


Abstract
Previously, based on the concept of bifunctional radiopharmaceuticals, we developed a highly stable 186Re-mercaptoacetylglycylglycylglycine (MAG3) complex–conjugated bisphosphonate, [[[[(4-hydroxy-4,4-diphosphonobutyl)carbamoylmethyl]carbamoylmethyl]carbamoylmethyl]carbamoylmethanethiolate] oxorhenium(V) (186Re-MAG3-HBP), for the treatment of painful bone metastases. This agent showed a superior biodistribution as a bone-seeking agent in normal mice when compared with 186Re-1-hydroxyethylidene-1,1-diphosphonate (186Re-HEDP). In this study, we evaluated the therapeutic effects of 186Re-MAG3-HBP using an animal model of bone metastasis. Methods: The model was prepared by injecting syngeneic MRMT-1 mammary tumor cells into the left tibia of female Sprague–Dawley rats. 186Re-MAG3-HBP (55.5, 111, or 222 MBq/kg) or 186Re-HEDP (55.5 MBq/kg) was then administered intravenously 21 d later. To evaluate the therapeutic effects and side effects, tumor size and peripheral blood cell counts were determined. Palliation of bone pain was evaluated by a von Frey filament test. Results: In the rats treated with 186Re-HEDP, tumor growth was comparable with that in untreated rats. In contrast, when 186Re-MAG3-HBP was administered, tumor growth was significantly inhibited. Allodynia induced by bone metastasis was attenuated by treatment with 186Re-MAG3-HBP or 186Re-HEDP, but 186Re-MAG3-HBP tended to be more effective. Conclusion: These results indicate that 186Re-MAG3-HBP could be useful as a therapeutic agent for the palliation of metastatic bone pain.
Malignant tumors, especially cancers of the breast and prostate, frequently metastasize to bone (1,2). A prominent symptom of such metastasis is pain, which has a significant impact on patient quality of life, and pain within the skeletal tissues is the most common source of pain in patients with malignant disease (3–5). Treatments designed to reduce inflammation-associated pain with nonsteroidal antiinflammatory drugs (NSAIDs) are the first option in most cases, with stronger opioids used as the intensity of the pain rises. However, these drugs produce side effects such as gastrointestinal ulceration, neutropenia, enhanced bleeding, and deterioration of renal function in the case of NSAIDs, and nausea, sedation, and constipation in the case of opioids. Localized radiation therapy is an effective treatment for bone pain (6) but is difficult to apply when there are multiple lesion sites, as is often the case in patients with bone metastases. Wide-field, hemibody radiotherapy is also an effective treatment but its potential benefit is often outweighed by significant bone marrow and gastrointestinal toxicity. Accordingly, in cases of metastases to multiple sites, molecular radiotherapy using bone-seeking radiopharmaceuticals is preferable (7,8).
186Re is a promising radionuclide with a maximum β-energy of 1.07 MeV and a γ-ray of 137 keV (9%) that are adequate for therapy and imaging, respectively. Furthermore, the physical half-life of 186Re is 3.8 d, which is long enough for shipment and processing of the radiopharmaceutical but not too long for its disposal as a radioactive waste. These physical characteristics have led to the development and clinical application of 186Re-1-hydroxyethylidene-1,1-diphosphonate (186Re-HEDP) (9,10). However, 186Re-HEDP showed a delayed blood clearance and high gastric uptake after injection, due to its instability in vivo (11–14). Thus, to overcome the problems of 186Re-HEDP, we recently developed, based on the concept of bifunctional radiopharmaceuticals, a highly stable 186Re-mercaptoacetylglycylglycylglycine (MAG3) complex–conjugated bisphosphonate, [[[[(4-hydroxy-4,4-diphosphonobutyl)carbamoylmethyl]carbamoylmethyl]carbamoylmethyl]carbamoylmethanethiolate] oxorhenium(V) (186Re-MAG3-HBP, Fig. 1) (15). This agent showed greater accumulation in bone and faster clearance from blood than 186Re-HEDP in normal mice.

Chemical structure of Re-MAG3-HBP.
In this study, we evaluated the therapeutic potential of 186Re-MAG3-HBP in comparison with 186Re-HEDP for the palliation of metastatic bone pain using an animal model of bone metastasis.
MATERIALS AND METHODS
Materials
186Re was supplied by the Japan Atomic Energy Research Institute as perrhenate ( ) at a specific activity of 18–20 TBq/g. Other reagents were of reagent grade and were used as received.
) at a specific activity of 18–20 TBq/g. Other reagents were of reagent grade and were used as received.
186Re-HEDP, 186Re-MAG3-HBP, and nonradioactive Re-MAG3-HBP were prepared according to a published procedure (15) with radiochemical yields of >90% without requiring purification. The radiochemical purity of 186Re-HEDP was determined by thin-layer chromatography (TLC) and cellulose acetate electrophoresis (CAE) (Separax-SP; Joko Co. Ltd.). TLC analyses were performed with silica plates (Silica gel 60; Merck KGaA) with acetone as a developing solvent. 186Re-HEDP remained at the original position (Rf = 0), whereas the free perrhenate ( ) migrated with the solvent front (Rf = 1). CAE was run at an electrostatic field of 0.8 mA/cm for 20 min in veronal buffer (ionic strength 0.06 M, pH 8.6). 186Re-HEDP migrated to the 3.5-cm anode from the origin, whereas reduced-hydrolyzed rhenium (186ReO2) remained at the origin. The radiochemical purity of 186Re-MAG3-HBP was determined by reversed-phase (RP) high-performance liquid chromatography (HPLC). RP-HPLC was performed with a Cosmosil 5C18-AR-300 column (4.6 × 150 mm; Nacalai Tesque) at a flow rate of 1 mL/min with a mixture of 0.2 mol/L phosphate buffer (pH 6.0) and ethanol (90:10) containing 10 mmol/L tetrabutylammonium hydroxide.
) migrated with the solvent front (Rf = 1). CAE was run at an electrostatic field of 0.8 mA/cm for 20 min in veronal buffer (ionic strength 0.06 M, pH 8.6). 186Re-HEDP migrated to the 3.5-cm anode from the origin, whereas reduced-hydrolyzed rhenium (186ReO2) remained at the origin. The radiochemical purity of 186Re-MAG3-HBP was determined by reversed-phase (RP) high-performance liquid chromatography (HPLC). RP-HPLC was performed with a Cosmosil 5C18-AR-300 column (4.6 × 150 mm; Nacalai Tesque) at a flow rate of 1 mL/min with a mixture of 0.2 mol/L phosphate buffer (pH 6.0) and ethanol (90:10) containing 10 mmol/L tetrabutylammonium hydroxide.
Biodistribution in Normal Rats
Experiments with animals were conducted in accordance with our institutional guidelines, and the experimental procedures were approved by the Kyoto University Animal Care Committee. Biodistribution experiments were performed by intravenously administering 186Re-labeled compounds into male Wistar rats (200–250 g). Groups of 4 rats each were administered 250 μL of each 186Re-labeled compound and sacrificed at 10 min, 3 h, and 24 h after injection. Tissues of interest were removed and weighed, and radioactivity counts were determined with an auto well γ-counter (ARC-2000; Aloka) and corrected for background radiation and physical decay during counting.
Rat Model of Bone Metastasis
Female Sprague–Dawley rats were used (150–180 g). The animals were housed with free access to food and water at 25°C with a 12-h alternating light/dark cycle. MRMT-1 mammary tumor cells were kindly supplied by the Cell Resource Center for Biomedical Research, Tohoku University. The culture of MRMT-1 cells and induction of bone cancer was performed as previously described with slight modifications (16). Briefly, MRMT-1 cells were grown in cell culture dishes in RPMI 1640 medium with phenol red, 10% heat-inactivated fetal calf serum, 100 μg/mL glutamine, 100 units/mL penicillin, and 100 μg/mL streptomycin. The cells were cultured in a humidified atmosphere of 95% air and 5% carbon dioxide at 37°C. They were then released from the dishes by treatment with 0.05% trypsin/ethylenediaminetetraacetic acid. Next, the rats to be inoculated were anesthetized with chloral hydrate, and a 1.5-cm incision was made over the top half of the tibia. A 23-gauge needle was inserted into the intramedullary canal of the tibia, approximately 5 mm below the knee joint to create a cavity for injection of the cells. At the left tibia, 3 μL of medium with tumor cells (approximately 3 × 103 cells) was then injected into the bone cavity using a Hamilton syringe (Hamilton Co.). At the right tibia, 3 μL of medium only was injected into the bone cavity as a sham-treated control. The cavities were sealed using bone wax, and the wounds were closed with surgical suture.
Imaging and Therapy
Rats were randomly distributed to the experimental groups. 186Re-MAG3-HBP (55.5, 111, or 222 MBq/kg), 186Re-HEDP (55.5 MBq/kg), or nonradioactive Re-MAG3-HBP was administered intravenously 21 d after inoculation—that is, the time needed for tumors to reach a palpable size (about 1 cm in diameter). A group of rats that did not receive any treatment served as a control group.
At 24 h after the injection of radiolabeled compounds, γ-imaging was performed on a SPECT-2000H (Hitachi Medical Co.) fitted with low-energy, high-resolution collimators. The energy window was symmetric (±20%) and centered on the 186Re photopeak (137 keV).
Tumoral bone-to-normal bone ratios were calculated by drawing regions of interest (ROIs) on planar images (counts/pixel). The ROI of tumoral bone was drawn manually around the edge of the tumoral bone activity by visual inspection. The ROI of normal bone was drawn at the corresponding site of the contralateral tibia (sham-treated) using an inverted figure of the tumoral bone ROI.
Tumor size was measured once weekly with a slide caliper in 2 dimensions. Individual tumor volumes (V) were calculated by the formula V = [length × (width)2]/2 and related to the values on the day of treatment (relative tumor volume).
Pain was evaluated as the hind paw withdrawal response to stimulation with von Frey filaments (North Coast Medical) as previously described with slight modifications (17,18). The test environment consisted of a wire mesh box. The rat was placed in the test box and allowed to acclimate for 5–10 min. The tactile stimulus was applied to the plantar surface in ascending order of force beginning with the 2.84-mN filament. Once a withdrawal response was established, the paw was retested, starting with the next descending von Frey filament until no response occurred. The lowest amount of force required to elicit a response was recorded as the paw withdrawal threshold (in newtons [N]). The ratio of the right value to the left value was used as an index of the palliation of pain.
The myelotoxicity of the radiotherapy was assessed using the peripheral blood cell counts. Two blood samples (5 μL) were obtained from a tail vein. The samples were pooled and diluted with 95 μL of Turk's solution (0.01% gentian violet and 1% acetic acid) for white blood cell (WBC) counts and 495 μL of 1% ammonium oxalate for platelet counts, and cell counts were performed using a hemocytometer and a light microscope.
Statistical Evaluation
An unpaired Student t test was used for the biodistribution experiments. One-way ANOVA followed by the Dunnett post hoc test compared with the untreated group was used for experiments on allodynia measurements, comparisons of tumor growth, WBC counts, and platelet counts. Results were considered statistically significant at P < 0.05.
RESULTS
Biodistribution in Normal Rats
The biodistributions of 186Re-MAG3-HBP and 186Re-HEDP in normal rats are presented in Table 1. Both compounds showed a rapid accumulation and long residence in the bone. The uptake of 186Re-MAG3-HBP in the bone was significantly higher than that of 186Re-HEDP.
Biodistribution of 186Re-MAG3-HBP and 186Re-HEDP in Rats
Imaging
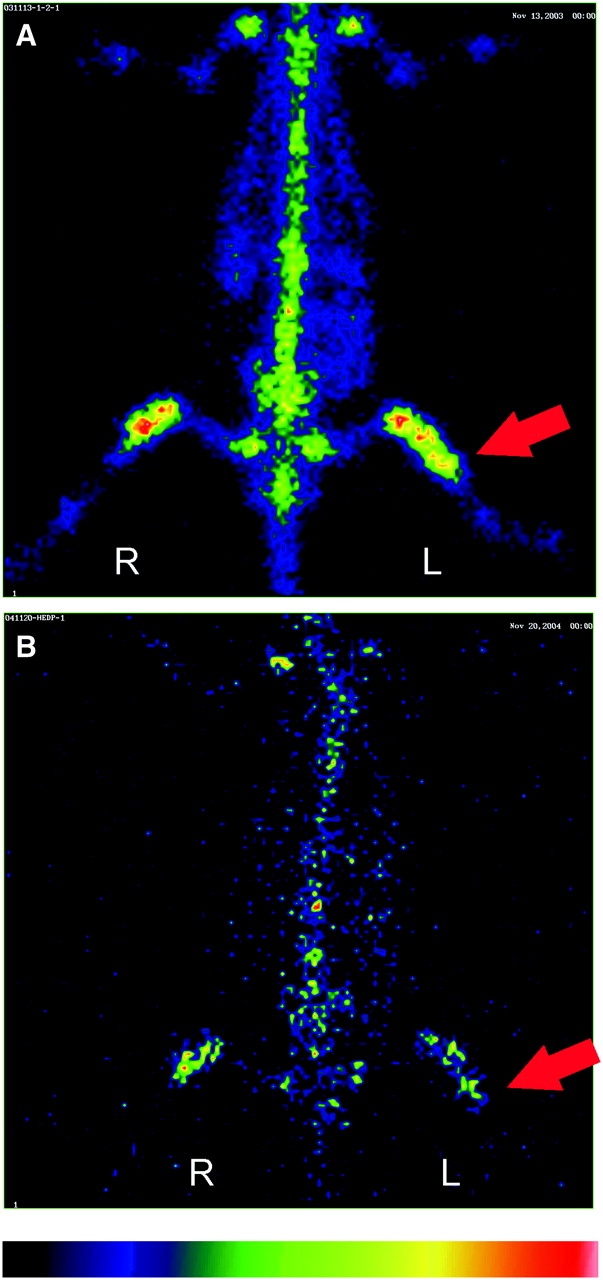
The planar images at 24 h after injection of 186Re-MAG3-HBP and 186Re-HEDP showed a marked accumulation of radioactivity surrounding the site of inoculation of the tumor cells (Fig. 2). In tissues other than bone, no significant accumulation of radioactivity was observed, a reflection of the results of the biodistribution experiments.
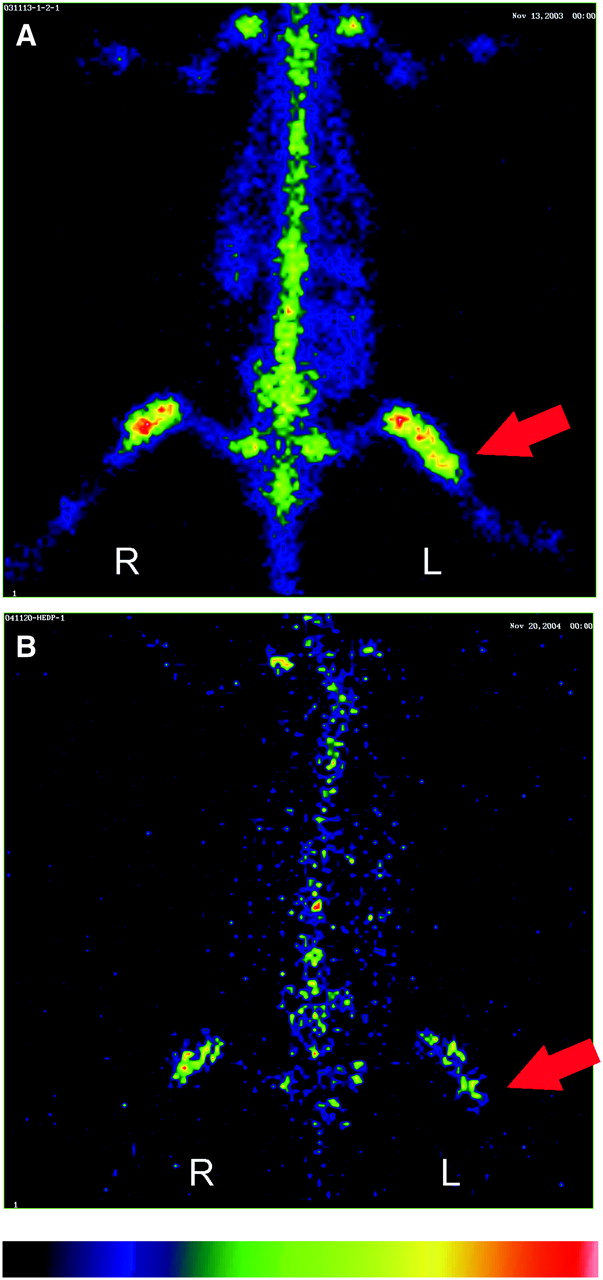
Planar images at 24 h after intravenous injection of 186Re-MAG3-HBP (222 MBq/kg) (A) and 186Re-HEDP (55.5 MBq/kg) (B). Arrows indicate the site where tumor cells were injected.
Tumoral bone-to-normal bone ratios of 186Re-MAG3-HBP and 186Re-HEDP were 3.54 ± 0.60 and 2.90 ± 0.97, respectively (mean ± SD). This difference was not statistically significant.
Therapeutic Effects
The volume of the tumors as a function of time is shown in Figure 3. As can be seen, the MRMT-1 tumor cells proliferated exponentially after a palpable tumor developed in the left tibia. In rats treated with 186Re-HEDP at a dose of 55.5 MBq/kg, tumor growth was comparable with that of untreated rats. In contrast, when 186Re-MAG3-HBP was administered at the same dose as 186Re-HEDP, tumor growth was significantly inhibited compared with that of the untreated group.
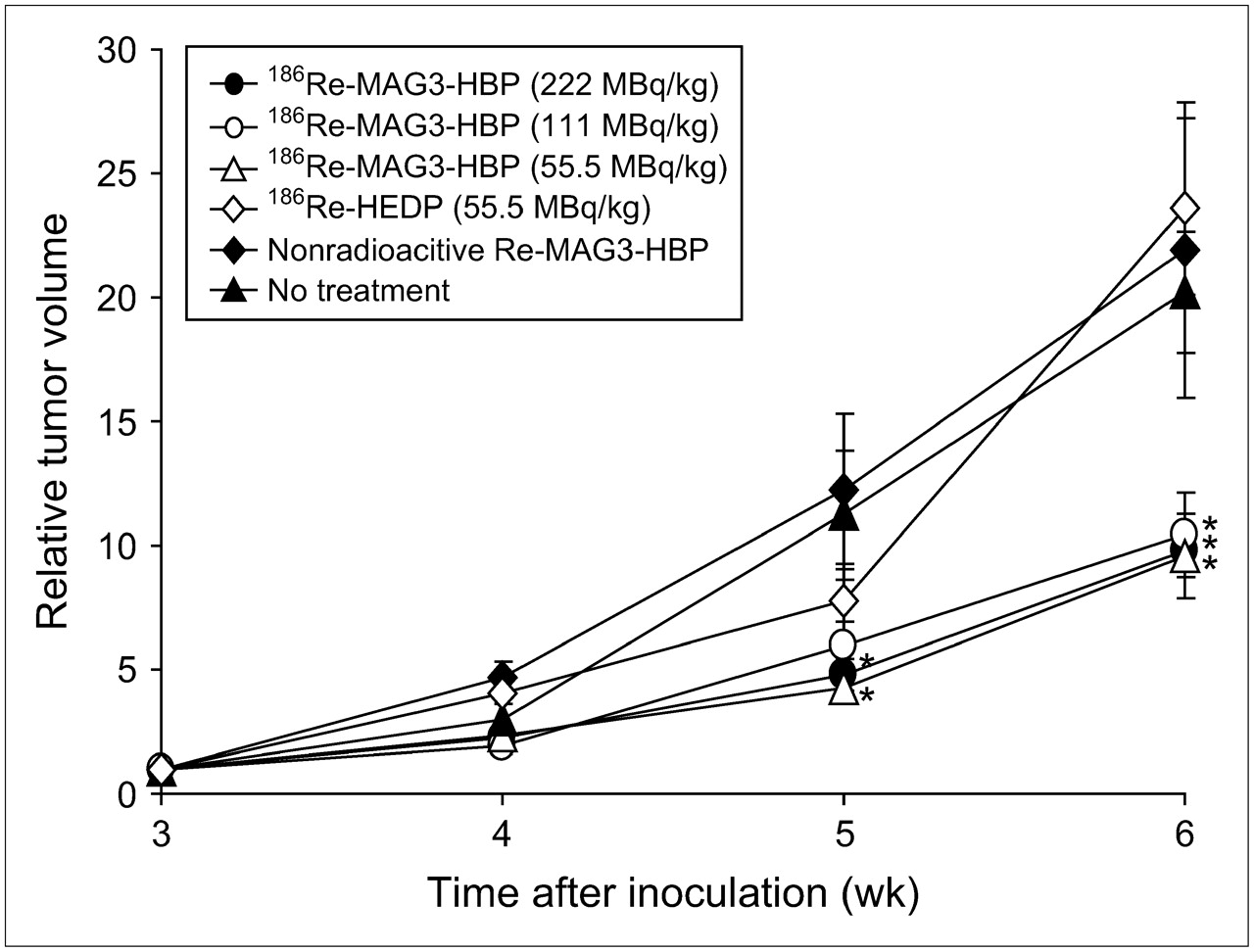
Curves show inhibition of growth of MRMT-1 tumor cells on therapy. Data are expressed as tumor volume relative to that on day of treatment (mean ± SEM for 5–7 rats). Significance was determined using 1-way ANOVA followed by the Dunnett post hoc test (*P < 0.05 vs. no treatment).
Palliative effects determined by the von Frey filament test are shown in Figure 4. A larger value indicates more intense pain on the cancer-bearing side. In untreated rats, the enhanced withdrawal response to mechanical stimulation with von Frey filaments caused by cancer-induced bone pain was elevated. Both 186Re-MAG3-HBP and 186Re-HEDP attenuated this mechanical allodynia but 186Re-MAG3-HBP tended to be more effective.
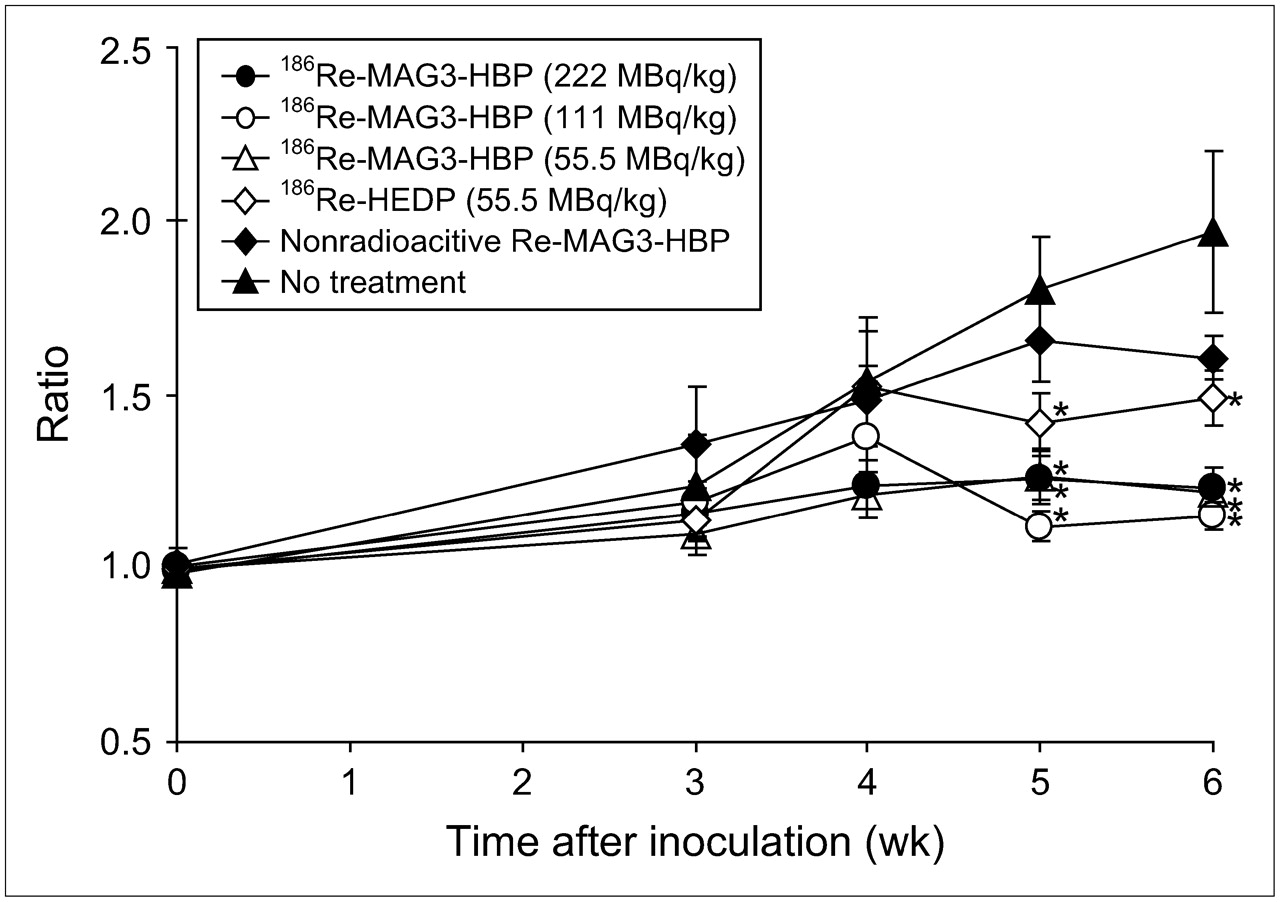
Effects of radiopharmaceuticals on bone cancer pain. Data are expressed as ratio of right (contralateral) withdrawal paw threshold values to left (ipsilateral) values (mean ± SEM for 5–7 rats). Significance was determined using 1-way ANOVA followed by the Dunnett post hoc test (*P < 0.05 vs. no treatment).
The injected dose of 186Re-MAG3-HBP ranged from 55.5 to 222 MBq/kg, and the therapeutic effects were assessed. Consequently, it was found that the inhibition of tumor growth and the response in terms of the palliation of pain were not correlated with the treatment dose (Figs. 3 and 4).
Moreover, when nonradioactive Re-MAG3-HBP was administered, tumor growth and the withdrawal response were not significant compared with those in untreated rats (Figs. 3 and 4).
Myelotoxicity
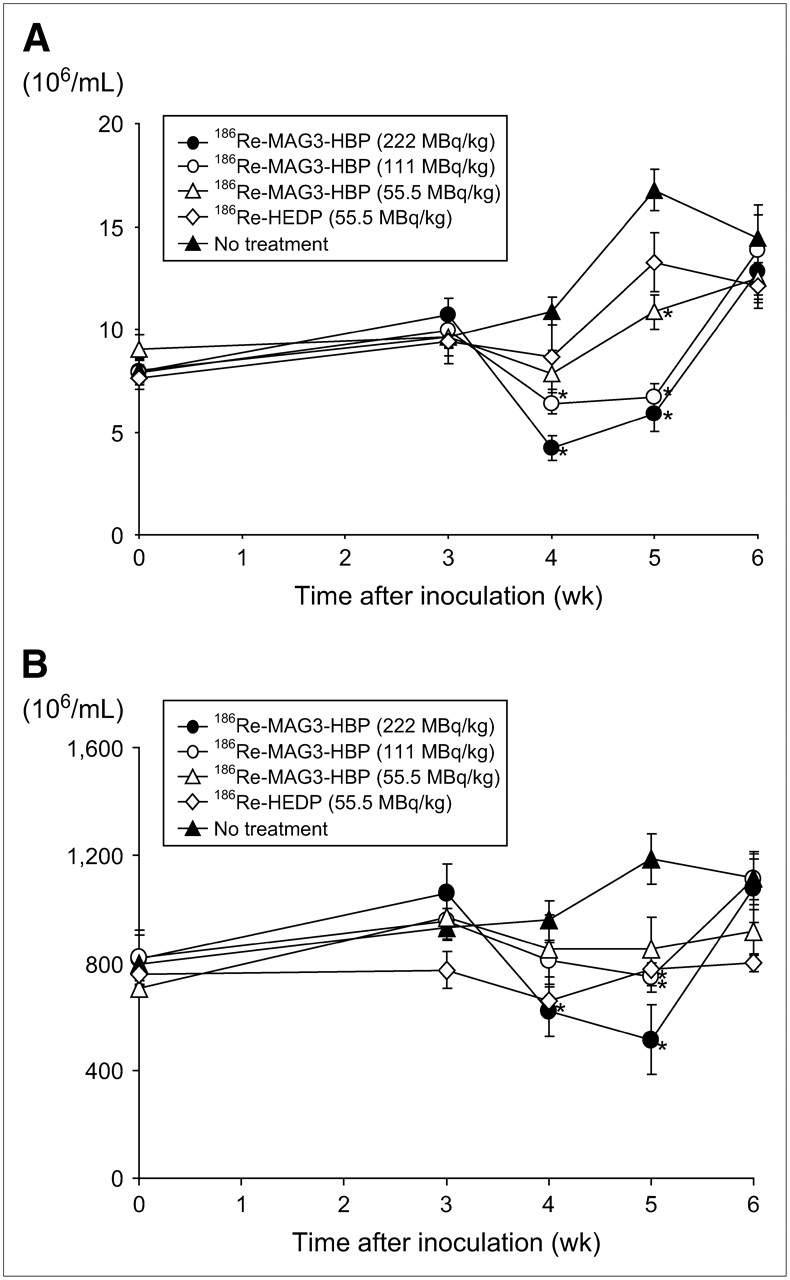
When 186Re-MAG3-HBP or 186Re-HEDP was administered, WBC and platelet counts tended to decrease at 1 and 2 wk after treatment, especially in the case of high-dose treatment with 186Re-MAG3-HBP. However, the decreases were not critical, and these counts were recovered within 3 wk after the injection (Fig. 5).
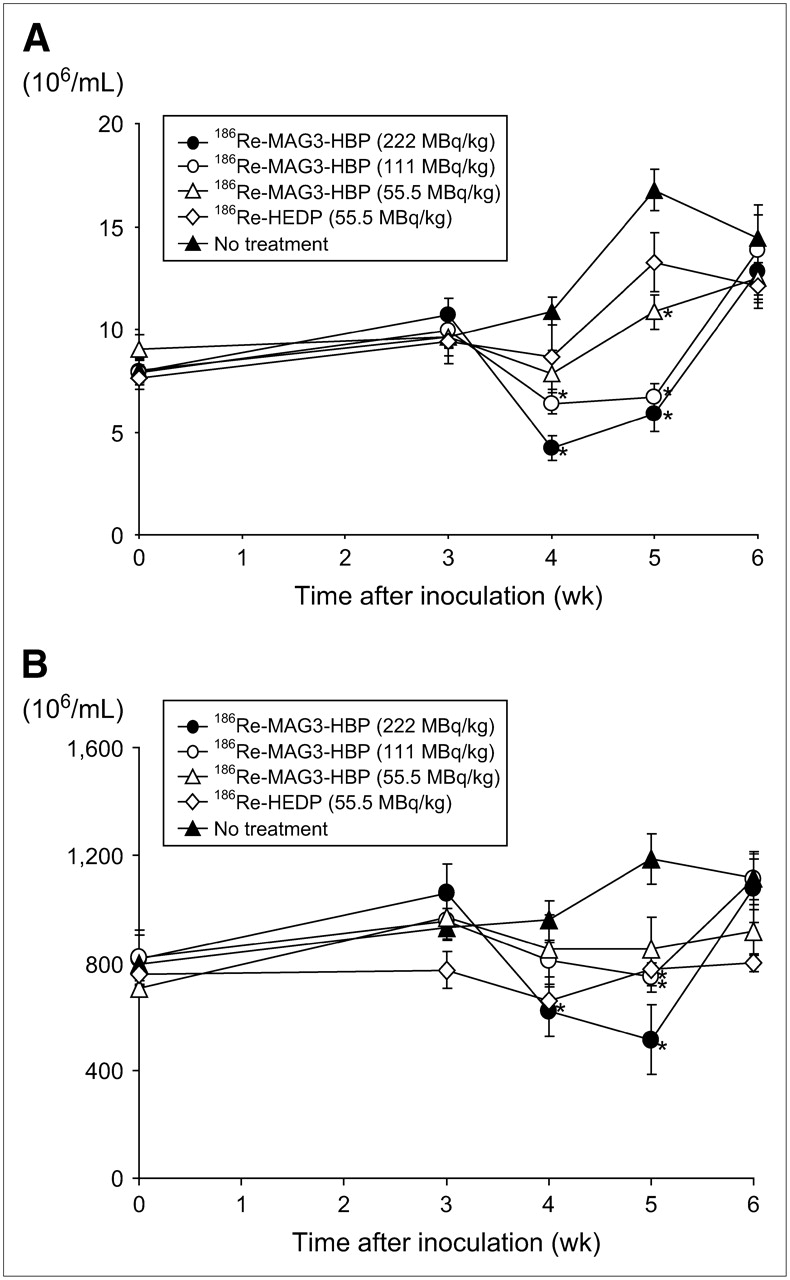
WBC (A) and thrombocyte (B) counts in rat model of bone metastasis under treatment. Data are presented as mean ± SEM for 5–7 rats. Significance was determined using 1-way ANOVA followed by the Dunnett post hoc test (*P < 0.05 vs. no treatment).
DISCUSSION
In general, the use of an appropriate animal model is important for the evaluation of the therapeutic effects of pharmaceuticals. For the evaluation of therapeutic effects of radiopharmaceuticals on metastatic bone tumors, a heart injection model has often been used (19,20). This model involves the direct introduction of tumor cells into the arterial circulation through the left ventricle of the heart in nude mice or nude rats (21,22). It is useful for the evaluation of survival (19,20) but is unsuitable for the evaluation of palliation of metastatic bone pain because it has multiple lesion sites. Furthermore, to our knowledge, there has been no report on an appropriate animal model for the evaluation of the palliating effects of radiopharmaceuticals on metastatic bone pain. However, intrabone injection models have recently been developed as a model of bone tumor pain (16,23,24). In this study, we used one of these models, the intratibial injection model, for the following reasons: (a) the radiologic, histologic, and behavioral characteristics resemble those of patients with bone metastases (5,16,25); (b) it is possible to equalize the position of single lesions in all experimental animals; (c) bone cancer pain can be quantitatively evaluated using a von Frey filament test; and (d) the surgery is simple and barely invasive.
The von Frey filament test is a way to examine withdrawal responses for mechanical stimuli to the hind paw of rats using various different von Frey filaments and has frequently been used for evaluating mechanical allodynia, especially in a neuropathic pain model (17,18). Recently, the test has also been used in a metastasis model (16,25). Bone cancer pain can be intermittent, but it progresses rapidly into continuous pain that is exacerbated by episodes of breakthrough pain. Once this chronic pain is established, the condition of the patient deteriorates further when mechanical allodynia develops. Mechanical allodynia occurs when normally nonpainful activity or stimulation is perceived as painful. For example, coughing, turning in bed, or gentle limb movement can cause intense pain (26). Accordingly, evaluating mechanical allodynia as an index of pain in the model is meaningful.
Moreover, it has been reported that levels of osteoblastic/osteoclastic activity were high in areas close to the tumor because the MRMT-1 cells used in this model produce a mixed type of bone lesion (16). Most bone-seeking radiopharmaceuticals, including 186Re-MAG3-HBP, accumulate at sites with strong osteoblastic activity. Accordingly, we assumed that this model might be adequate to evaluate the therapeutic effects of bone-seeking radiopharmaceuticals.
The main finding of this study is that a single treatment with 186Re-MAG3-HBP, a 186Re-complex–conjugated bisphosphonate, achieved significant inhibition of tumor growth and palliation of pain in a rat model of bone metastasis (Figs. 3 and 4). 186Re-HEDP palliated the pain but did not inhibit tumor growth. Although the mechanism of the palliation of bone cancer pain by radiotherapy remains unclear, a radiation-induced reduction of tumor size has been considered one of the causes (27,28). However, empiric data from experiments with external irradiation indicate that the absorbed dose required to achieve pain relief is significantly lower than that necessary to achieve a tumoricidal effect (29–31). Because 186Re-MAG3-HBP showed much greater accumulation in normal bone than did 186Re-HEDP in biodistribution experiments with normal rats and because there was no significant difference between the tumoral bone-to-normal bone ratios of 186Re-MAG3-HBP and 186Re-HEDP in the bone metastasis model, the difference in the inhibition of tumor growth between the 2 radiopharmaceuticals could be attributed to the difference in accumulation at the site of bone metastasis. Furthermore, the inhibition of tumor growth should result in a more effective palliation than that achieved with 186Re-HEDP.
The pain-relieving effect of 186Re-MAG3-HBP was not dependent on dose (Fig. 4). This result is consistent with the clinical observations in breast cancer patients that the response rate in terms of pain reduction was not correlated with the dose of 186Re-HEDP (10). Contrary to expectation, raising the dose of 186Re-MAG3-HBP did not potentiate the inhibition of tumor growth. Although the reason for this is unclear, no serious toxic effects were observed on high-dose treatment. Therefore, it is necessary to examine the effect of increasing the dose of 186Re-MAG3-HBP on tumor growth using other models.
Bisphosphonates have been used primarily to treat hypercalcemia (from excess bone resorption) and, more recently, cancer-induced bone pain (32). Recent reports indicate that the regular use of bisphosphonates for metastatic bone disease prevents skeletal-related events, reduces bone pain, and improves the patient's quality of life (32,33). Briefly, the mechanism of action includes induction of the apoptosis of osteoclasts, inhibition of the proliferation of cancer cells, and reduction in the production of cytokine and secretion of metalloproteinase. Walker et al. reported that zoledronic acid, a bisphosphonate, was a useful antinociceptive agent in a rat model of metastatic cancer pain (25). These findings raise the possibility that the therapeutic effect of 186Re-MAG3-HBP is attributable not to the β-particles of 186Re but, rather, to the bisphosphonate structure of 186Re-MAG3-HBP. To test this possibility, we treated rats with nonradioactive Re-MAG3-HBP at the same dose as 186Re-MAG3-HBP. In nonradioactive Re-MAG3-HBP–treated rats, tumor growth and the withdrawal response were comparable with those in untreated rats (Figs. 3 and 4). Accordingly, the therapeutic effect of 186Re-MAG3-HBP can be attributed to the β-particles of 186Re.
CONCLUSION
186Re-MAG3-HBP accumulated at the site where tumor cells were injected in a rat model of bone cancer and significantly inhibited tumor growth and attenuated the allodynia induced by bone cancer without having critical myelosuppressive side effects. These results indicate that 186Re-MAG3-HBP could be useful as a therapeutic agent for the palliation of metastatic bone pain.
Acknowledgments
This work was supported in part by a Grant-in-Aid for Scientific Research on Priority Areas from the Ministry of Education, Culture, Sports, Science and Technology of Japan and by a research grant from the Sagawa Foundation for the Promotion of Cancer Research.
Footnotes
-
COPYRIGHT © 2006 by the Society of Nuclear Medicine, Inc.
References
- Received for publication June 26, 2006.
- Accepted for publication September 25, 2006.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}