


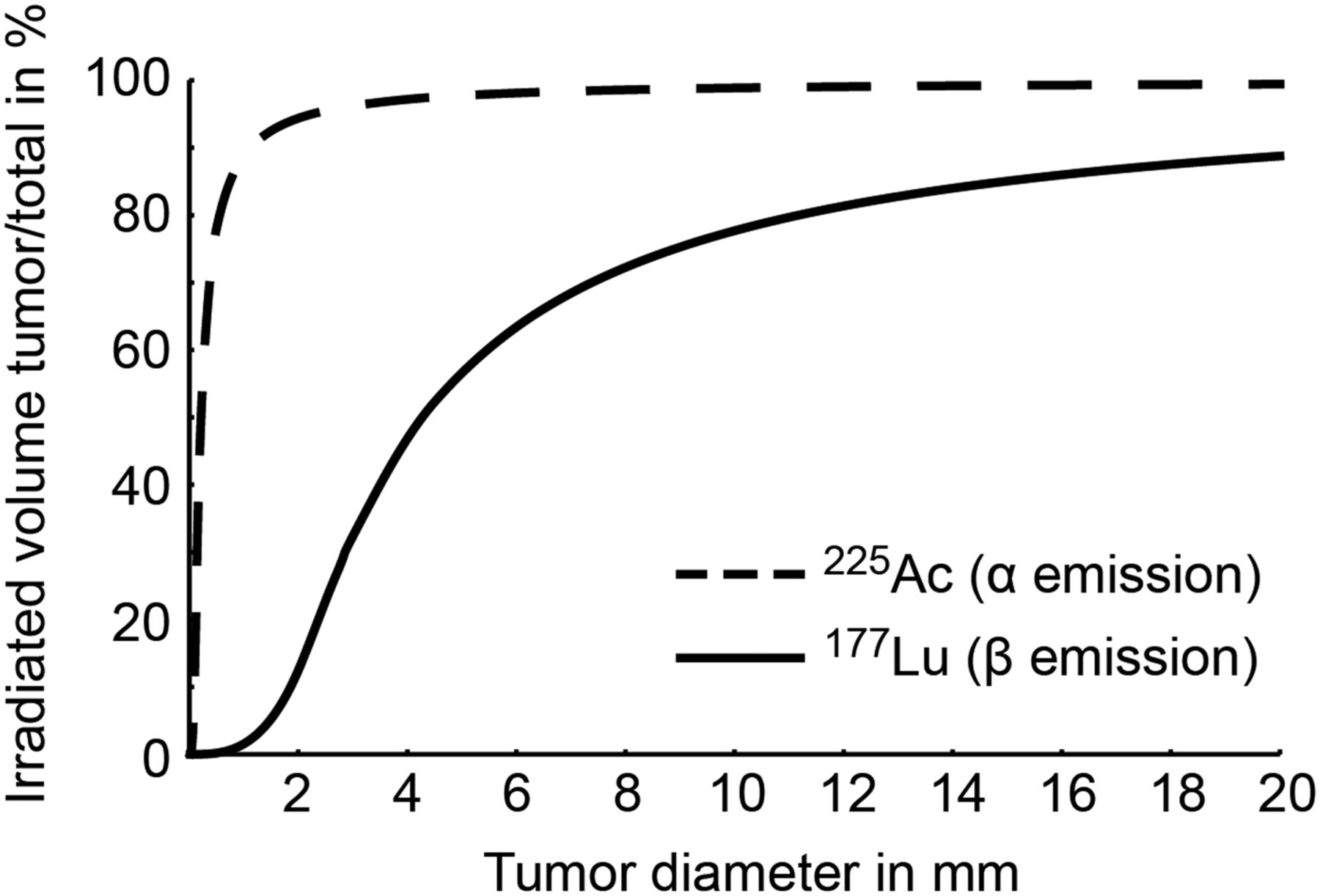
Radionuclide therapy for prostate cancer started more than 70 y ago (1). Nuclear medicine has since evolved considerably to provide a multitude of new imaging and therapy options. The past decade witnessed an unprecedented expansion of radioligands for prostate cancer. Milestones include the first α-emitter for treatment of symptomatic bone metastases (2) and theranostic vectors directed at the prostate-specific membrane antigen (PSMA) or bombesin receptor (3–5). However, current radionuclide therapies are applied at a late stage of the disease aiming at palliation. Despite recent advances for treatment of metastatic prostate cancer, cure remains an unmet need of the 21st century. Cancer spreads early and develops slowly as submillimeter occult lesions. Lesions grow at distant sites and become detectable only when significant morphologic or metabolic alterations have formed, often years to decades after the initial spread (6). Effective ablation of small metastases is critical for cure and presents a specific challenge for β-emitting radionuclide therapy. Millimeter-range β-particles deliver insufficient amounts of radiation to millimeter-size tumor lesions, as energy deposition extends and dilutes beyond lesion boundaries (Fig. 1). α-radiation, because of its micrometer range, targets millimeter-size tumor volumes at higher relative yield (Fig. 1). Further evidence points to a superior biologic effectiveness for α-therapy based on high-linear-energy transfer resulting in frequent double-strand DNA breaks (7). However, are basic advantages of α-therapy associated with a clinical benefit?
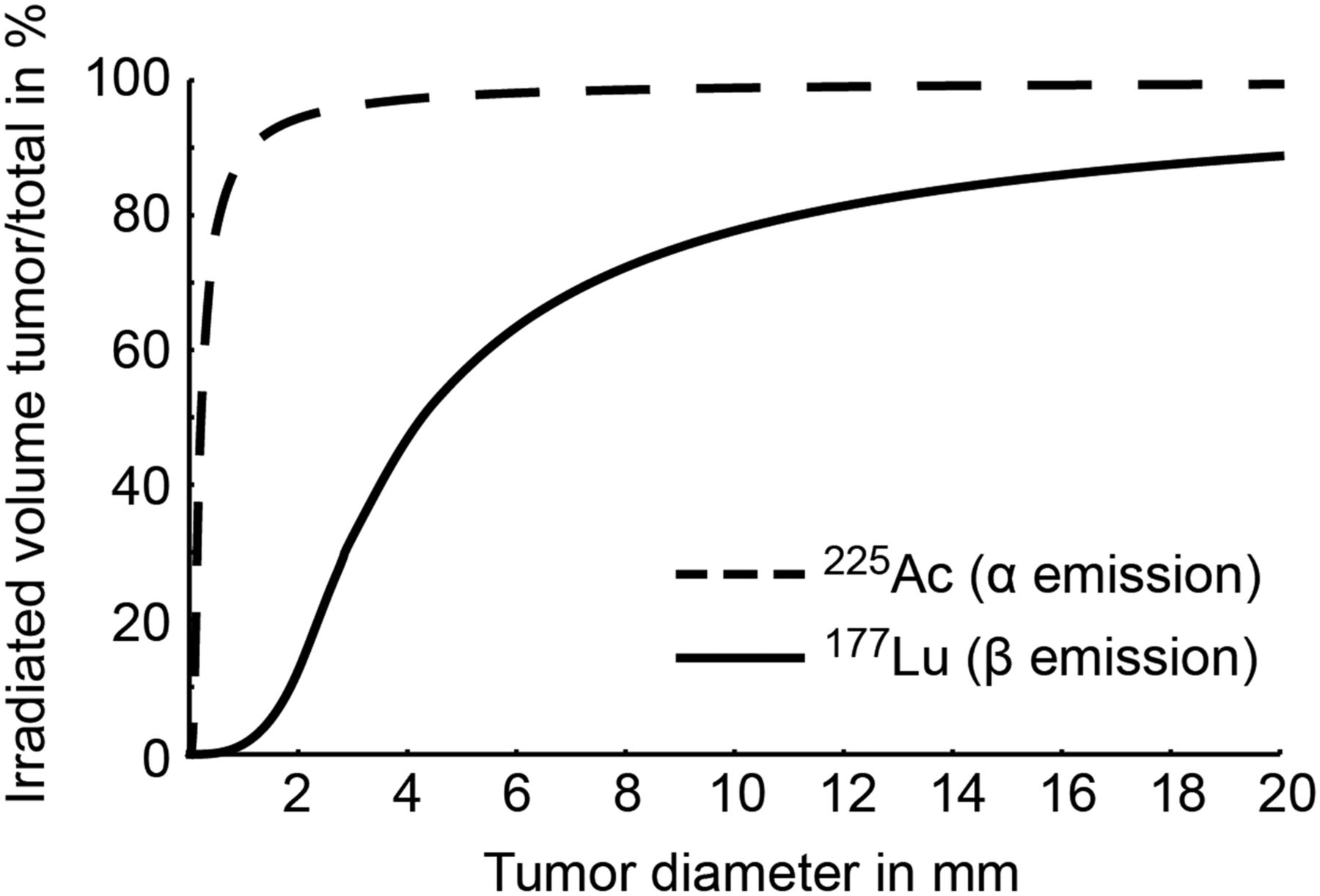
Proportion of targeted tumor volume per total irradiated volume for α- (225Ac) versus β- (177Lu) radioligand therapy of small prostate cancer lesions. Maximum range in tissue is 0.1 mm for α- and 2 mm for β-therapy. Radiation delivered to subcentimeter lesions drops significantly for β-therapy, as energy deposition significantly extends beyond lesion boundaries. The simplified model calculates irradiated volumes assuming homogeneous intratumoral distribution of 225Ac and 177Lu without taking into account any potential difference in biodistribution, energy transfer, and relative biologic effectiveness.
223Ra was the first α-emitter, approved for survival benefit in patients with symptomatic bone metastatic castration-resistant prostate cancer (mCRPC) (2). 223Ra therapy comes with a low rate of serious adverse events (2) thought to be based on sparing of healthy red marrow by the short-range α-particles. On the contrary, β-emitting bone-seeking 153Sm and 89Sr effectively reduce bone pain, however, without evidence for survival benefit and at higher rates for hematologic toxicity (8,9).
223Ra α-therapy has become an important option in the management of mCRPC. However, bone-targeting is of limited value in patients with extraosseous disease (10). Effective targeting of skeletal and extraskeletal disease is achieved by intravenous administration of radiolabeled small ligands for the PSMA (11). 177Lu-labeled PSMA617 induced a prostate-specific antigen drop of more than 50% in about half of mCRPC patients with bone, lymph node, or soft-tissue metastases (12). Significant tumor shrinkage occurred, and in a few patients even complete response was achieved after PSMA-directed radioligand therapy (12–14). However, disease inevitably recurs. Kratochwil et al. were able to salvage 9 of 11 patients with 177Lu-PSMA617–recurrent mCRPC by switching to 225Ac-PSMA617 α-therapy (15). A high response rate was achieved by repeated application of 100 kBq of 225Ac-PSMA617 per kilogram, an α-therapy protocol with acceptable toxicity for salivary glands (15).
Preclinical and clinical evidence indicate higher efficacy for α- than β-based therapy of prostate cancer. Thus, α-therapy should be in the focus of research aimed at the cure of metastatic disease. Several challenges need to be overcome for improved effectiveness and broad clinical implementation. First, a reliable, high-yield, pharmaceutical-grade supply of α-emitter must be established to enable clinical trials and subsequent widespread distribution. For 225Ac, the current annual global supply estimated at 1.2–1.7 Ci would treat fewer than 2,000 patients with 4 cycles of 225Ac-PSMA617. Supply comes nowhere near meeting the estimated demand of 50 Ci listed in the 2008 U.S. Department of Energy report (16). Several alternative production methods were evaluated, including low-energy proton irradiation of 226Ra (17) and high-energy proton irradiation of 232Th (18) in a cyclotron. However, chemical processing and large-scale production methods are still under development. Second, prospective, multicenter clinical trials need to be conducted. Recently, NETTER-1 and ALSYMPCA established new radionuclide therapies by reporting improved progression-free and overall survival (2,19). Both studies may serve as a role model for future trial designs aimed at approval and reimbursement of α-therapy. Third, given the favorable safety of 223Ra and 225Ac-PSMA617, α-therapy should be performed at an earlier stage of the disease. The combination of surgery, adjuvant radionuclide therapy, and hormonal therapy has the potential to cure metastatic disease, a key lesson learned almost one century ago from the application of radioiodine in patients with differentiated thyroid cancer (20). Likewise, adjuvant PSMA-directed α-therapy may cure, when performed early and in conjunction with other systemic treatment. Finally, α-therapy should be evaluated in combination with potentially synergistic pharmacologic approaches. α-radiation induces replication stress, characterized by the accumulation of double-strand DNA breaks (21). Small-molecule inhibitors of double-strand DNA break repair pathways demonstrated antitumor properties in preclinical models and are being investigated in more than 50 active clinical trials (22). The combination of PSMA-directed α-therapy with inhibitors of double-strand DNA break repair may potentiate efficacy at low toxicity. Furthermore, the combination with inhibitors of the androgen receptor may enhance radiation delivery by increased PSMA expression on tumor cells (23–25).
In summary, α-therapy is effective in patients with metastatic prostate cancer. Short-range α-emission targets small lesions more effectively than β-radiation. Given this advantage, cure of metastatic disease should be the ultimate goal of future α-therapy research. In this intent, the evaluation of early treatment and systemic PSMA-directed α-therapy in conjunction with synergistic pharmacologic approaches are highly encouraged.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank Dr. Norbert Müller for help with calculation of 225Ac and 177Lu radiation volumes.
Footnotes
Published online Sep. 21, 2017.
- © 2017 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication September 5, 2017.
- Accepted for publication September 11, 2017.





{kind=link}