


Abstract
Recently, troglitazone has emerged as an insulin sensitizer for the treatment of type II diabetes. However, its effect on skeletal muscle glucose use (SMGU) has not been studied. Methods: To investigate the effect of troglitazone on SMGU in patients with type II diabetes, we undertook skeletal muscle 18F-FDG PET dynamic imaging under insulin clamping before and after administration of SMGU to 20 patients with type II diabetes. Data were compared with those for 12 age-matched healthy volunteers. Results: The whole-body glucose disposal rate (GDR) was significantly lower in patients (29.9 ± 9.83 μmol/min/kg) than in control subjects (55.6 ± 16.5 μmol/min/kg, P < 0.01), as was the SMGU (patients, 3.27 ± 2.17 μmol/min/kg; control subjects, 10.9 ± 6.4μmol/min/kg; P < 0.01). After the therapy, GDR significantly improved in patients (29.3 ± 14.6 μmol/min/kg, P < 0.05), as did SMGU (5.06 ± 2.11 μmol/min/kg, P < 0.05). When results for patients with and without hypertension were separately analyzed, a significant improvement in SMGU after troglitazone was seen in both normotensive and hypertensive patients (normotensive [n = 10]: baseline, 3.67 ± 2.89 μmol/min/kg; after therapy, 5.28 ± 2.61 μmol/min/kg; P < 0.05; hypertensive [n = 10]: baseline, 2.89 ± 1.22 μmol/min/kg; after therapy, 4.72 ± 1.39 μmol/min/kg; P < 0.05). GDR in patients with and without hypertension was significantly improved by troglitazone (normotensive: baseline, 17.9 ± 10.2 μmol/min/kg; after therapy, 31.9 ± 15.9 μmol/min/kg; P < 0.01; hypertensive: baseline, 39.6 ± 15.1 μmol/min/kg; after therapy, 47.7 ± 23.8 μmol/min/kg; P < 0.05). The plasma free fatty acid concentration during insulin clamping was not changed by troglitazone (baseline, 1.1 ± 0.86 mEq/L; after therapy, 0.93 ± 0.65 mEq/L; P = not significant). Conclusion: Troglitazone can improve whole-body insulin resistance through the improvement of SMGU but not through a decline in plasma free fatty acid concentration in patients with type II diabetes with or without hypertension.
- troglitazone
- insulin resistance
- skeletal muscle glucose metabolism
- PET
- insulin sensitizer
- type II diabetes
Impaired peripheral tissue glucose use, or insulin resistance, has been reported for patients with type II diabetes (1–3). Several factors, including impaired skeletal muscle glucose use (SMGU), reduced peripheral blood flow (4), increased hepatic gluconeogenesis (5), and an increase in plasma free fatty acid (FFA) concentration (6,7), contribute to insulin resistance. Among these factors, SMGU is thought to play a central role in the pathogenesis of insulin resistance. The effect of therapy on insulin resistance as determined by the whole-body glucose disposal rate (GDR) has been shown (1–3); however, the specific effect of medications on SMGU in patients with type II diabetes has not been investigated.
Troglitazone is in a new class of oral hypoglycemic agents that act as insulin sensitizers (8,9). The effect of troglitazone on muscle metabolism in the rat hind limb has been reported experimentally (10–12). An in vitro experimental study on cultured skeletal muscle cells suggested an improvement in glucose metabolism in obese patients with type II diabetes (13). However, the in vivo effect of troglitazone on SMGU in patients with type II diabetes and the relationship between troglitazone administration and whole-body insulin resistance have not been investigated. Also not studied has been the effect of troglitazone on SMGU in patients with type II diabetes who also have hypertension. In addition, whether the plasma FFA concentration is related to the effects of troglitazone on insulin resistance and SMGU is not clear.
PET allows in vivo quantitative analysis of tissue metabolism. In particular, PET has been used in research on quantitative analysis of muscle glucose metabolism in vivo (14–24) using 18F-FDG as the tracer. In this study, we succeeded in quantifying SMGU in patients with type II diabetes to assess the effects of troglitazone on SMGU.
MATERIALS AND METHODS
Study Subjects
We studied 20 asymptomatic patients with type II diabetes (13 men, 7 women; mean age, 53.0 ± 10.7 y) and 12 asymptomatic age-matched healthy volunteers who were selected according to the criteria of Rozanski et al. (25) (10 men, 2 women; mean age, 48.5 ± 9.88 y). All patients had been treated only with dietary changes before this investigation. After the first evaluation of insulin resistance and SMGU as determined by PET, troglitazone (400 mg/day) was prescribed. Between 4 and 6 mo after the first PET study, insulin resistance and SMGU were reevaluated. The control subjects did not receive troglitazone. Between 4 and 6 mo after the initiation of troglitazone therapy, all patients underwent a second evaluation of insulin resistance. The control subjects were evaluated only once. Patients with angina pectoris, heart failure, or significant coronary artery disease were excluded. The general characteristics of the study subjects are shown in Table 1. Before this study, we informed all subjects of its nature, after which they agreed to participate in the protocol, which was approved by the local ethics committee.
General Characteristics of Study Subjects
PET
Preparation of FDG.
18F was synthesized using a Cypris model 370 cyclotron (Sumitomo JYUKI Industries, Ltd., Kyoto, Japan), and FDG was synthesized with an automated system based on the method reported by Ehrenkaufer et al. (26). Radiochemical purity was >95%.
Acquisition of Myocardial Metabolic Images.
Myocardial FDG images were obtained using a Headtome IV PET scanner (Shimadzu, Kyoto, Japan). This PET scanner has 7 imaging planes; in-plane resolution is 4.5-mm full width at half maximum (FWHM), and the z-axial resolution is 9.5-mm FWHM. Effective in-plane resolution was 7 mm after using a smoothing filter. The sensitivities of the scanner are 14 and 24 kcps (MBq/mL) for direct and cross planes, respectively (27).
After acquisition of transmission data for correct photon attenuation, we injected FDG (185–370 MBq) and collected dynamic PET data for both the thoracic region and the femoral region. Two hours before the injection of FDG, hyperinsulinemic euglycemic clamping was started to keep the plasma glucose concentration at a constant level of 95–105 mg/dL. Insulin clamping was continued during the entire PET scan. During this interval, we obtained 19 dynamic scans for the thoracic region and 5 dynamic scans for the femoral region using the following protocol: nine 10-s, three 30-s, two 120-s, four 300-s, and one 600-s scan for the thoracic region and one 120-s and four 300-s scans for the femoral region.
Quantification of SMGU
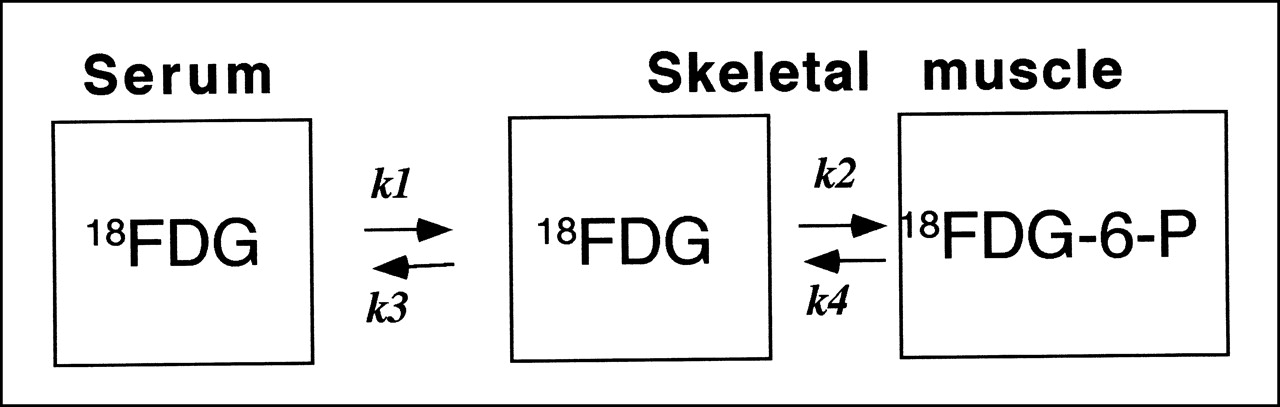
The amount of glucose metabolized by femoral muscle was determined by calculating the SMGU. Following the method of Ohtake et al. (20), we obtained the time–activity curve of the descending aorta corrected by venous blood samplings. Input function for femoral muscle SMGU was composed by combining the time–activity curve of the descending aorta and 5 arterialized venous blood samplings during the femoral muscle dynamic PET scan. Using the input function, we determined k1 × k3/(k2 + k3) = [Ki] by Patlak graphic analysis and calculated SMGU by substituting Ki in the equation SMGU = [Ki] × (BG1 + BG2 + BG3)/3/LC. K1, k2, and k3 were rate constants of the chemical formula shown in Figure 1; k4 was assumed to be 0 in skeletal muscle (16–18). BG1, BG2, and BG3 were serum glucose concentrations during the dynamic PET scan using FDG as shown. LC stands for lumped constant, which was calculated to be 1.0 in skeletal muscle cells, as reported in human studies (16–18).
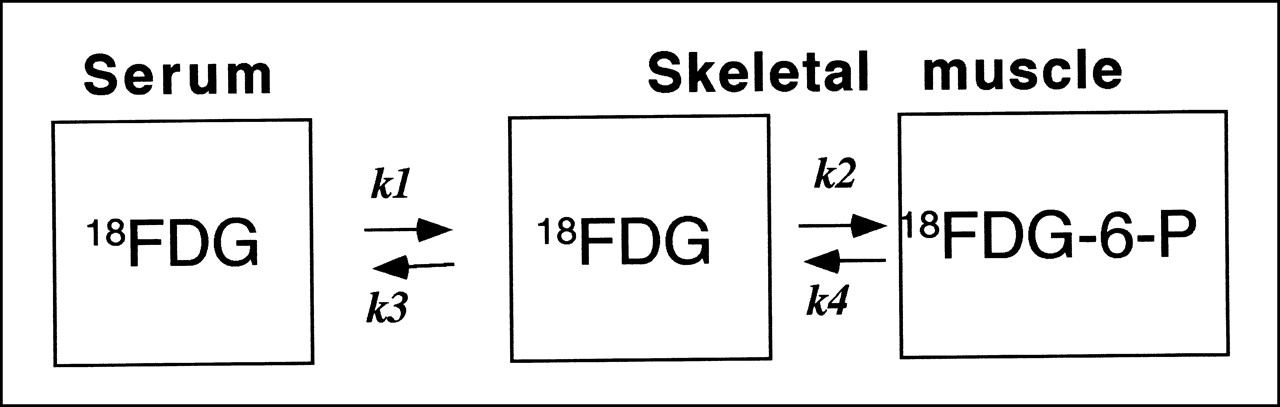
Schematic representation of 3-compartment FDG tracer kinetic model. k4 is assumed to be 0 in skeletal muscle. Difference between FDG and glucose was calculated to be 1.0 in skeletal muscle cells as reported in human studies. 18FGD-6-P = FDG-6-phosphate.
All data were corrected for dead-time effects to reduce error to <1%. To avoid the influence of the partial-volume effect associated with the size of the object, we used recovery coefficients obtained from experimental phantom studies in our laboratory. The recovery coefficient was 0.8 for a 10-mm object and 1.0 for a >30-mm object. In our program, the recovery coefficient to measure the SMGU of the femoral region was considered to be 1.0.
To calculate the rate of tissue glucose use, we used an Ultra-30 high-speed image processing system (Sun Microsystems Japan, Tokyo, Japan) with Dr. View software (Asahi Kasei Information System Co., Ltd., Tokyo, Japan).
Data were collected after hyperinsulinemic euglycemic clamping to maintain a stable serum glucose concentration of 95–105 mg/dL by simultaneous infusion of insulin (1 mU/min/kg) at a fixed rate and glucose at a variable rate. Whole-body insulin resistance was measured by obtaining the GDR during hyperinsulinemic euglycemic clamping (μmol/min/kg) using a reported method (28). During the PET scan, insulin clamping was continued to keep the fasting plasma blood glucose concentration constant at 95–105 mg/dL.
Statistical Analysis
Data consisting of 2 parameters were analyzed by the 2-tailed Student t test. P < 0.05 was considered statistically significant. Values were expressed as mean ± SD. Multivariate stepwise regression analysis was used to examine which factors were independently related to SMGU among FFA, age, GDR, fasting plasma blood glucose concentration, hemoglobin A1c, systolic blood pressure, diastolic pressure, duration of diabetes, and sex.
RESULTS
Effect of Troglitazone on GDR and SMGU
The GDR was significantly lower in patients (29.9 ± 9.83 μmol/min/kg) than in control subjects (55.6 ± 16.5 μmol/min/kg, P < 0.01), as was the SMGU (patients, 3.27 ± 2.17 μmol/min/kg; control subjects, 10.9 ± 6.44 μmol/min/kg; P < 0.01). After therapy, GDR significantly improved in patients (39.3 ± 14.6 μmol/min/kg, P < 0.05), as did SMGU (5.06 ± 2.11 μmol/min/kg, P < 0.05).
When results for patients with and without hypertension were separately analyzed, a significant improvement in SMGU after troglitazone was seen in both normotensive and hypertensive patients (normotensive [n = 10]: baseline, 3.67 ± 2.89 μmol/min/kg; after therapy, 5.28 ± 2.61 μmol/min/kg; P < 0.05; hypertensive [n = 10]: baseline, 2.89 ± 1.22 μmol/min/kg; after therapy, 4.72 ± 1.39 μmol/min/kg; P < 0.05). GDR in patients with and without hypertension was significantly improved by troglitazone (normotensive: baseline, 17.9 ± 10.2 μmol/min/kg; after therapy, 31.9 ± 15.9 μmol/min/kg; P < 0.01; hypertensive: baseline, 39.6 ± 15.1 μmol/min/kg; after therapy, 47.7 ± 23.8 μmol/min/kg; P < 0.05) (Table 2).
Results for Type II Diabetic Patients With and Without Hypertension
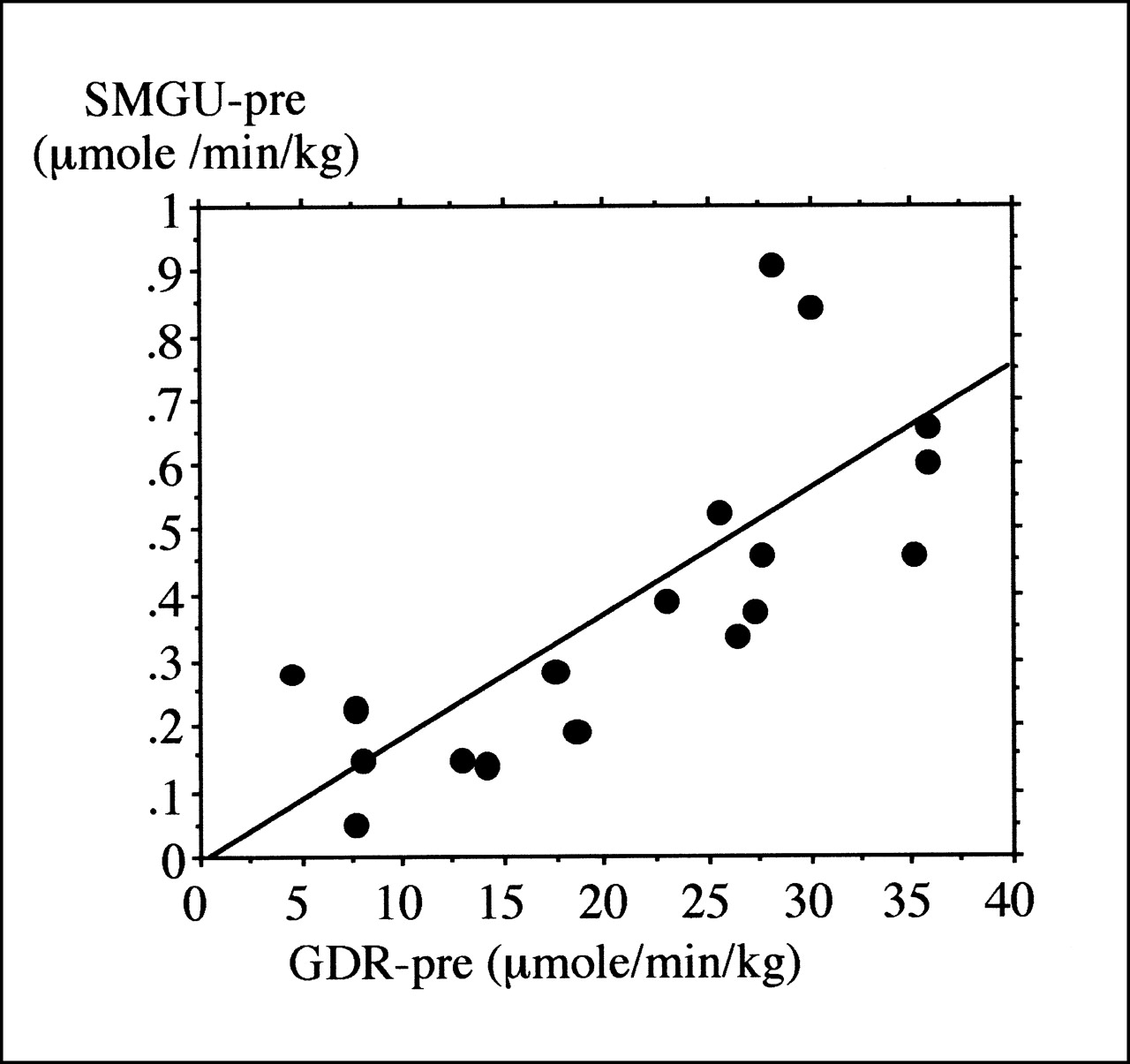
A significant positive relationship was seen between GDR and SMGU before therapy (r = 0.75; P < 0.01) (Fig. 2), and this relationship became much more apparent after troglitazone therapy (r = 0.77; P < 0.01) (Fig. 3). FDG PET functional imaging also showed an improvement in the SMGU of femoral muscle in the patients whose insulin resistance improved with troglitazone. However, static femoral muscle FDG imaging did not show this improvement to reach the level shown in the control subjects (Fig. 4).
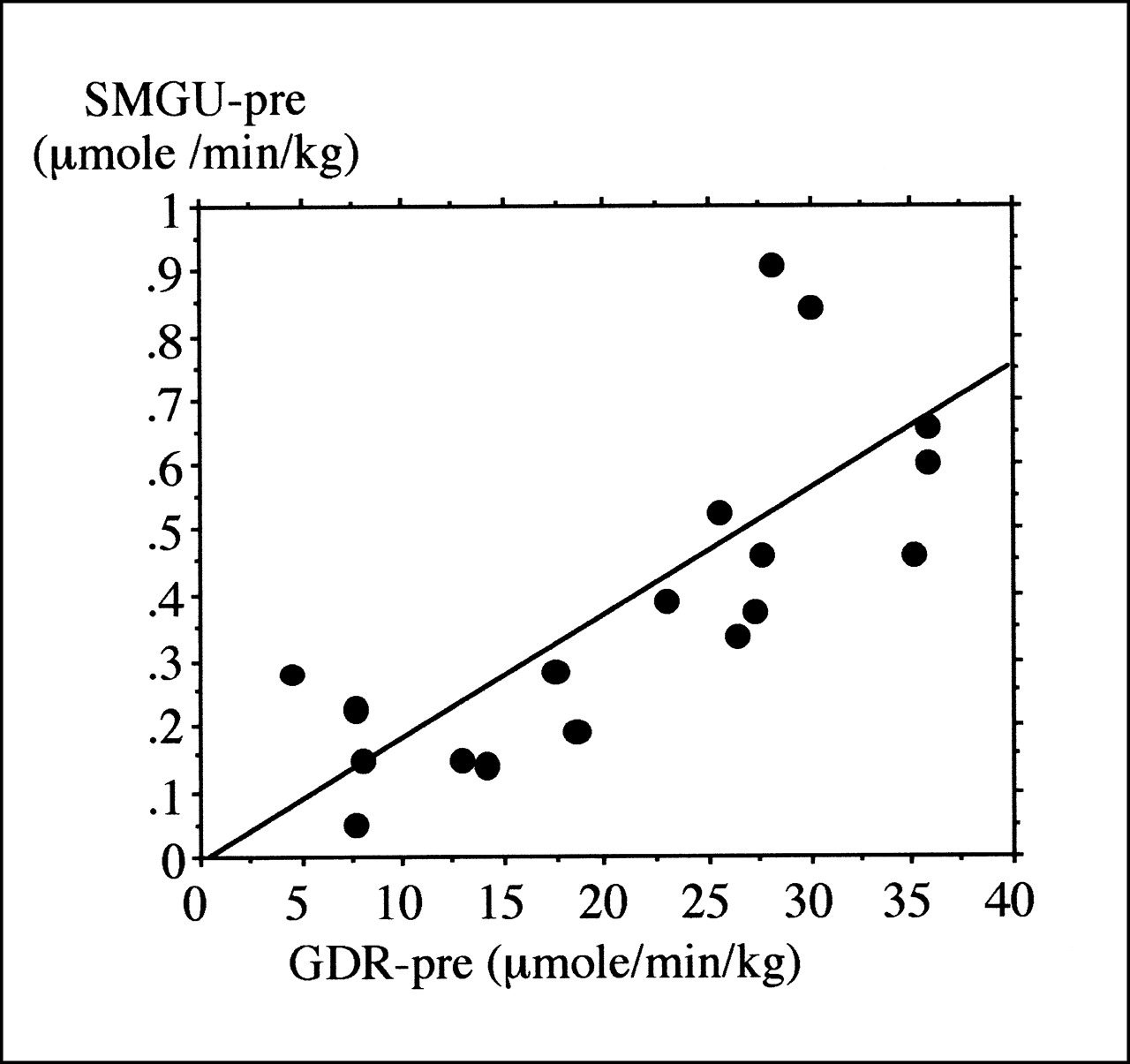
GDR and SMGU show significant positive relationship (r = 0.75; P < 0.01).
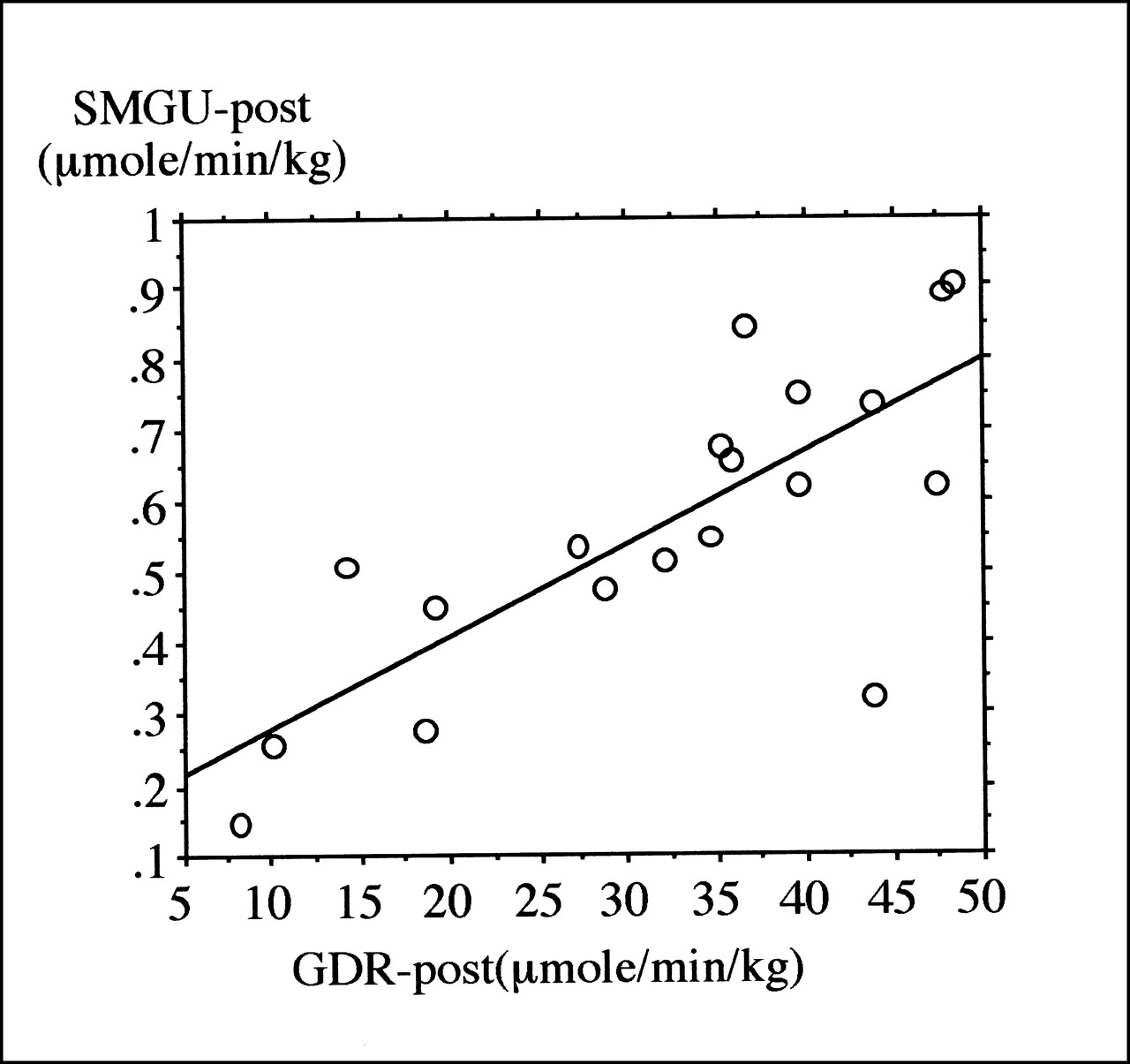
Significant positive relationship between GDR and SMGU is more apparent after troglitazone therapy (r = 0.77; P < 0.01).
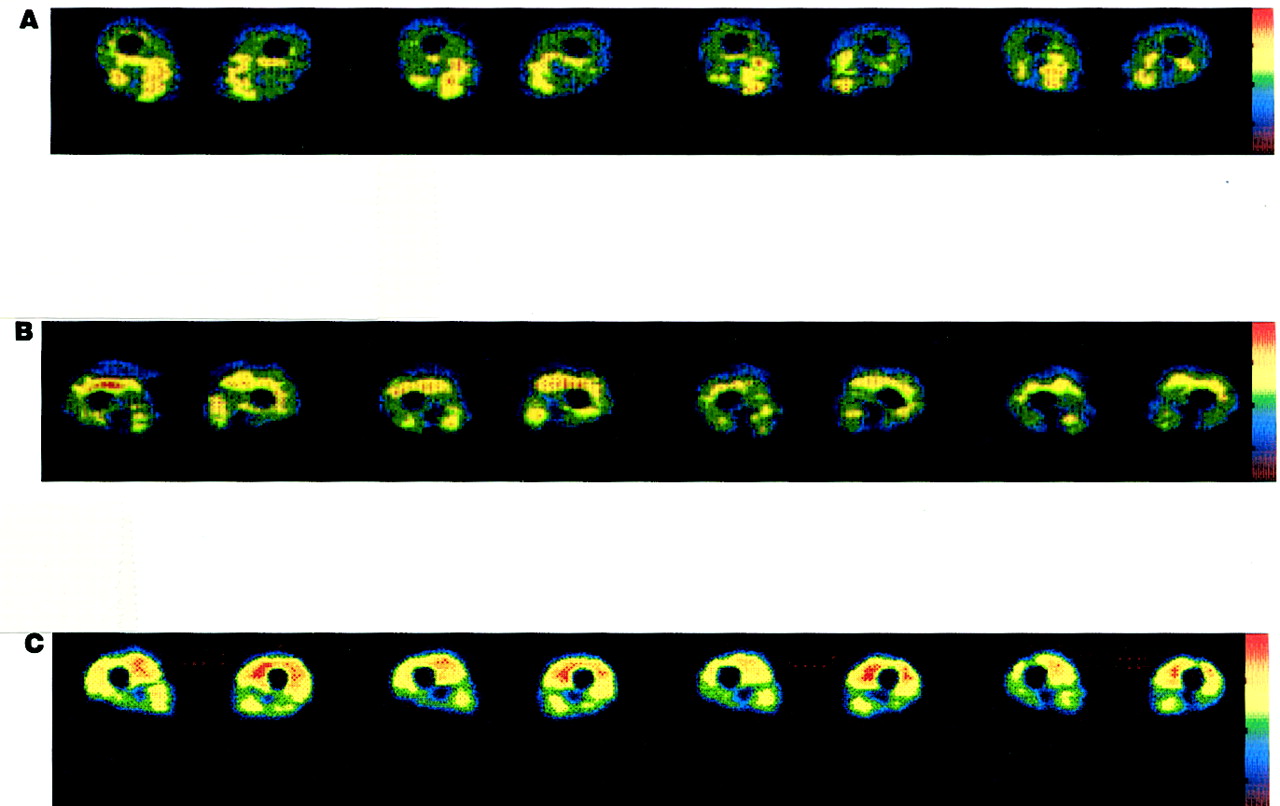
FDG PET images of femoral muscle. (A) In patients with type II diabetes before troglitazone therapy, images show irregular and relatively reduced FDG uptake compared with that after therapy and in control subjects. (B) After troglitazone therapy, images show improvement in irregular and relatively reduced FDG uptake, especially in anterior part, but not to level seen in control subjects. (C) In control subjects, images show apparently homogeneous FDG uptake compared with that in patients with type II diabetes.
Serum Glucose Concentration
The plasma fasting glucose concentration was significantly higher in patients before therapy (8.28 ± 0.87 mmol/L) than in control subjects (5.21 ± 0.79 mmol/L, P < 0.01) and was significantly reduced after therapy (7.22 ± 1.84 mmol/L, P < 0.01). During hyperinsulinemic euglycemic clamping, the average serum glucose concentration was the same in patients (5.21 ± 0.87 mmol/L) as in control subjects (4.79 ± 0.78 mmol/L).
Serum Insulin Concentration
Serum insulin concentration in patients during hyperinsulinemic euglycemic clamping (52 ± 20 μU/mL) was comparable with that in control subjects (54 ± 29 μU/mL). Serum insulin concentration at the beginning of the dynamic PET scan did not significantly differ from that at the end. Plasma fasting insulin concentration in patients before therapy (7.9 ± 4.3 μU/mL) was significantly higher than that in control subjects (1.8 ± 0.4 μU/mL). However, this value after therapy (7.1 ± 4.9 μU/mL) tended to be decreased compared with pretherapy values but remained significantly higher than values for control subjects. No significant relationship was seen between SMGU and plasma insulin concentration in the patients.
Serum FFA Concentration
Serum FFA concentration was significantly higher in patients during insulin clamping (1.1 ± 0.86 mEq/L) than in control subjects (0.32 ± 0.19 mEq/L, P < 0.05) but was not significantly reduced after therapy (0.93 ± 0.65 mEq/L, P = not significant). In addition, plasma fasting FFA concentration was also significantly higher in patients (1.32 ± 0.65 mEq/L) than in control subjects (0.41 ± 0.11 mEq/L, P < 0.01). Plasma fasting FFA concentration after therapy (1.06 ± 0.85) was comparable with that before therapy and also significantly higher than that in control subjects (P < 0.01). No significant relationship was seen between plasma FFA concentration during insulin clamping and the GDR before and after therapy.
DISCUSSION
Troglitazone is a new oral hypoglycemic agent that treats type II diabetes through improvement of insulin resistance (8). Several factors, including impaired SMGU, reduced peripheral blood flow, hepatic gluconeogenesis, and altered plasma FFA metabolism (7), can be involved in the progression of insulin resistance. Although the effect of troglitazone as an insulin sensitizer has been well acknowledged experimentally (8–10), the specific effect of troglitazone on SMGU in patients with type II diabetes has not been visualized and quantified in vivo. Furthermore, whether such an effect extends to patients having both type II diabetes and hypertension has not been clear, although hypertension can be associated with insulin resistance. Finally, the effect of an elevated FFA concentration in relation to the effect of troglitazone on insulin resistance has not been studied. Our current study showed that a reduced whole-body insulin resistance as well as SMGU could be improved by troglitazone in patients with type II diabetes. Furthermore, this improvement in SMGU, as well as in whole-body insulin resistance, was not affected by the coexistence of essential hypertension. Moreover, heterogeneously impaired femoral muscle FDG uptake, which is usually associated with insulin resistance, improved after the troglitazone therapy. These are novel findings.
A relationship between plasma FFA concentration and insulin resistance has been reported for patients with type II diabetes (29,30). We found that the plasma FFA concentration during insulin clamping was not changed before and after therapy with troglitazone, whereas SMGU and GDR were significantly improved. This finding indicates that the FFA concentration was not a factor in the improvement of insulin resistance or SMGU after the administration of troglitazone. These results suggest that troglitazone can improve whole-body insulin resistance by directly improving SMGU in patients with type II diabetes without the enhancement of the glucose–FFA cycle or inhibition of hepatic gluconeogenesis. Moreover, our current results strongly suggest that the main effect of troglitazone in the improvement of SMGU or GDR is not induced by a modification of the glucose–FFA cycle in patients with type II diabetes. Although the mechanism by which troglitazone increases SMGU remains speculative, possible factors include the activation of the peroxisome proliferator–activated receptor (PPAR-γ) in adipocytes (31,32) and the increase in the number of small adipocytes and inactivation of tumor necrotizing factor-α through the activation of PPAR-γ in adipocytes (33). Upregulation of gene expression of PPAR-γ in skeletal muscle cells by troglitazone may be another mechanism for the improvement of SMGU in patients with type II diabetes. Enhancement of both glucose transporter 1 messenger RNA and glucose transporter 1 protein but not glucose transporter 4 in patients with type II diabetes can also be a mechanism by which troglitazone increases SMGU (13). All these possibilities suggest that enhancement of SMGU can occur independently of the plasma FFA concentration and are consistent with our current results.
Because SMGU has been thought to be the major factor contributing to whole-body insulin resistance in type II diabetes (8,12,13), quantification of SMGU is important in characterizing troglitazone as an insulin sensitizer. Recently, the results of an in vitro study with cultured skeletal muscle cells in patients with type II diabetes suggested that troglitazone can increase SMGU (13). However, the use of cultured cells has some limitations. Cultured skeletal muscle cells may differ from the in vivo skeletal muscle cells of diabetic patients in reflecting pathophysiologic features, especially with reference to insulin resistance. Cell culture requires invasive muscle biopsy and much time to acquire the final results, making this technique inappropriate for determining responses to drugs. Finally, the influence of plasma FFA cannot be assessed through the use of cultured cells. Therefore, the effects of troglitazone on SMGU need to be ascertained in vivo in patients with type II diabetes. The specific effect of troglitazone on SMGU in the in vivo femoral muscle tissue of patients with type II diabetes had not been investigated previously, especially with reference to the effects of FFA and hypertension. Our current in vivo study clearly showed the effectiveness of troglitazone in improving SMGU in patients with type II diabetes.
As to validity of using FDG PET methodology to quantify SMGU, FDG is essentially metabolized by hexokinase but not by glucokinase. Because the latter is the major enzyme in hepatic cells, the change in GDR should be associated mainly with SMGU. The good correlation between GDR and SMGU seen in our current results supports the validity of using FDG PET methodology to quantify SMGU. Therefore, the influence of methodologic factors on our results, especially as to effect of troglitazone on SMGU, can be negated.
Although our results indicated that troglitazone can improve insulin resistance by improving SMGU in patients with type II diabetes, and although no serious side effects were seen during follow-up of our study patients, troglitazone has been withdrawn from the U.S. market because of serious side effects. Therefore, although our findings cannot be applied directly by clinicians, further studies of other approved agents in this class may confirm the results shown here.
CONCLUSION
Troglitazone can improve SMGU in patients with type II diabetes with or without hypertension. The plasma FFA concentration was not related to the improvement of insulin resistance and SMGU through the use of troglitazone.
Footnotes
Received Nov. 17, 2000; revision accepted Mar. 9, 2001.
For correspondence or reprints contact: Ikuo Yokoyama, MD, 7-3-1 Hongo, Bunkyo-ku, Tokyo, Japan 113-8655.




{kind=link}
{kind=link}
{kind=link}
{kind=link}