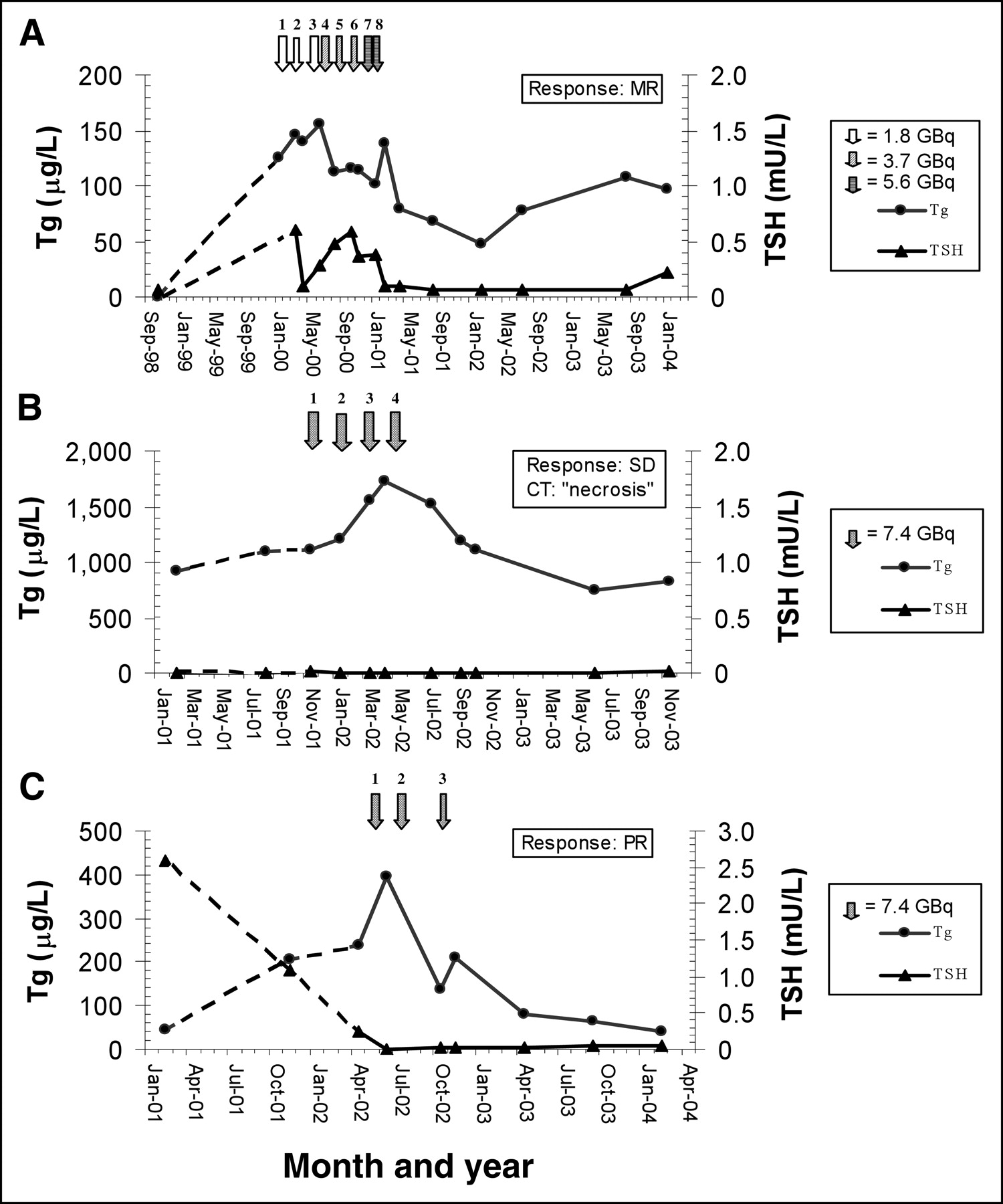
Time course of serum Tg and TSH levels in patient 3, 4, and 5 treated with 177Lu-DOTATATE. Broken lines represent pretherapy levels.
Patient 4 initially had a left-sided hemithyroidectomy for HCTC. Sixteen years later, 3 lung metastases were detected, and she had a right-sided hemithyroidectomy followed by 131I therapy with 3.7 GBq, after which the serum Tg levels decreased from 150 to 18 μg/L. However, no change in tumor size was found. One year later no accumulation during 123I scintigraphy was found. Despite the absence of radioiodine uptake, she was retreated with 3.7 GBq of 131I, with no effect on tumor mass or serum Tg levels. In 1999, the serum Tg level increased to 507 μg/L and 5.5 GBq of 131I was administered. Despite a positive lesion in the right upper lobe of the lung on 131I scintigraphy after therapy, again no effect was found. Because of positive lesions detected on 111In-octreotide scintigraphy, the patient received 4 treatments with a total dose of 30.1 GBq 177Lu-DOTATATE. The serum Tg levels, which were measured before each treatment, increased up to a maximum of 1,730 μg/L. After the last treatment, the serum Tg levels decreased, with a nadir of 746 μg/L 14 mo later (Fig. 1B). On CT, no difference in tumor size was found. However, the radiology report mentioned an inhomogeneous aspect that suggested tumor necrosis.
Patient 5 with an HCTC was diagnosed in 1997 and subsequently underwent a total thyroidectomy followed by radioiodine ablation therapy. Because of local recurrences in the surgical bed and low cervical region, she was retreated with radioiodine in 2000 and 2001. Persistent uptake near the jugulum was seen on 131I scintigraphy after therapy. In 2001, additional imaging was performed because of persistent elevated serum Tg levels and progressive pain in the left leg. In addition to the neck lesion seen on 131I scintigraphy, both 18F-FDG PET and MRI showed lesions in the spine (L3 and L5-S1). Lack of radioiodine accumulation in the latter lesions suggested dedifferentiation, and, therefore, external radiation was given. Because of the growth of the neck lesion, which compressed the trachea, the patient developed a stridor. 111In-octreotide scintigraphy showed uptake in all tumor lesions as previously seen on 18F-FDG PET and MRI. The patient received 3 treatments with a cumulative dose of 22.7 GBq of 177Lu-DOTATATE. After the second treatment, serum Tg levels began to decrease (Fig. 1C). At the same time, the CT scan showed regression of the tracheal lesion with a shrinkage of 50% 12 mo after the last therapy.
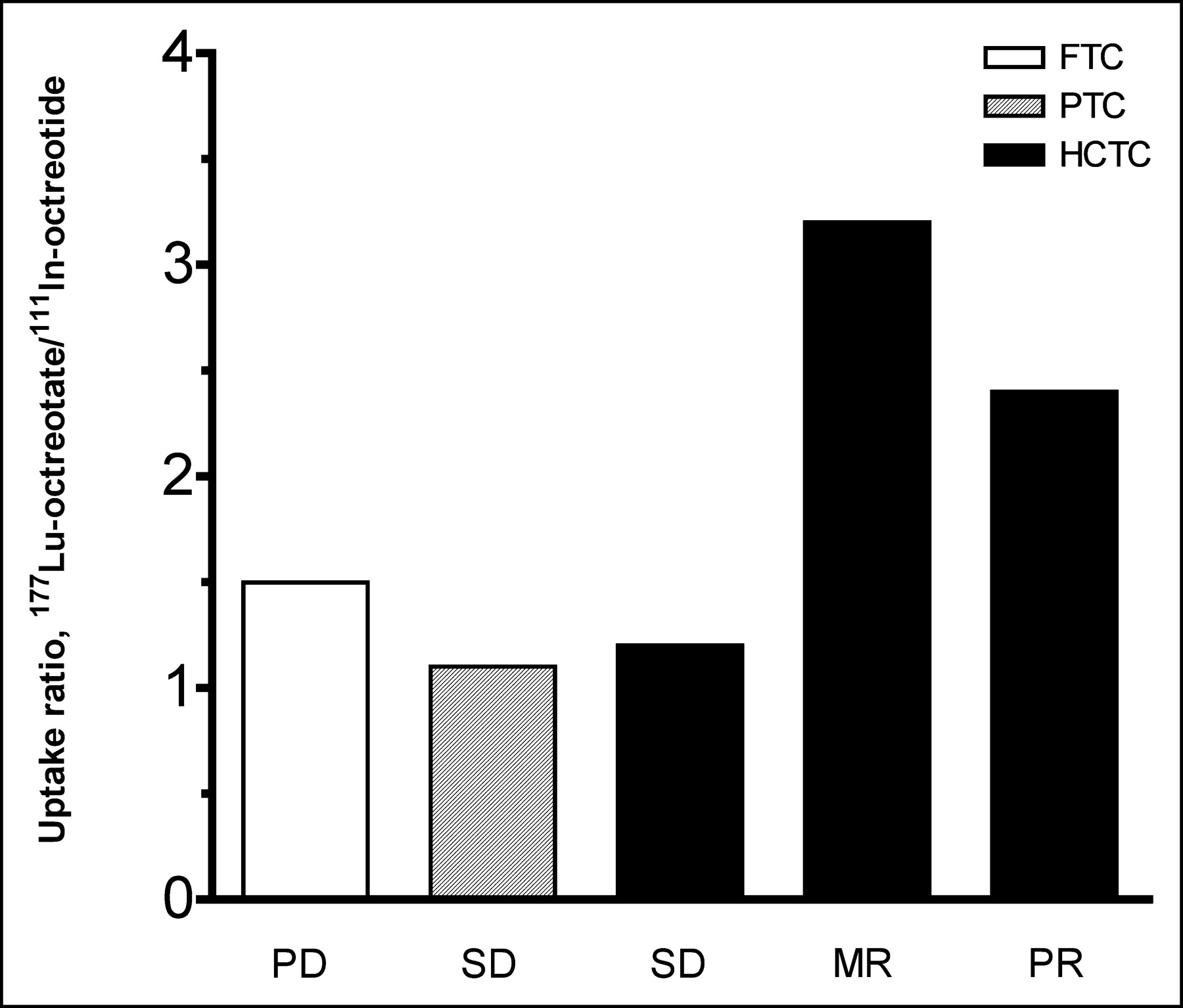
A comparison between pretherapy 111In-octreotide and posttherapy 177Lu-DOTATATE scintigraphy in patients 1 and 3 is shown in Figure 2. In patient 1, the uptake of both somatostatin analogs was about the same. In contrast, more uptake was shown in the tracheal lesion of patient 3 on 177Lu-DOTATATE scintigraphy than on 111In-octreotide scintigraphy. Calculated 177Lu-DOTATATE/111In-octreotide tumor uptake ratios in the tumor lesions of all patients varied from 1.1 to 3.2. Two patients with HCTC, in whom tumor shrinkage was demonstrated, had the highest ratios (Fig. 3).

Images comparing pretherapy 111In-octreotide scintigraphy (A) and posttherapy 177Lu-DOTATATE scintigraphy at 24 h (B). Top row shows corresponding images of tumor sites in patient 1 with metastatic PTC. Bottom row shows corresponding images of patient 3 with HCTC.

Ratios of 177Lu-DOTATATE and 111In-octreotide uptake in tumor sites. Uptake was expressed as percentage of administered dose. Note differences in uptake between patients with HCTC who responded with MRe and PR and those who did not respond with tumor shrinkage.
DISCUSSION
Therapeutic options in patients with recurrent or metastatic DTC that cannot concentrate radioiodine are limited. Also, the loss of iodine-trapping ability, or dedifferentiation, is associated with a more aggressive behavior (6).
In this paper we describe the results of therapy with 177Lu-DOTATATE in 5 patients with DTC, who had no other treatment available. CT-assessed tumor shrinkage was found in 2 patients with HCTC. Concomitantly, a decrease in serum Tg levels was observed in both patients. In the other patient with HCTC the serum Tg levels decreased significantly, whereas CT-assessed tumor volume did not change. However, the aspect of the lesions changed, which suggested necrosis. Disease stabilization was achieved in one patient with clearly progressive PTC before therapy, whereas the patient with FTC progressed despite treatment. These results suggest that in some patients with DTC, who have no treatment options left, 177Lu-DOTATATE therapy can be effective.
The reason to treat these patients with 177Lu-DOTATATE, was found in the successful treatment with this compound in patients with somatostatin receptor–positive gastroenteropancreatic (GEP) tumors. Objective tumor shrinkage was demonstrated in up to 38% of patients (20). In addition, reports in which other somatostatin analogs were labeled with different radionuclides, such as 111In or 90Y, showed similar therapeutic benefit in patients with GEP tumors (16,17,21,22). Apart from GEP tumors, other results of therapy in patients with DTC were reported (Table 3). Patients with DTC were treated because they had progressive disease, somatostatin receptor–positive lesions on 111In-octreotide scintigraphy, and no other treatment option available.
Peptide Receptor Radionuclide Therapy in 58 Patients With Differentiated Thyroid Carcinoma
Krenning et al. (19) reported the first 2 DTC patients treated with radiolabeled somatostatin analogs. Both had PTC and were treated with 111In-octreotide, which was available for therapy. One patient, who had a total cumulative dose of at least 20 GBq, showed disease stabilization, whereas the other patient, who had received <20 GBq, was lost to follow-up. In a review that summarized the use of 111In-octreotide therapy in a total of 50 patients in a single institution, 40 patients were evaluated after cumulative doses of at least 20 GBq up to 160 GBq. Within this group, 5 patients had DTC, including 4 patients with PTC and 1 with FTC (17). Four patients were progressive despite treatment, whereas 1 patient, who was reported earlier to have SD for some time, ultimately progressed. In a recent report, 11 patients with progressive iodine nonresponsive thyroid carcinoma were treated with high, fixed doses of 111In-octreotide (23). Nine patients were evaluable, because 2 patients died during follow-up of causes unrelated to their disease. Six months after the last therapy, 4 patients had SD and 5 patients had PD. Stablilization of disease was accompanied with a stable Tg level, whereas 3 out of a group of 5 patients with radiologic progression had increasing levels of Tg. Interestingly, the mean Tg value in the latter group was higher than in the group with stabilization of disease (mean Tg value 180,432 vs. 275 μg/L). It was suggested that low Tg values could be used as selection criteria for 111In-octreotide therapy.
Waldherr et al. (15) treated 8 DTC patients (3 FTC, 4 PTC, and 1 anaplastic thyroid carcinoma) with 90Y-DOTATOC. Two patients, who were treated with 9.1 and 14.8 GBq, had SD and documented TTP of 8 mo, whereas the other patients had PD. Chinol et al. (21) also used 90Y-DOTATOC to treat 2 patients with PTC. Unfortunately, the efficacy of therapy in these 2 patients was difficult to determine from this study, because results were presented as the effect of treatment in the whole group of somatostatin receptor (SSTR) positive tumors. In the Multicenter Analysis of a Universal Receptor Imaging and Treatment Initiative, a European Study (MAURITIUS) trial reported by Virgolini et al. (16), 25 patients with radioiodine negative thyroid carcinoma were treated with 0.9–7.0 GBq of the somatostatin analog 90Y-DOTALAN. Three patients had regressive disease (>25% reduction of tumor size), 11 had SD, and 11 had PD. In a very recent report, 5 patients with DTC were treated with 90Y-DOTATOC with a dose range of 5.6 GBq to 7.4 GBq (24). The authors reported that patients who responded under this therapy regimen had SD for at least 5 mo. Especially interesting in comparison with our results is the report by Gorges et al. (14), who described the courses of disease of the first 3 patients with HCTC treated with 90Y-DOTATOC (total dose, 1.7–9.6 GBq). The patient with the highest dose responded with a period of SD of 9 mo, whereas the other 2 patients had progressive disease despite treatment. They concluded that the protocol was not ideal, because tumor radiation dose was suboptimal.
To draw conclusions from all the studies concerning the therapeutic efficacy of PRRT in patients with non-radioiodine-avid or unresponsive thyroid cancer is difficult. The number of treated patients in the reported studies was low. Furthermore, different radiolabeled somatostatin analogs were used with individually variable administered doses. Clearly, PRRT in DTC seems to be less effective than in GEP neuroendocrine tumors.
One reason for this difference in efficacy might be the expression profile of SSTR subtypes by tumors. Reubi et al. (25), who intensively studied the SSTR subtype profile of numerous human tumors, reported a predominance of SSTR2 or SSTR1 in GEP tumors. In contrast, in vitro studies with thyroid cancer cell line monolayers and xenografts showed a predominant expression of SSTR3 and SSTR5, whereas SSTR2 mRNA was only faintly detectable (26). In another report, in which the receptor subtype expression in biopsied DTC tumor tissue was investigated by Northern Blot analyses, SSTR1, SSTR3, SSTR4, and SSTR5 were expressed in all tumors, whereas SSTR2 was not detected in any FTC or PTC tumors. In line with these observations, Forssell-Aronsson et al. (27) also demonstrated that the highest tumor-to-background ratio and expression of high-affinity SSTR2, was found in medullary thyroid carcinoma and Hürthle cell neoplasia. In the latter, the expression of SSTR2 was irregular. These findings suggest that the SSTR subtype expression profile found in DTC cells is different and more variable than that in GEP tumors.
Most radiolabeled somatostatin analogs available for therapy share the high binding affinity for the SSTR2 receptor. It was reported that, in comparison with DTPA0,Tyr3-octreotide, DTPA0,Tyr3-octreotate showed improved binding to SSTR-positive tissues in animal experiments (28). Furthermore, the somatostatin analog DOTATATE has a 9-fold higher affinity for the SSTR2 than does DOTATOC, whereas the affinity to SSTR3 and SSTR5 were found to be lower (29). In line with the higher affinity for the SSTR2, our biodistribution studies on 111In-octreotide and 177Lu-DOTATATE scintigraphy, reported previously, showed a 3- to 4-fold higher tumor uptake in 4 out of 5 patients (18). The presence of SSTR subtypes other than SSTR2 was suggested as an explanation for equivalent tumor uptake of both somatostatin analogs in 1 patient with PTC, who is also described in this article (patient 1). Interestingly, the 177Lu-DOTATATE/111In-octreotide uptake ratios calculated in the 5 patients demonstrated that the 2 HCTC patients with the highest uptake ratios responded with tumor shrinkage, whereas the others had ratios <1.5. Thus, in patients with PTC or FTC with tumors that probably exhibit a different and variable SSTR expression profile with predominantly SSTR5 and SSTR3 instead of SSTR2, there is no clear advantage of Tyr3-octreotate over Tyr3-octreotide.
For the better tumor targeting and increase in uptake required for better therapeutic efficacy of PRRT in DTC, SSTR subtype-specific analogs with higher affinity for SSTR3 and SSTR5 are necessary. Most promising is the recent study by Wild et al. (30), who reported the first preclinical data on 111In- and 90Y-labeled DOTA-1-Nal3-octreotide (DOTA-NOC), which has, apart from high affinity to SSTR2, a favorable affinity for SSTR3 and SSTR5. In addition, they briefly mentioned excellent images of thyroid cancer patients in clinical studies with [111In]DOTA-NOC. It was assumed that DOTA-NOC labeled with either 90Y or 177Lu will have similar favorable properties, so that it might become available for therapy in patients with DTC in the near future.
In our opinion, the best candidates for PRRT with 177Lu-DOTATATE in non-iodine-avid metastatic and radioiodine unresponsive DTC are patients with HCTC. The combination of a large percentage of HCTC patients with positive lesions on 111In-octreotide scintigraphy, relatively high tumor uptake of 177Lu-DOTATATE compared with PTC or FTC, and the favorable outcomes observed in our patients suggest that especially in these patients 177Lu-DOTATATE may induce tumor shrinkage or prolonged disease stabilization.
Acknowledgments
The authors wish to thank all supporting personnel in the Department of Nuclear Medicine at the Erasmus Medical Center (Rotterdam, The Netherlands) for their expert help and effort.
Footnotes
Received June 7, 2004; revision accepted Oct. 21, 2004.
For correspondence or reprints contact: Jaap J.M. Teunissen, MD, Department of Nuclear Medicine, Erasmus Medical Center, Dr. Molewaterplein 40, 3015 GD, Rotterdam, The Netherlands.
E-mail: j.teunissen{at}erasmusmc.nl
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Clinical History of the Theranostic Radionuclide Approach to Neuroendocrine Tumors and Other Types of Cancer: Historical Review Based on an Interview of Eric P. Krenning by Rachel Levine
- 68Ga-DOTATOC PET/CT in Patients with Iodine- and 18F-FDG-Negative Differentiated Thyroid Carcinoma and Elevated Serum Thyroglobulin
- A New Theranostic Paradigm for Advanced Thyroid Cancer
- In Vitro Evaluation of Targeted Antisense 177Lu Radiotherapy
- Effects of Therapy with [177Lu-DOTA0, Tyr3]Octreotate in Patients with Paraganglioma, Meningioma, Small Cell Lung Carcinoma, and Melanoma