


Abstract
242271
Introduction: Prostate cancer is the second most commonly diagnosed cancer in men and a leading cause of cancer death worldwide. After primary definitive therapy of localized prostate cancer with either radical prostatectomy or radiation therapy, up to 50% of patients will experience biochemical recurrence (BCR) of disease. Current clinical guidelines do not give clear indications on the management of BCR. Both PSMA PET/CT and pelvic MRI can provide useful information about the location of disease, which can guide more tailored management of these patients. The objective of this descriptive, retrospective analysis is to compare the performance of PSMA PET/CT and pelvic MRI in BCR and investigate the added value of their combined use in this patient population.
Methods: 45 patients with localized BCR who underwent PSMA PET/CT and pelvic MRI within three months of each other at the University of California, Los Angeles were included in our retrospective analysis. Patients who underwent any other treatments between the two scans, patients lost to follow-up, or patients with disease on PSMA PET/CT outside the field-of-view of the pelvic MRI were excluded. Two board-certified nuclear medicine physicians blinded to clinical information interpreted the PSMA PET/CT scans independently and described up to three positive findings. A third nuclear medicine physician resolved any disagreements (2:1 majority rule). In a similar framework, two radiologists interpreted the pelvic MRIs with a third radiologist serving as a tiebreaker. Data on disagreements between clinical PSMA PET/CT and pelvic MRI reads, disagreements between blinded and clinical PSMA PET/CT and pelvic MRI reads, and differences in management based on findings from clinical PSMA PET/CT and pelvic MRI were collected.
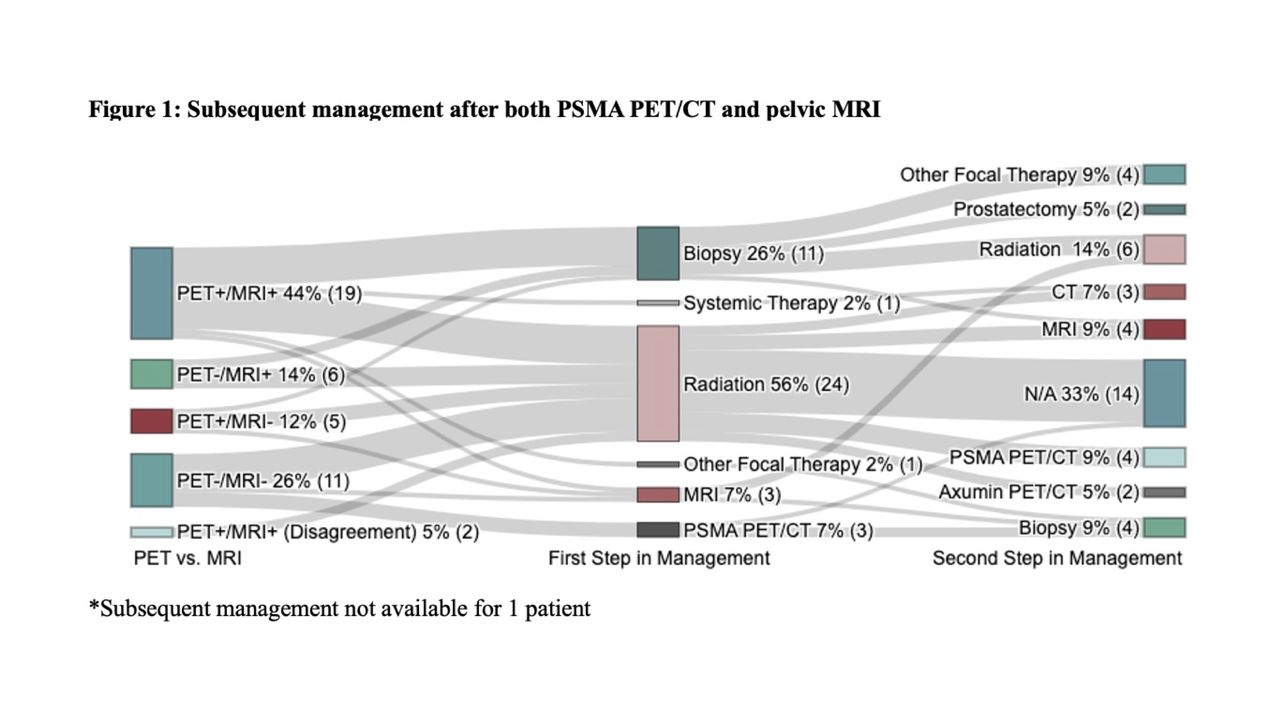
Results: Out of 45 patients in our cohort, 27 were initially treated with prostatectomy, 15 were treated with radiation, and 3 were treated with other focal therapies. 5/45 patients had a negative pelvic MRI and positive PSMA PET/CT, with 44% of these lesions noted to be in the lymph nodes, while 7/45 patients had a negative PSMA PET/CT and positive pelvic MRI, with 100% of these lesions noted to be in the prostate or prostate bed. Table 1 summarizes findings from clinical PSMA PET/CT and pelvic MRI reads, while Table 2 summarizes disagreements between clinical PSMA PET/CT and pelvic MRI reads. In 5/45 patients, the blinded PSMA PET/CT reads were negative while the clinical PSMA PET/CT reads were positive, and in 5/45 patients, the blinded pelvic MRI reads were negative while the clinical pelvic MRI reads were positive. Table 3 and Table 4 summarize disagreements between blinded and clinical PSMA PET/CT and pelvic MRI reads respectively. 56% of patients underwent radiation as a next step in management, 26% underwent biopsy, 14% underwent follow-up imaging, and 4% underwent other focal or systemic therapy. Figure 1 shows a Sankey diagram, which characterizes subsequent management strategies based on findings on clinical PSMA PET/CT and MRI.
Conclusions: In this retrospective, descriptive analysis of 45 patients with localized BCR, there was good agreement between PSMA PET/CT and pelvic MRI, although pelvic MRI may overcall lesions in the prostate and prostate bed and miss nodal metastases. Most patients with localized BCR underwent radiation therapy or biopsy following PSMA PET/CT and MRI, with a minority of patients undergoing follow-up imaging, systemic therapy, or focal therapy.


In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.