


Abstract
The somatostatin analog diethylenetriaminepentaacetic acid (DTPA)-d-Phe1-octreotide labeled with 111In has been applied extensively for diagnosis of neuroendocrine tumors using SPECT or planar scintigraphy. However, the spatial resolution of planar scintigraphy and SPECT prohibits imaging of small tumors, and the quantification accuracy of both methods is limited. Methods: We developed a method to prepare the positron-emitting radiopharmaceutical 110mIn-DTPA-d-Phe1-octreotide based on a commercially available kit. Phantom studies were done to investigate and compare the performance of 110mIn PET and 111In SPECT. A clinical imaging study using 110mIn-DTPA-d-Phe1-octreotide and PET was done to investigate the application of this radiopharmaceutical. Results: An almost 3-fold better resolution and much better quantitative capabilities were found for 110mIn PET than for 111In SPECT. The clinical imaging study demonstrated the potential use of 110mIn-octreotide in PET to image tumors and quantify radioactivity uptake in humans using 110mIn-DTPA-d-Phe1-octreotide. Conclusion: PET with 110mIn-DTPA-d-Phe1-octreotide greatly improved detection of small tumors and offers a possibility of more accurate quantification of tumor uptake than can be obtained with 111In-DTPA-d-Phe1-octreotide and SPECT.
Today, about 50% of all malignant tumors can be successfully treated with surgery, external radiotherapy, and chemotherapy. The remainder are mainly tumors that have extensively spread and have metastatic growth. Further improvement in treatment requires effective methods to seek and eradicate spread tumor cells. A promising approach for both diagnostics and therapy is the targeting of tumor-specific cell-surface structures with radiopharmaceuticals. Receptors for the neuropeptide somatostatin are overexpressed in several neuroendocrine tumors, making these receptors potential targets for radionuclide diagnostics and therapy (1,2). Somatostatin is unstable in vivo and is therefore not suitable for application to diagnostic imaging. Octreotide, an octapeptide analog of somatostatin, has a longer biologic half-life, which makes it more suitable for labeling and imaging. Octreotide can be radioiodinated (3) or labeled with the radiometals 111In, 67Ga, 64Cu, 90Y, and 161Tb (4–8). A kit for preparation of 111In-diethylenetriaminepentaacetic acid (DTPA)-d-Phe1-octreotide, or 111In-octreotide, is commercially available (OctreoScan; Mallinckrodt Medical BV, Petten, The Netherlands), and in recent years, 111In-octreotide has been used extensively in the diagnosis of hormone-producing tumors using planar gamma camera imaging and SPECT (9–13).
The spatial resolution obtainable with single-photon imaging limits its capability to detect, for example, gastroenteropancreatic tumors. These tumors are frequently small (<1 cm) and difficult to find even with 111In-octreotide scintigraphy (14,15). For this reason, PET, which has better spatial resolution, has been suggested as a possible way to improve detection of small lesions (16). Octreotide has been labeled with the positron-emitting nuclides 18F, 68Ga, and 86Y (8,17). We propose the use of a short-lived positron-emitting isotope of indium, 110mIn (half-life, 69 min), for labeling DTPA-d-Phe1-octreotide using the OctreoScan kit. There is a lack of consensus about the use of the designation “m” in this isotope and in the other 110In isotope (half-life, 4.9 h), but in this article, we follow the notation of Chu SYF et al. (18). Because of its short half-life, 110mIn is suitable for the labeling of short peptides with fast kinetics, such as octreotide. 110mIn-octreotide PET should be able to provide quantitative information about receptor kinetics and concentrations with better temporal and spatial resolution than can 111In-octreotide SPECT. 110mIn can be produced either from a 110Sn/110mIn generator or using the 110Cd(p,n)110mIn nuclear reaction on low-energy cyclotrons, which are available at many PET centers (19,20). Table 1 shows decay properties for 110mIn and 111In.
Main Decay Radiation of 110mIn and 111In
The aim of this study was to establish a technique for labeling DTPA-d-Phe1-octreotide with 110mIn, to compare the performance of 110mIn PET and 111In SPECT, and to demonstrate the use of 110mIn-octreotide in a clinical imaging study. The Ethics Committee and the Isotope Committee of the Uppsala University Medical Faculty approved the patient study, and informed consent was obtained from the patient.
MATERIALS AND METHODS
Production of Radiopharmaceuticals
110mIn was produced by irradiating an enriched 110Cd target using the 110Cd(p,n)110mIn nuclear reaction according to a previously described method (20). In a typical production run, 4 isotopically enriched 110Cd foils (thickness, about 50 μm; Teknowledge UK Ltd., London, U.K.) were irradiated on a water-cooled copper backing at the MC17 cyclotron (Scanditronix AB, Uppsala, Sweden) at Uppsala University PET Centre. An aluminum energy degrader with a thickness of 0.18 g/cm2 was used to decrease the energy of incident protons to 11.8 MeV (the threshold energy for formation of 109Cd). Beam currents of up to 15 μA were applied for the production of 110mIn.
For separation, the irradiated foils were heated at 306°C during 30 min in an argon atmosphere. After cooling, the surface of the foils was etched with 5 mL of 0.05 mol/L HCl. Each foil was then rinsed with 20 mL of deionized water and 20 mL of absolute ethanol and, after drying, was used for further irradiation. The acidic solution of 110mIn was evaporated almost to dryness and then was redissolved in 0.6 mL of 4 mol/L HCl and passed through a column with anion-exchange resin (AG 1 × 8, 200–400 mesh; Bio-Rad Laboratories, Hercules, CA) preequilibrated with 4 mol/L HCl. The 110mIn was eluted with 5 mL of 0.05 mol/L HCl, and the eluate was evaporated to dryness. 110mIn was redissolved in 400 μL of 0.02 mol/L HCl and used for further labeling.
110mIn-octreotide was produced using the OctreoScan kit. The labeling of octreotide was performed using a procedure similar to that recommended by the manufacturer for production of 111In-octreotide. 110mIn (500 MBq in 0.02 mol/L HCl) was added to a vial containing 10 μg DTPA-d-Phe1-octreotide. After 30 min of incubation, the content of the vial was diluted with saline. Finally, the product was sterilized by filtration with a 0.22-μm sterile filter (Millipore, Molsheim, France). Analysis of the radiopharmaceuticals was performed using instant thin-layer chromatography (ITLC-SG; Gelman Instrument Co., Ann Arbor, MI), with sodium citrate (0.1 mol/L, pH 5) as the mobile phase. Complementary analysis using Sep-Pak C-18 (Waters, Milford, MA) and size-exclusion high-performance liquid chromatography was also performed. Details on this step were published previously (21). Hydrochloric acid of pro analysi quality (Merck KGaA, Darmstadt, Germany) was used to prepare the solution. All solutions were prepared with ultrapure water (18 MΩ/cm3 resistance). All vessels and glassware used in separations were rinsed with concentrated HCl, kept overnight filled with a mixture of ethanol and 3 mol/L HCl (1:1), and rinsed 6 times with ultrapure water before use. Radioactivity was measured with an ultrapure germanium detector (EG&G Ortec, Oak Ridge, TN) online with an 8,192-channel personal computer–based multichannel analyzer (The Nucleus, Oak Ridge, TN). The detector was calibrated for energy and efficiency with a standard 152Eu source of known absolute radioactivity. Dead-time losses were always less than 10% during measurements.
Tomographs
The PET measurements were made with a whole-body scanner (4096+ WB; General Electric Medical Systems, Uppsala, Sweden). This tomograph consists of 8 detector rings, each having 512 bismuth germanate detectors separated by nonremovable septa, producing 15 image planes. The axial field of view (FOV) is 10.4 cm, and the transverse FOV is 55.5 cm. The detection energy threshold is 300 keV. Attenuation can be corrected either analytically, by contour finding or by definition of an ellipse contour, or on the basis of a transmission scan with a rotating 68Ge/68Ga pin source. Before reconstruction by filtered backprojection, corrections for dead time, random coincidences, normalization, scatter, and attenuation were applied. Scatter was corrected using the convolution-subtraction method (22). All images were reconstructed using a 4.2-mm Hann filter and a pixel size of 2 mm.
For SPECT measurements, a dual-head system (DynaScan; Picker International, Cleveland, OH) containing two 36 × 36 cm planar NaI detectors applied with medium-energy general-purpose collimators was used. For all phantom measurements, the distance between detectors was kept constant at 46 cm, the minimum possible distance for the resolution phantom. Counts were acquired at 64 angles during 20 s to 2 min for each angle, depending on counting rate. Detection energy windows were set at 20% around the 111In peaks at 171 and 245 keV. The data acquired in these windows were corrected for scattered radiation using a triple-energy window with data from two 3-keV-wide windows located just below the 171-keV window and centrally between the 171 and 245 keV windows. After scatter correction, the data acquired in both windows were summed. Attenuation was corrected analytically using an ellipse-shaped contour and a linear attenuation correction coefficient of 0.14 cm−1. Projections were filtered using a Metz filter of order 13 before reconstruction by filtered backprojection to 64 image planes of 128 × 128 pixels each, a pixel size of 2.9 mm, and a slice separation of 5.8 mm.
Performance Measurements
Spatial Resolution.
A 5 × 45 × 20 cm (height × length × width) polythene block containing a 1-mm-diameter catheter crossing the block at 0, 5, 10, and 20 cm from its center was placed centrally in the FOV of the scanner. Polythene was chosen because of its 0.97 g/cm3 density, which resembles normal tissue. The catheter was filled with a solution containing approximately 30 MBq of 110mIn or 111In, and a 15-min (PET) or 32-min (SPECT) emission scan was made. Transverse resolution was calculated as the mean of the full widths at half maximum of a gaussian fit to a vertical and horizontal profile through the peaks in each image plane. Scatter and attenuation corrections were omitted in the SPECT measurement.
Correction Accuracy.
A 20-cm-diameter cylindric polystyrene phantom filled with a solution of approximately 40 MBq of 110mIn or 111In was placed in the center of the FOV of the scanner. The phantom contained a 5-cm-diameter cylinder filled with cold water and placed 5 cm above the phantom axis. A 1-h (PET) or 2.1-h (SPECT) emission scan was made. Images were reconstructed both with and without scatter correction. The residual correction error was calculated by dividing the measured radioactivity concentration in a 3-cm-diameter volume of interest through each image plane (PET), or in 15 central image planes (SPECT) inside the cold insert, by the mean radioactivity concentration in six 3-cm-diameter volumes of interest in the same planes in the radioactive solution.
Recovery.
A water-filled phantom containing 6 hot spheres with diameters ranging from 11 to 38 mm was placed centrally in the FOV of the scanner. The spheres were filled with a solution containing approximately 1 MBq/mL 110mIn or 111In, and a 20-min emission scan was made. Analytic attenuation correction was done. After reconstruction, 10-mm-diameter regions of interest (ROIs) were drawn in each sphere. Because of the large sphere size relative to the spatial resolution, the recovery in the largest sphere was assumed to be 1 for PET. Sphere recovery was calculated by dividing the measured radioactivity concentration in each sphere by the radioactivity concentration in the largest sphere (PET) or the known radioactivity concentration (SPECT).
Clinical Imaging Study
Imaging.
To 1 patient who had a small-intestine-carcinoma metastasis in the upper thorax, approximately 175 MBq of 111In-octreotide were administered. A standard clinical SPECT measurement (64 angles, 40 s per angle) was made 24 h after administration. Images were reconstructed as described above, without scatter correction. To the same patient, 140 MBq of 110mIn-octreotide were administered intravenously. PET emission scans of the upper thorax were made during the first 50 min after administration. The scan lengths were 1 min (0–5 min after administration), 3 min (5–20 min after administration), and 5 min (20–50 min after administration). The patient was then moved, and two 10-min scans of the lower part of the body, including the kidneys, were made. The patient was moved back to the initial position, and 3 more scans of 10 min each were made at 102, 112, and 122 min after administration. Before all 3 scanning series, a 10-min transmission scan was made for attenuation correction and to verify proper positioning. Images were reconstructed as described above, with scatter correction.
Kinetics.
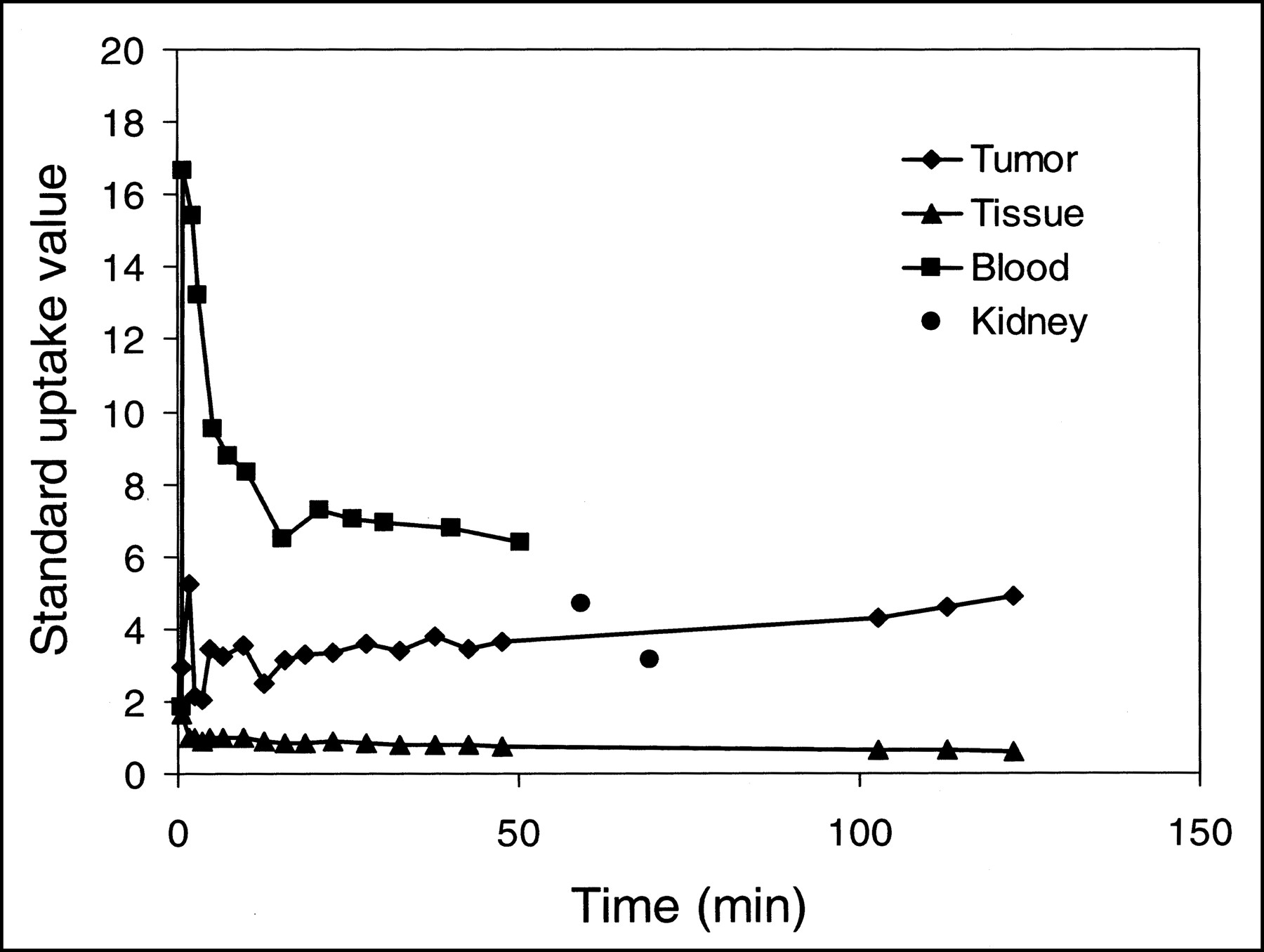
Thirteen blood samples were taken during the first 50 min after administration of 110mIn-octreotide, and the blood radioactivity was measured in well counters. The image data in the last 3 PET emission scans were summed before ROIs were drawn. In the summation image, an ROI was drawn around the central tumor at 50% of the maximum radioactivity concentration and was transferred to all individual images. The same procedure was followed for the 16 scans from the first 50 min. Two circular ROIs with radii of 25 mm were drawn at 50 mm from the left and right sides of the tumor to determine the background radioactivity concentration in tissue. All these ROIs were drawn in the 3 planes where the tumor was most visible, and the ROIs in these 3 planes were linked to create volumes of interest for better statistics. ROIs around the kidneys were also drawn at 50% of the maximum radioactivity concentration. The standard uptake values of the central tumor, the blood, and the kidneys were calculated by dividing the tissue radioactivity concentration by the injected radioactivity per kilogram of body weight.
RESULTS
Production of Radiopharmaceuticals
A 1-h-long irradiation of the stacked foil target produced 110mIn in excess of 20 GBq. Decay-corrected separation yields were 63%–68%. Labeling, which was performed according to the OctreoScan instructions, gave yields of 93%–98%, as confirmed by independent measurements with instant thin-layer chromatography, Sep-Pak, and high-performance liquid chromatography.
Performance Measurements
Figure 1 shows the spatial resolution as an average of the radial and tangential resolutions in all slices for 110mIn PET and in five 5.8-mm-thick slices for 111In SPECT. The residual correction error in the reconstructed images, after attenuation correction in PET and SPECT, was approximately 15% in PET and 31% in SPECT. After scatter correction, the residual correction error was approximately 6% in PET and 26% in SPECT. Figure 2 gives the recovery functions. Recovery in the largest sphere was 76% in SPECT, and recovery in a 20-mm-diameter sphere was 29% for 111In SPECT, compared with 83% for 110mIn PET and 93% for 18F PET.
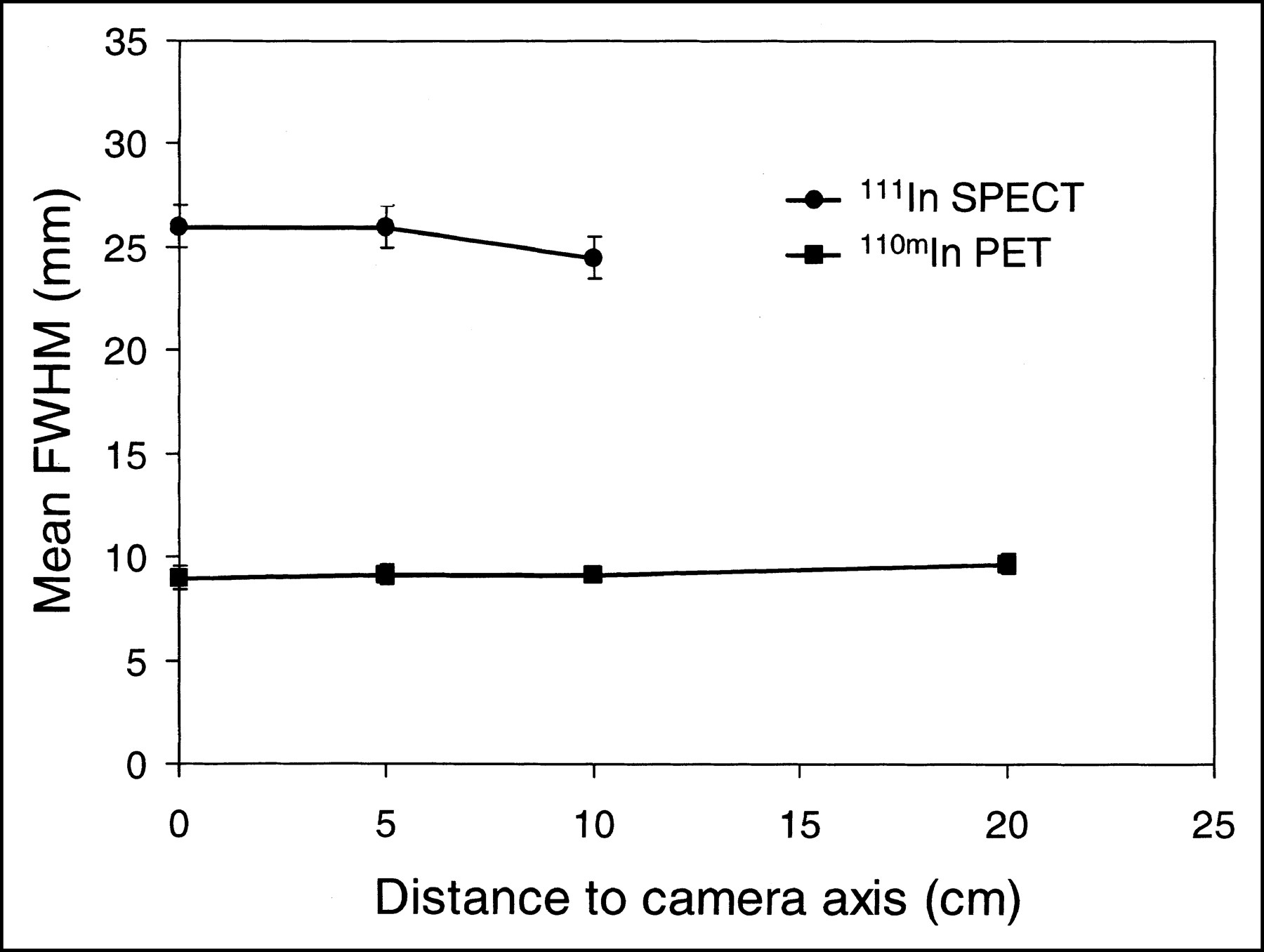
Spatial resolution in PET and SPECT with 110mIn and 111In, respectively. Just outside FOV in SPECT measurement was 20-cm point. FWHM = full width at half maximum.
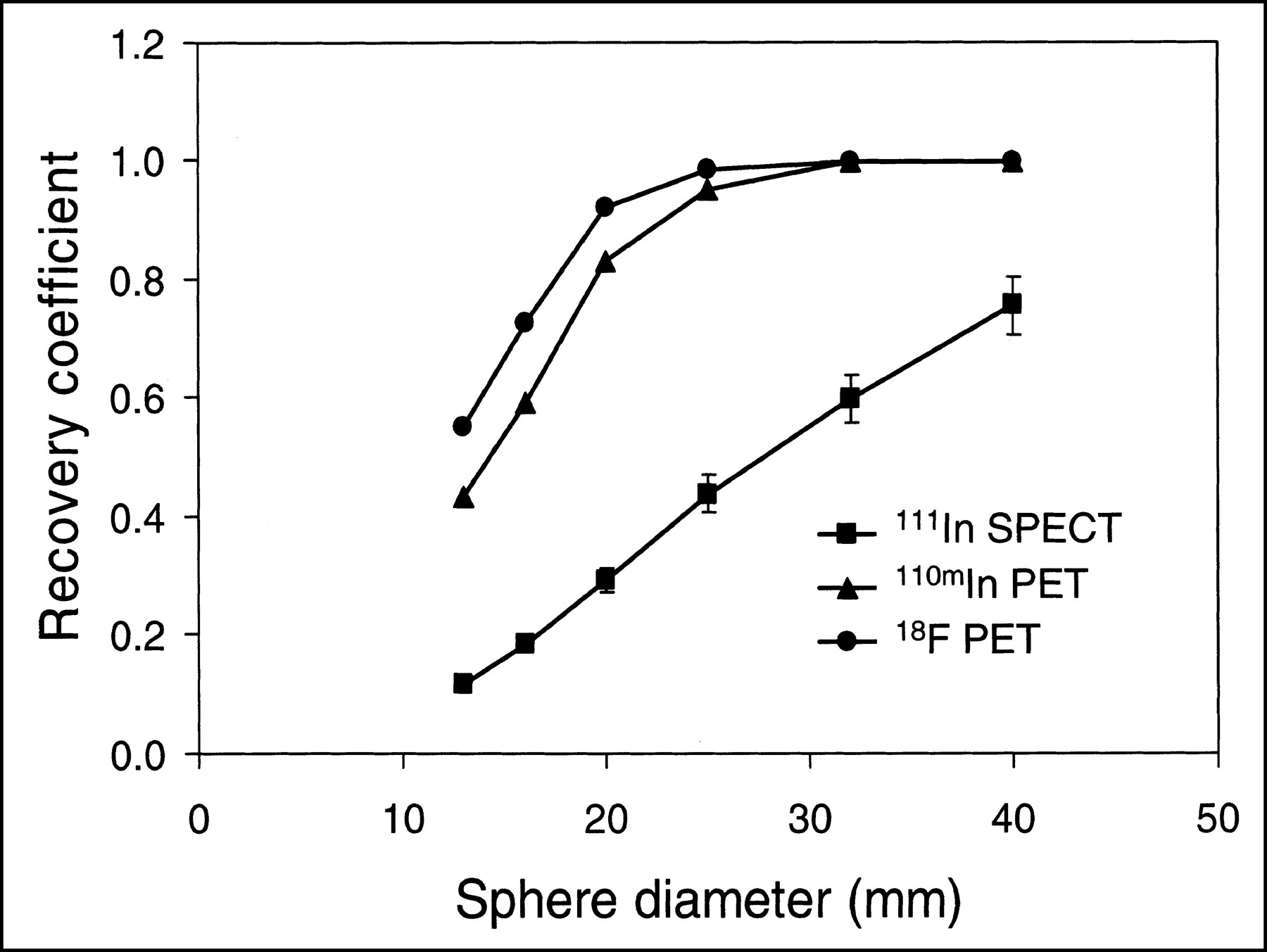
Sphere recovery functions for 110mIn PET, 111In SPECT, and 18F PET.
Clinical Imaging Study
SPECT images at 24 h after administration of 111In-octreotide are given in Figure 3. Figure 4 shows PET images taken approximately 1.5 h after administration of 110mIn-octreotide. The standard uptake values, calculated from the PET data, are given in Figure 5. The images clearly show that the tumor contour is seen better with PET than with SPECT using standard clinical settings.
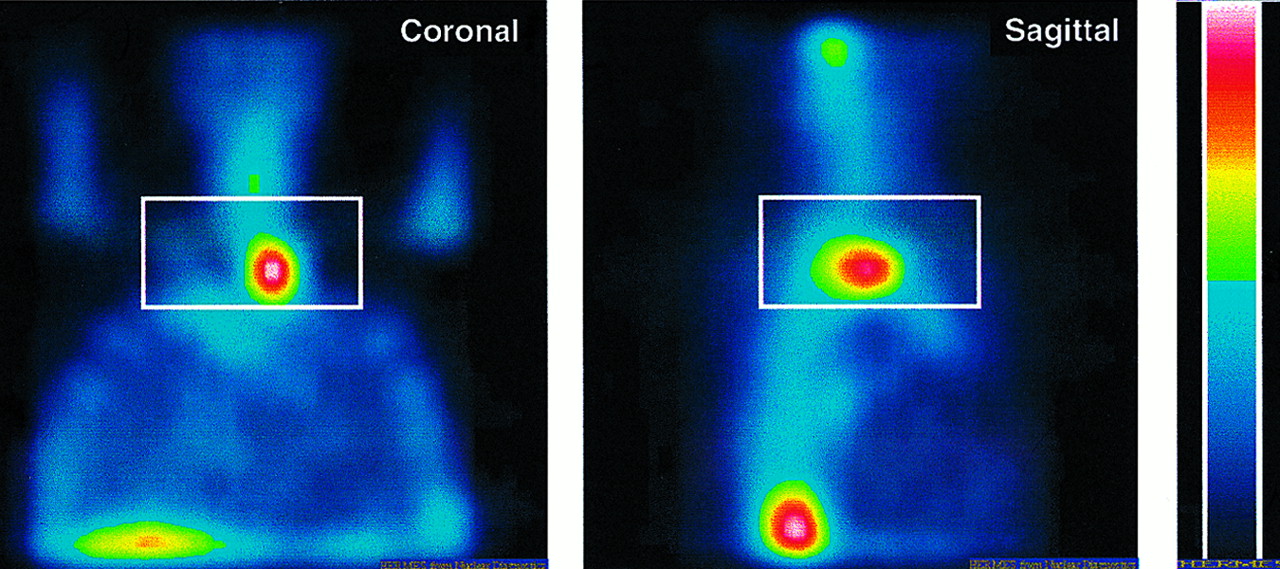
Reoriented reconstructed SPECT images 24 h after administration of 175 MBq of 111In-octreotide. Rectangles indicate position of PET images in Figure 4.
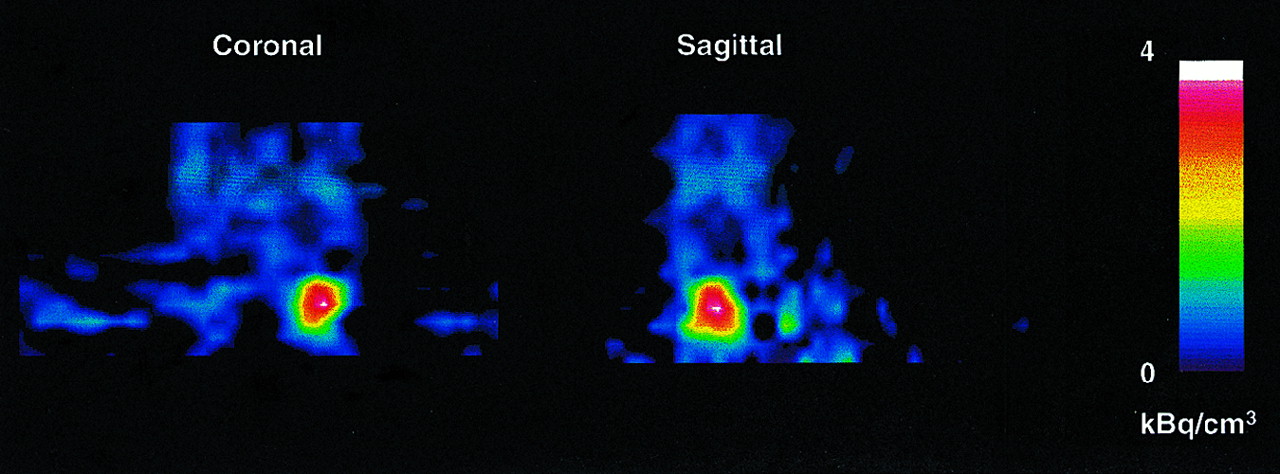
Reoriented PET images of same patient as in Figure 3, 1.5 h after administration of 110mIn-octreotide.
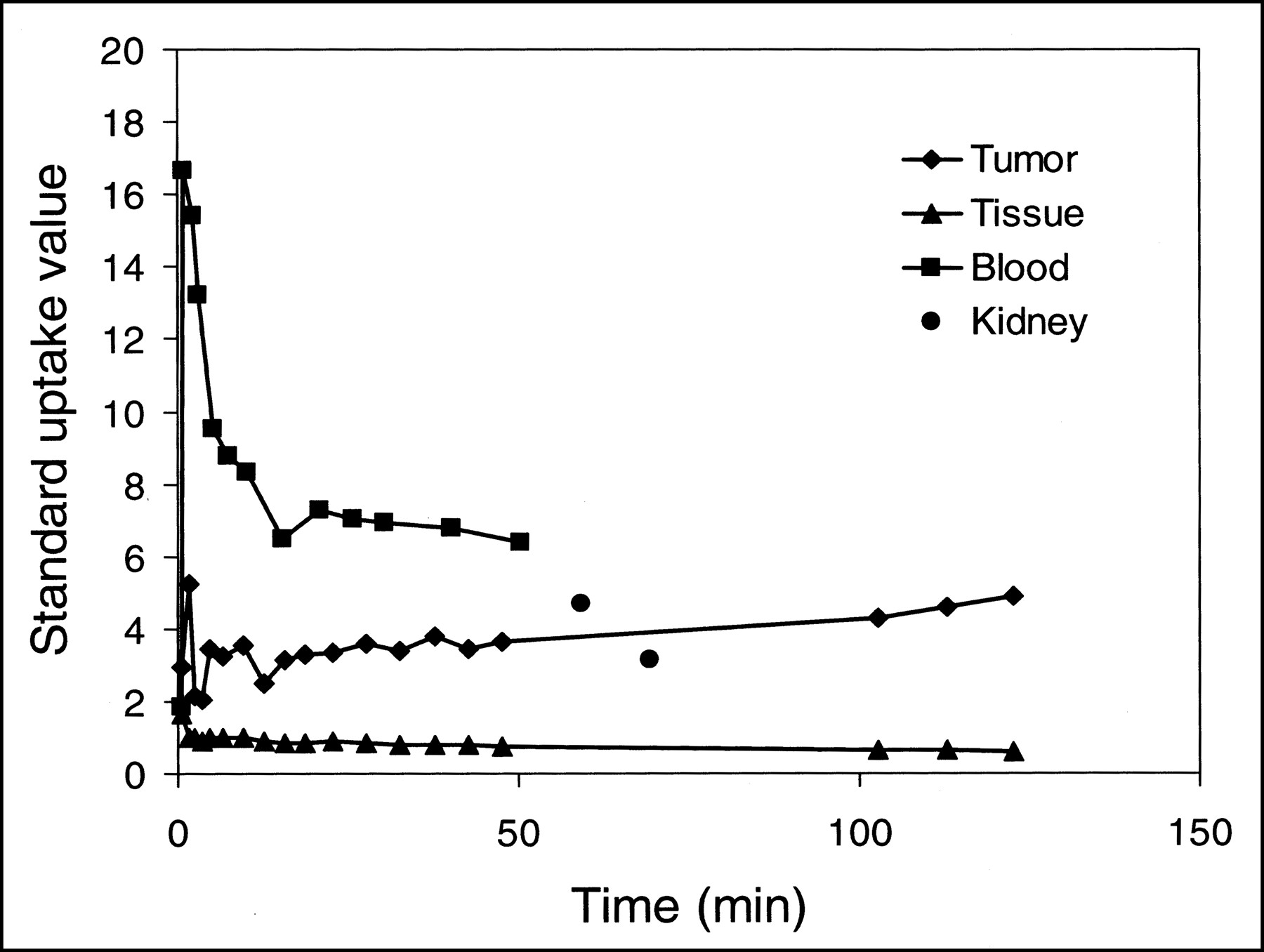
Standard uptake values of 110mIn-octreotide in tumor, background tissue, blood, and kidney. Error bars are of same size as markers.
DISCUSSION
Our initial labeling experiments confirmed that 110mIn-DTPA-d-Phe1-octreotide can easily be prepared using the OctreoScan kit and locally produced 110mIn. The availability of the commercial OctreoScan kit solves problems associated with good-manufacturing-practice production of the peptide–chelator conjugate, and OctreoScan is optimized for labeling with indium isotopes. The radionuclidic purity of the produced 110mIn met all requirements for human use, and the production rate gave a sufficient amount of radiopharmaceutical for several patients in 1 production run. The low energy required for the 110Cd(p,n)110mIn reaction makes it possible to use any commercially available cyclotron for local production of 110mIn. The half-life of 110mIn also opens the possibility of delivering the compound to satellite PET centers that do not have their own cyclotron for radionuclide production.
The performance studies clearly showed the improvement in resolution and recovery that can be obtained with 110mIn PET in comparison with 111In SPECT. An improvement in resolution by almost a factor 3 would meet the demands of imaging small tumors or metastases (<1 cm) as expressed in the literature (23,24). The sphere recovery measurements also showed that quantification is possible in structures with diameters of less than 2 cm. The poorer SPECT recovery, 76% in the largest sphere, was caused mainly by the difference in scatter contribution in the calibration and sphere recovery measurements. The calibration images contained approximately 26% scatter, even after scatter correction, whereas the scatter contribution in the sphere phantom images was much lower because of the distribution of scatter over whole images, not just the spheres, leading to an underestimation of activity concentration in the spheres. The amount of scatter in SPECT measurements causes a major problem in quantification, which can be improved by applying scatter corrections. However, the triple-energy-window scatter correction used here requires good count statistics in the narrow scatter windows and, thus, long measurement times. Kaplan et al. (25) suggested a method for 111In SPECT scatter correction based on energy spectrum fitting. Their method, although significantly increasing noise, decreased the measured scatter contribution in their images from 32% to 8%. Another factor introducing quantification problems in SPECT measurements is the applied uniform attenuation correction, which leads to overestimation of radioactivity concentrations in the lungs and underestimation in the bones. Compared with the 1% correction error for the pure positron emitter 18F, the correction error for 110mIn PET increased (26). This increase was caused by essentially true coincidences involving γ-radiation emitted in the decay of 110mIn. The PET scanner cannot distinguish between coincidences involving the 658-keV photon emitted in the 110mIn decay and coincidences involving 511-keV photons only. Correction methods for this effect have been suggested (27–29) but were not implemented at the time of this study.
The clinical imaging study shows that 110mIn-octreotide can be used in studies with PET. The 69-min half-life of 110mIn well matches the rapid kinetics of octreotide. The images and uptake curves clearly show the fast blood clearance and kidney uptake of 110mIn-octreotide. Kinetics were followed for only up to 2 h, but a measurement time of 4 h should be possible without increasing patient dose. The patient study showed a fast blood clearance phase, with a half-life of approximately 5 min, followed by a slower phase, fast initial uptake in the tumor, and a tumor-to-background uptake ratio of 8 after only 2 h. Even though the energy emitted per decay of 110mIn is 2.2 MeV, compared with 438 keV for 111In, the effective dose resulting from a PET study with several hundreds of megabecquerels of 110mIn-octreotide would be significantly smaller than the effective dose of an 111In-octreotide administration because of the much shorter half-life of 110mIn.
111In-labeled octreotide has also been proposed and evaluated for radionuclide therapy using the Auger and conversion electrons emitted in its decay (30–33). Dose planning, advanced calculation of dose distribution, and dose monitoring during therapy are prerequisites for successful external therapy. We believe that this same approach is needed if targeted radionuclide therapy is to become successful. Because dose planning is necessary in each patient, there is a need to estimate the spatial and temporal distribution of the therapeutic radionuclide before therapy. During therapy, actual uptake of the radionuclide in tumor and critical organs needs to be determined in order to obtain the radioactivity integral and thus the absorbed dose as accurately as possible. Introduction of the positron-emitting analog 110mIn might help to obtain more precise values of the radioactivity concentration in tumors and the critical organs of a given patient and thus aid in the optimization of the therapeutic regimen. This concept has also been suggested for the isotopic analogues 90Y/86Y (34) and 131I/124I (35,36), and several approaches for dosimetric calculations have been published (37–39). Similar half-lives of the positron-emitting and therapeutic isotopes facilitate calculation of the radioactivity integral, which is needed to obtain a good estimate of the absorbed dose. Such a similarity in half-life exists for the isotopic pairs 90Y/86Y and 131I/124I but not for 111In/110mIn (Table 1). However, the half-life of 110mIn is long enough to measure the first hours of the octreotide kinetics in the individual patient, after which a stationary situation may have become established. The later distribution, measured by gamma camera techniques, can then be related to the early, detailed quantitative PET measurements. Although PET gives a spatial resolution of less than 1 cm3, only macroscopic dose information is obtained, which is sufficient in healthy tissue. An important part of the dose delivered by 111In is due to the Auger electrons or the conversion electrons emitted in its decay. Biopsies and other studies have to be added if a more detailed dosimetry on the cellular level is wanted. However, being able to determine an accurate macroscopic dose is an important and necessary first step to beginning to understand the dose–effect relationship of this type of therapy.
Treatment with nonlabeled octreotide is helpful in controlling clinical symptoms through hormone hypersecretion inhibition in most patients with metastatic carcinoids, gastrinomas, insulinomas, and glucagonomas (40). However, evidence has been found that this kind of treatment may cause downregulation of the somatostatin receptors in tumor cells (24). Quantitative assessment of somatostatin receptor density may be useful in such tumors to evaluate the rationale for somatostatin therapy and to monitor the effect of treatment. The short half-life of 110mIn, which allows repeated investigations, is here useful to determine the optimal receptor concentration for successful therapy.
CONCLUSION
Limited resolution and recovery of single-photon imaging techniques can result in undetected tumors or metastases when neuroendocrine tumors are imaged with 111In-octreotide. Therefore, we attempted to enhance the possibilities of octreotide by substituting for 111In its positron-emitting analog 110mIn and the use of PET. 110mIn-DTPA-d-Phe1-octreotide can be prepared using the OctreoScan kit and locally produced 110mIn. Phantom studies and a clinical imaging study show that PET with 110mIn-DTPA-d-Phe1-octreotide can better detect small tumors and might be able to more accurately quantify tumor uptake than can 111In-DTPA-d-Phe1-octreotide and SPECT.
Acknowledgments
We thank Dr. Sten Nilsson for his input, Dr. Ulrike Garske for helpful comments on the manuscript, Mimi Lidholm for preparation of the radiopharmaceuticals, and the staff at Uppsala University PET Centre and the Division of Oncological Nuclear Medicine at Uppsala University Hospital for assistance with the measurements. We also thank the staff of The Svedberg Laboratory for technical help. This study was supported by grants 3978-B97-01XBB and 3978-B98-02XBB from the Swedish Cancer Society.
Footnotes
Received Dec. 31, 2001; revision accepted Jun. 11, 2002.
For correspondence or reprints contact: Mark Lubberink, PhD, Uppsala Research Imaging Solutions AB, Uppsala University Hospital, 751 85 Uppsala, Sweden.
E-mail: mark.lubberink{at}pet.uu.se
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.