


Abstract
This review deals with noninvasive imaging for risk stratification and with a conceptual approach to the selection of noninvasive tests in patients with suspected or known chronic coronary artery disease (CAD). Already widely acknowledged with SPECT, there is an increasing body of literature data demonstrating that CT coronary calcium assessment is also of prognostic value. The amount of coronary atherosclerosis, as can be extrapolated from CT coronary calcium score, has been shown to be highly predictive of cardiac events. The principal difference between myocardial perfusion SPECT (MPS) and CT coronary calcium for prognostic application appears to be that the former is an excellent tool for assessing short-term risk, thus effectively guiding decisions regarding revascularization. In contrast, the atherosclerosis imaging methods are likely to provide greater long-term risk assessment and, thus, are more useful in determination of the need for aggressive medical prevention measures. Although the more recent development of CT coronary angiography is promising for diagnosis, there has been no information to date regarding the prognostic value of the CT angiographic data. Similarly, cardiac MRI has not yet been adequately studied for its prognostic content. The selection of the most appropriate test for a given patient depends on the specific question being asked. In patients with a very low likelihood of CAD, no imaging test may be required. In screening the remaining asymptomatic patients, atherosclerosis imaging may be beneficial. In symptomatic patients, MPS, CT coronary angiography, and cardiac MRI play important roles. We consider it likely that, with an increased emphasis on prevention and a concomitant aging of the population, many forms of noninvasive cardiac imaging will continue to grow, with nuclear cardiology continuing to grow.
- cardiac computed tomography
- cardiac magnetic resonance
- myocardial perfusion SPECT
- coronary artery disease
Noninvasive testing can provide useful information for risk stratification in the chronic coronary artery disease (CAD) patient. Patients who have limiting angina are usually taken directly to cardiac catheterization for consideration of revascularization; however, for the asymptomatic or mildly symptomatic patient, noninvasive assessment of cardiac risk is increasingly being used to determine the need for aggressive medical therapy and to select patients for catheterization (1–3).
PROGNOSTIC APPLICATIONS OF MYOCARDIAL PERFUSION SPECT (MPS)
Stress gated MPS is the most commonly used and well-documented noninvasive method for risk stratification. It is most cost-effective in patients with a clinically intermediate risk of a subsequent cardiac event (1–3). This application has been recently summarized in ACC/AHA/ASNC (American College of Cardiology/American Heart Association/American Society of Nuclear Cardiology) guidelines (4). In general, cardiac mortality is considered, with low risk < 1%, high risk > 3%, and intermediate risk 1%−3% (5). In chronic CAD, it has been suggested that a mortality rate of >3% per year can be used to identify patients with minimal symptoms whose mortality rate can be improved by myocardial revascularization (4,6). The 1%−3% range for intermediate risk would be scaled up for patients who are very elderly or have serious comorbidities, due to increased mortality in all subgroups of these patients. Also, patients whose known or suspected CAD is seriously affecting quality of life or functional status should be considered catheterization candidates irrespective of risk status.
POST-MPS PATIENT OUTCOMES
Two basic tenets, confirmed by extensive literature evidence, are behind the acceptance of MPS for risk stratification: a normal MPS study defines patients at low risk for subsequent cardiac events (2,3), and risk increases exponentially with worsening perfusion abnormality (7,8). Because of this evidence, physicians today can comfortably manage most patients with normal MPS without resorting to myocardial revascularization, confident that angiographic assessment is unlikely to yield further benefit. At the other end of the spectrum, extensive or severe perfusion defects define high risk and usually lead to coronary angiography.
The need for consideration of revascularization in patients with only mild perfusion abnormalities is less clear. Though many such patients may not need such consideration, there are subgroups of patients with mild perfusion abnormalities who might require coronary angiography on the basis of other high-risk scan information—for example, patients with a low ejection fraction (9), transient ischemic dilation of the left ventricle (10), increased lung uptake, or other clinical information suggesting high risk (e.g., diabetes (11), atrial fibrillation (12), those undergoing adenosine stress (13), high pretest likelihood of CAD (14,15), very abnormal stress electrocardiogram (ECG) (16)).
Although the greatest numbers of patients for risk stratification have been reported with 99mTc-sestamibi stress MPS, similar findings have been shown with 201Tl (17) and, more recently, 99mTc-tetrofosmin (18). These findings have resulted in a large number of class I indications for MPS in risk assessment of patients with an intermediate or high likelihood of CAD (4).
ADDED VALUE OF FUNCTION PARAMETERS FROM MPS
Recent reports show that risk assessment with MPS is improved if functional assessments of ejection fraction (9) and end-systolic volume (19) from gated SPECT measurements are considered as well as transient ischemic dilation of the left ventricle (10). Nonnuclear parameters such as the hemodynamic responses to adenosine (20) or exercise (21) also add value.
USING MPS FOR DECIDING BETWEEN MEDICAL AND REVASCULARIZATION THERAPY
Beyond risk stratification, MPS can identify patients who are likely to benefit from revascularization (Fig. 1). In the setting of no or mild ischemia, patients undergoing medical therapy as their initial treatment have been shown to have survival superior to that of patients referred for revascularization. On the other hand, when moderate-to-severe ischemia (>10% of the total myocardium ischemic) was detected by MPS, patients undergoing revascularization have shown an increased survival benefit over patients undergoing medical therapy. The importance of predicting benefit appears to hold across ejection fraction levels (22). The findings of these studies suggest a new paradigm: rather than only identifying patient risk, MPS in a testing strategy can identify which patients may benefit from revascularization.
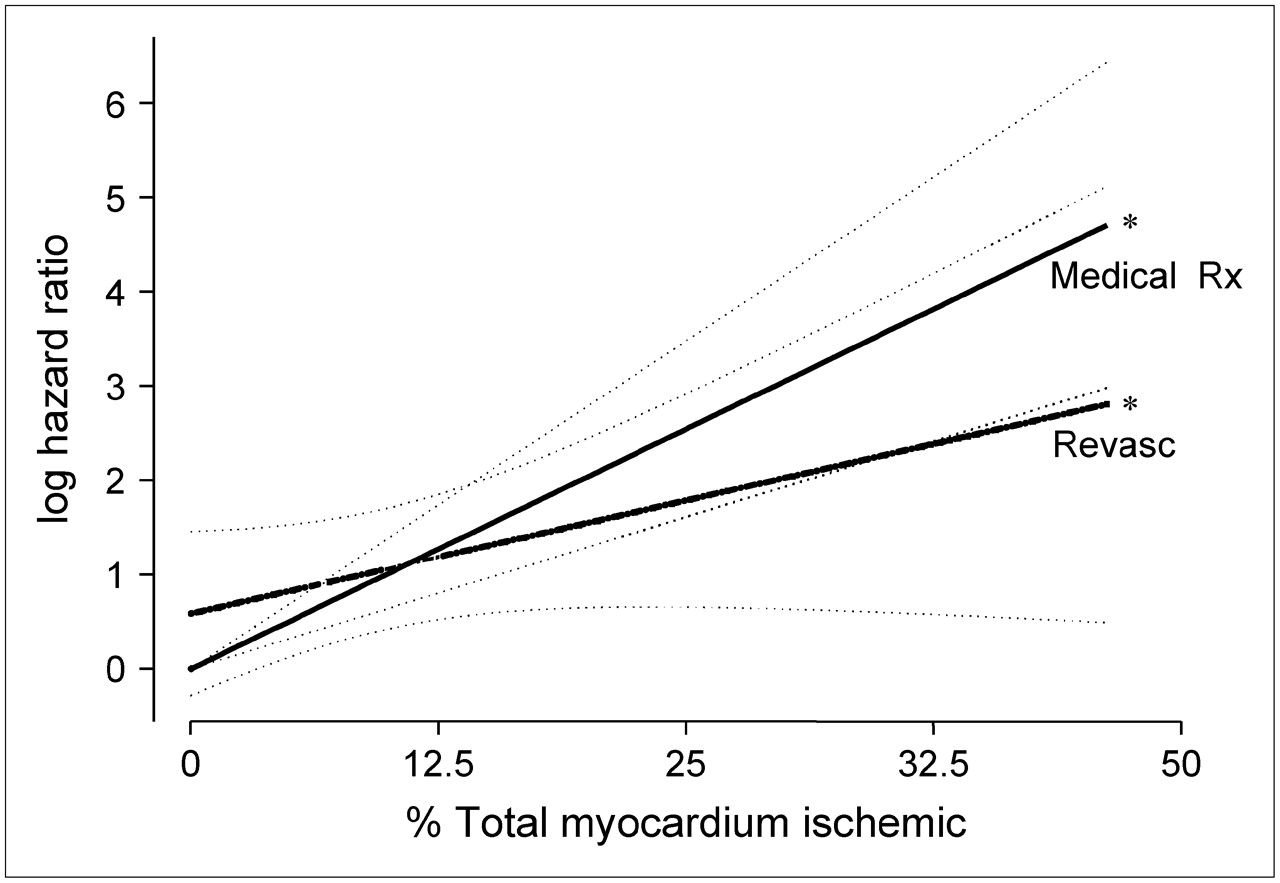
Log hazard ratio for revascularization vs. medical therapy (medical Rx) as a function of the percentage myocardium ischemic on the basis of final Cox proportional hazards model. Revasc = revascularization. *Model P < 0.0001; interaction P = 0.0305. (Adapted with permission from (8).)
PROGNOSTIC SIGNIFICANCE OF CORONARY CALCIUM SCORE (CCS)
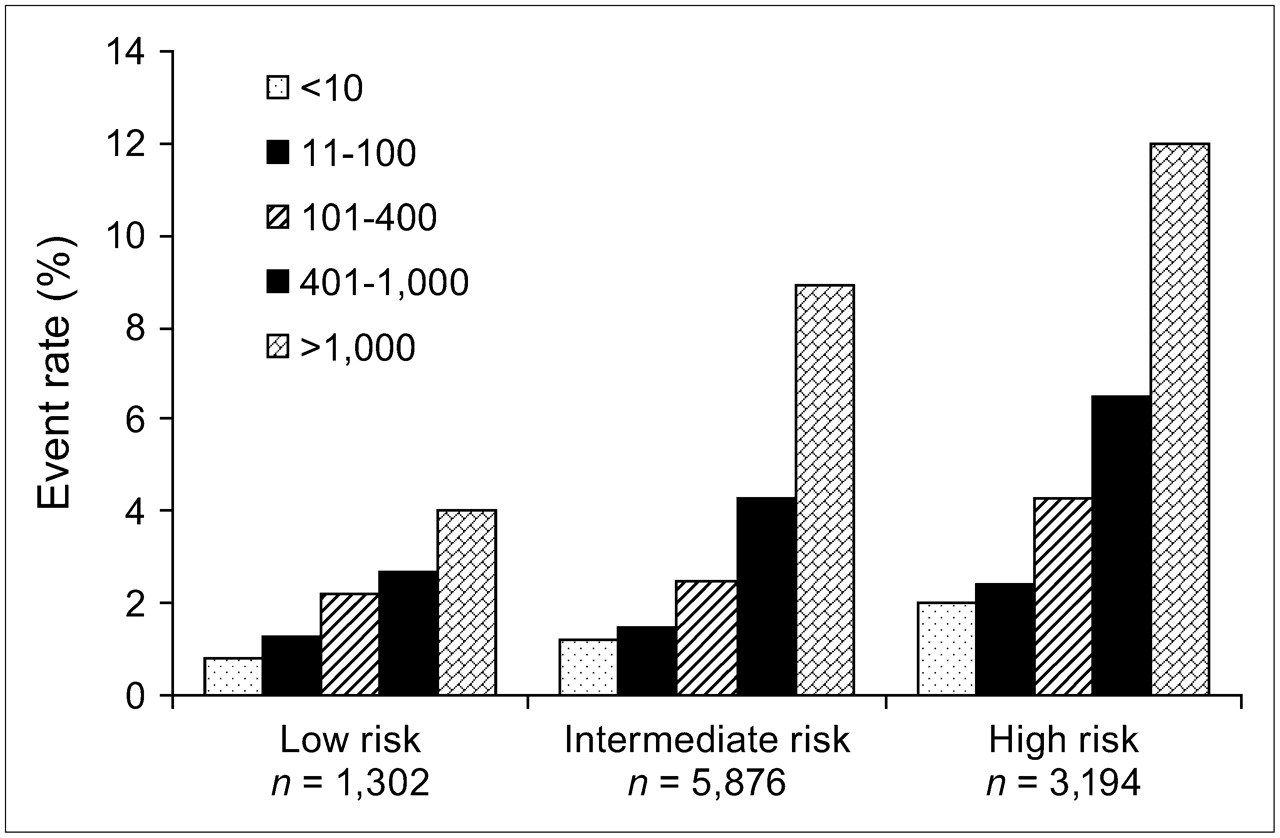
As with MPS, measuring CCS has potentially wide prognostic applications. However, in contrast to MPS, which provides useful information across the spectrum of patients with known as well as suspected CAD, it is not likely that assessment of CCS will provide incremental prognostic discrimination in patients with known CAD. In such patients, prognosis is governed more by functional parameters, such as ischemia and left ventricular (LV) function, than by measurements of atherosclerotic disease burden. Rather, the principal prognostic value of CCS is likely to reside in asymptomatic patients with a low-to-intermediate likelihood of CAD (e.g., range, 15%–50%) based on age, sex, and risk factors, which is basically another way of expressing a group with intermediate long-term risk by the Framingham risk score (FRS) (23). A large number of studies have demonstrated that CCS provides incremental prognostic information over conventional risk factors in assessing the risk of hard cardiac events. For example, a publication of results in >10,000 asymptomatic patients followed over 5 y for all-cause mortality demonstrated that, in both men and women, the previously described categories for degrees of CCS abnormality were strongly predictive of all-cause mortality and that CCS provided significant incremental information over that provided by conventional risk factor analysis alone (Fig. 2) (24). Several other studies have supported these findings (23,25–27), including 2 recent prospective, population-based trials (28,29) that have demonstrated the incremental prognostic value of CCS over the traditional Framingham risk assessment. The St. Francis Heart Study (28) determined the relationship of CCS by electron beam tomography (EBT) to standard coronary disease risk factors and C-reactive protein in the prediction of atherosclerotic cardiovascular disease events in 4,613 asymptomatic persons (age, 50–70 y) who underwent EBT of the coronary arteries and were monitored at a mean of 4.3 y. One hundred nineteen had sustained at least 1 atherosclerotic cardiovascular disease event. For a CCS threshold > 100 versus < 100, relative risk (95% confidence interval) was 9.6 (6.7−13.9) for all atherosclerotic cardiovascular disease events, 11.1 (7.3−16.7) for all coronary events, and 3 and 9.2 (4.9−17.3) for nonfatal myocardial infarction (MI) and death. The CCS predicted coronary disease events independently of standard risk factors and C-reactive protein (P = 0.004), was superior to the Framingham risk score in the prediction of events (area under the receiver-operating-characteristic curve of 0.79 ± 0.03 vs. 0.69 ± 0.03; P = 0.0006), and enhanced stratification of those falling into the Framingham categories of low, intermediate, and high risk (P < 0.0001) (28).

Risk stratification for each category of Framingham risk (from low to high) according to calcium score (P < 0.001 across risk groups). Event rate is predicted mortality at 5 y. (Adapted with permission from (24).)
In a second prospective study, Taylor et al. reported a prognostic population-based study of a younger population (29). Of a cohort of 2,000 nonreferred, asymptomatic, healthy men and women 40−50 y old, incident MI, acute coronary syndromes, and sudden cardiac death were ascertained via annual telephonic contacts, with follow-up (mean, 3.0 ± 1.4 y; range, 1−6 y) in 99.2% of the cohort. Nine acute events occurred in men at a mean age of 46 y, including 7 of 364 men with coronary artery calcium (CAC) (1.95%) and 2 of 1,263 men without CAC (0.16%; P < 0.0001 by log rank). No events occurred in women. In young men, the presence of any CAC was associated with an 11.8-fold increased risk for incident coronary heart disease (P = 0.002) in a Cox model controlling for the FRS. Among those with CAC present, the risk of coronary events increased incrementally across tertiles of CAC severity (hazard ratio, 4.3 per tertile). In this study of relatively young individuals, the authors concluded that the presence of coronary artery calcification provides substantial, cost-effective, independent prognostic value in predicting incident coronary heart disease that is incremental to measured coronary risk factors (29).
The evidence is now strong that CCS is valuable for purposes of risk assessment of asymptomatic patients with intermediate clinical risk. There is now widespread support that third-party carriers should pay for testing in this patient group rather than having it be a test only for patients who can afford to pay for it.
Although several reports have shown that approximately 95% of patients suffering a first MI have an abnormal CCS within days of the MI, implying that it is unusual for coronary atherosclerosis to result in acute MI before the development of any coronary calcification (30–33), approximately 5% of patients with documented acute infarction have no CAC. Thus, the CCS may be limited in ruling out disease in symptomatic patients. The increasing experience with coronary CT angiography (CTA) suggests that the latter, rather than the CCS, will become the most commonly used CT method of choice to triage these patients. The images illustrated in Figures 3 and 4 illustrate this potential drawback of relying of the CCS to rule out an acute coronary syndrome.
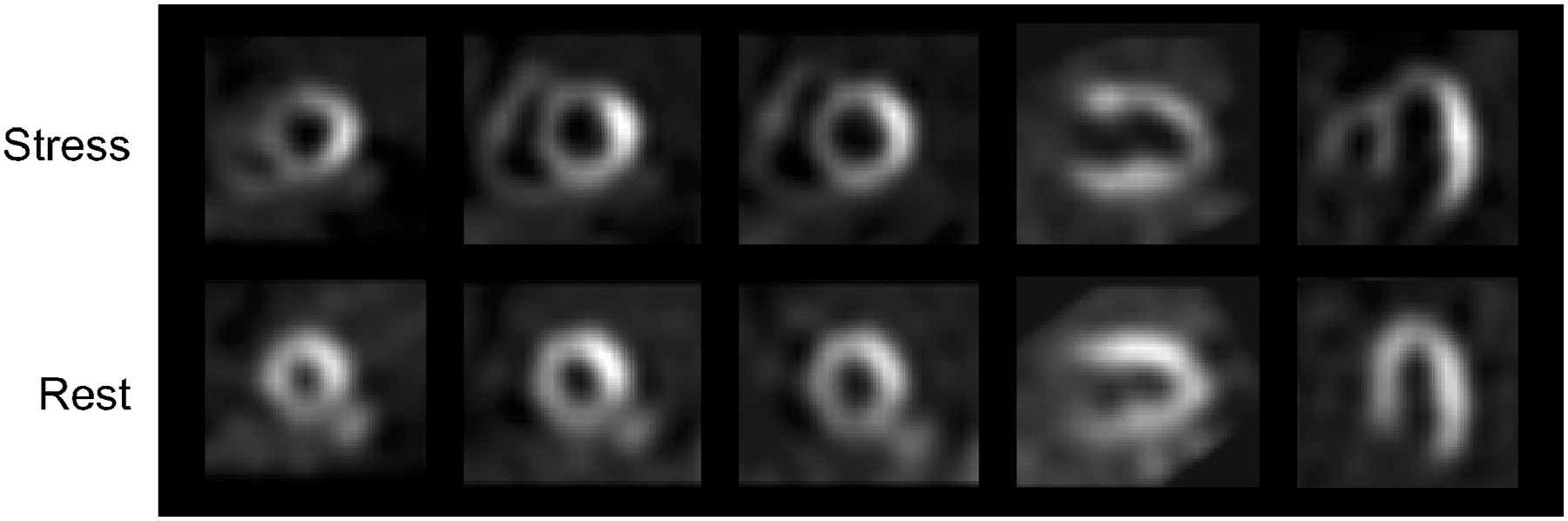
Exercise stress sestamibi/rest 201Tl MPS images in 64-y-old man with recent onset of angina suggesting unstable CAD. Clinical and ECG responses to stress were ischemic. Large reversible defects are seen in anterior, septal, inferior, and apical walls consistent with critical left anterior descending coronary artery stenosis.

EBT for CCS performed as part of research study after MPS of patient in Figure 3 showed minimal calcification in left anterior descending coronary artery (LAD)—an almost imperceptible small calcified area was seen (CCS, 7.5). Subsequent coronary angiography revealed 80% stenosis in proximal LAD and subtotal occlusion of first diagonal branch. This example illustrates how an acute coronary syndrome might be misclassified by noncontrast CT alone.
GUIDING PATIENT MANAGEMENT DECISIONS BY CCS
One of the important applications of noninvasive testing is in determining the appropriate therapy in an individual patient. In asymptomatic patients with coronary risk factors, the CCS may be of particular use. For example, in patients with borderline cholesterol elevations or borderline hypertension, the CCS can help the primary care physician decide whether to treat aggressively to prevent the development of clinical atherosclerotic disease. On the basis of available data, the CCS may be used to determine the appropriateness and aggressiveness of medical therapies, such as statin use, or the need for stress testing, among patients presenting with an intermediate 10-y risk of MI or cardiac death by the FRS.
One group of patients affected in this manner includes those with the metabolic syndrome—characterized by varying combinations of abdominal obesity, insulin resistance, lipid abnormalities, and hypertension—many of whom are at intermediate risk. Approximately one fourth of these patients have a CCS ≥ the 75th percentile, which has been designated by the National Cholesterol Educational Program as a criterion to stratify the patient into more intensive risk factor management. Nearly half of such patients have either a high FRS or fit the high CCS or both criteria that would justify intensive secondary-prevention medical therapy (i.e., considering them to have a coronary heart disease risk equivalent justifying treatment of low-density lipoprotein (LDL) cholesterol to <70 mg/dL and blood pressure to 120/80) (34). The use of the CCS to guide management is one of the most common reasons that the test is currently ordered by physicians.
Part of guiding management decisions is the manner in which a test result affects the choice of subsequent testing. From the foregoing discussion, it would seem clear that asymptomatic patients with extensive coronary atherosclerosis by CCS would benefit from additional testing for ischemia. This concept fits with recommendations made years ago by Rumberger et al. (35). For purposes of cost-effectiveness, it would not be appropriate for all patients with atherosclerosis by EBT or CT to be referred for further testing.
Several published reports have been helpful in determining the CCS threshold above which asymptomatic patients merit referring for stress imaging. He et al. (36) evaluated the frequency of stress-induced ischemia by MPS in patients who had undergone EBT scanning. These investigators evaluated 370 patients undergoing both MPS and EBT for coronary calcification. They divided their patients into the traditional categories of no (CCS, 0), minimal (CCS, 1−10), mild (CCS, 11−100), moderate (CCS, 101−399), and extensive coronary calcium (CCS, >400) (35). Only 1 of >100 patients with CCS ≤ 100 had abnormal MPS. Twelve percent of patients with moderate CCS had abnormal MPS and 47% of patients with extensive CCS had abnormal MPS. Moser et al. (37) recently reported results of combined SPECT and CCS testing in 102 patients, with these investigators using multislice CT (MSCT) for CCS. In this smaller group, none of 19 patients with a CCS < 100, 6 of 51 patients (12%) with a CCS of 100−400, and 13 of 32 patients (41%) with a CCS ≥ 400 had an abnormal SPECT study. They concluded that a CCS threshold of >400 was useful in determining the need for subsequent MPS.
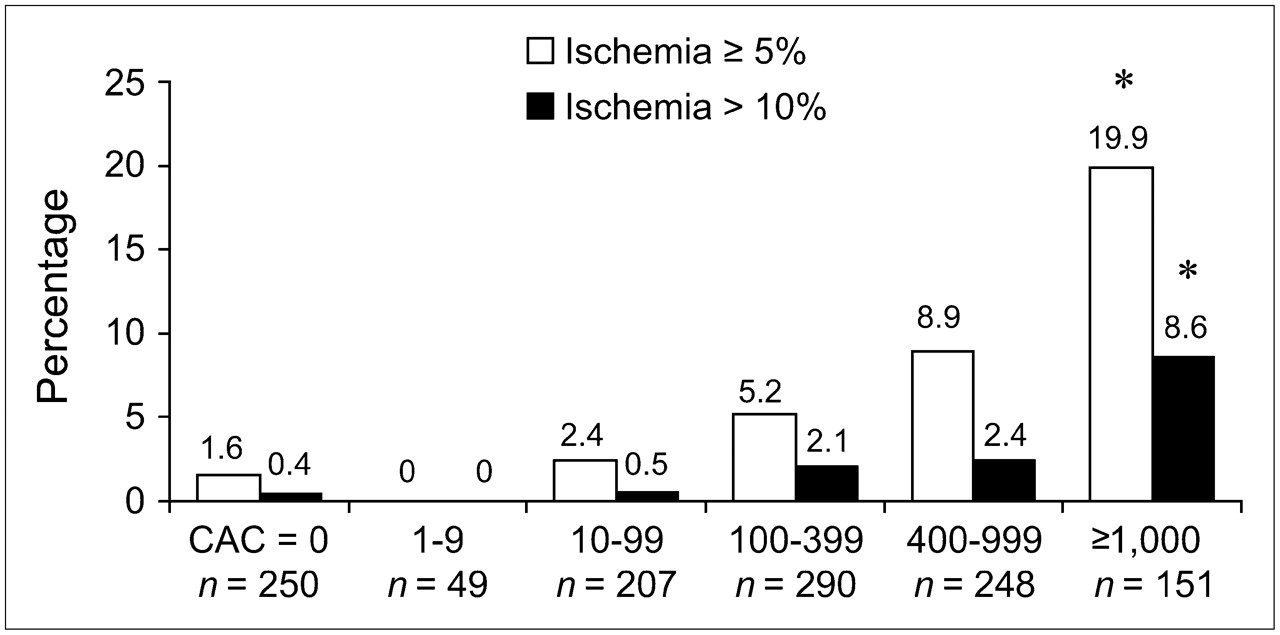
Data from Cedars-Sinai Medical Center have confirmed the findings of previous studies with respect to the patients with CCS ≥ 400 (38). In 1,195 consecutive patients with no history of CAD who had EBT and MPS, among the patients with a CCS < 100, MPS ischemia was rare, occurring in <2% of such patients (38). This low frequency of ischemia with a CCS < 100 was present in patients with and without clinical symptoms, although a trend toward more ischemia in symptomatic patients with scores 10−99 was observed. As the CCS increased in magnitude above 100, the frequency of myocardial ischemia on MPS increased progressively (Fig. 5). Among patients with CCS exceeding 1,000, 20% manifested an ischemia by MPS. Our results further indicate that the likelihood of myocardial ischemia by MPS is more tightly related to the absolute CCS than to the age–sex-stratified CCS percentile. These 3 studies were concordant in finding that the CCS threshold > 400 generally appeared appropriate for guiding the decision to refer for stress MPS. Another aspect of our study was of particular importance in documenting the insensitivity of MPS for detecting coronary atherosclerosis (in contrast to detecting patients with hemodynamically significant CAD). Of 1,119 patients with normal MPS, a large proportion had a high enough CCS that there would be consensus that aggressive medical management is warranted: 56% had CCS > 100 and 31% had CCS > 400 (Fig. 6). These findings suggest that if testing begins with MPS in a given patient, further assessment of atherosclerotic burden by CAC testing may be useful in assessment of the need for aggressive attempts to prevent coronary events.
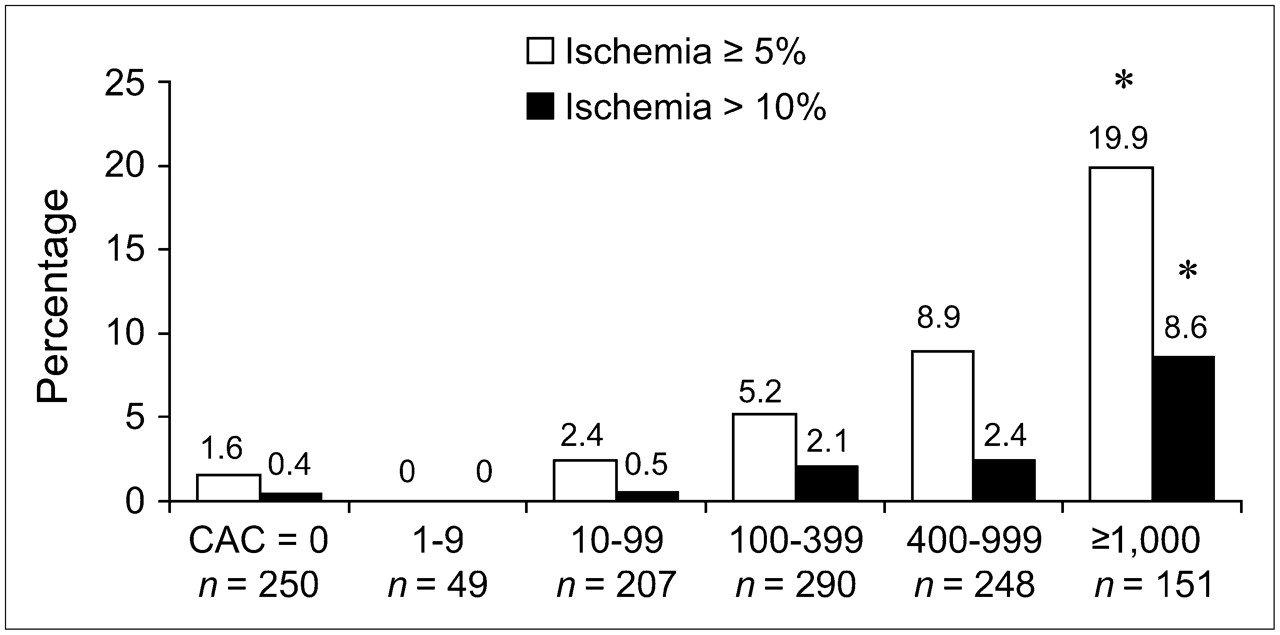
Frequency of ischemic MPS (≥5% ischemic) and of moderate-to-severe ischemia (>10% ischemic) for patients divided into 6 CCS groupings. *P < 0.0001 for trend. (Adapted with permission from (38).)

Distribution of CCS for 1,119 patients manifesting normal MPS (left) and 76 patients with ischemic MPS (right). (Adapted with permission from (38).)
In a more recent study, we further examined the relationships between CCS and MPS according to the presence of the metabolic syndrome (39). In patients with the metabolic syndrome and a CCS of 100−400, the frequency of abnormal MPS was as high as that in patients with no metabolic abnormality with CCS ≥ 400 (15.0% vs. 14.8%, respectively). Thus, in this group of patients a lower threshold for determining the need for assessment of stress ischemia may be indicated—that is, additional testing with MPS might be appropriate in patients with the metabolic syndrome and CCS ≥ 100. Similarly, Anand et al. (40) reported that there was an intermediate to high frequency of abnormal MPS studies in diabetic patients with CCS ≥ 100.
The data from these studies suggest an important distinction between short-term and long-term risk. Although a low CCS with a high percentile ranking in young patients may be indicative of long-term risk for developing cardiac events (41–43), this same score is probably not predictive of short-term risk, given the finding that such patients rarely have evidence of ischemia on MPS. Thus, further testing by MPS of patients found to have a high CCS percentile but a CCS < 100 would not appear to be needed in most patients. In contrast, MPS appears excellent for determining short-term risk but, because of the insensitivity of the method for detecting subclinical atherosclerosis, may not be as effective as atherosclerosis imaging in determining long-term risk.
On the basis of the available data, 3 summary statements might be made with regard to combined MPS and CCS testing: (i) It appears that the referral of patients for MPS is generally not needed when the CCS is <100 because of the very low likelihood of observing inducible myocardial ischemia in such patients. Conversely, when the CCS is ≥400, stress imaging would appear to be generally beneficial, because the frequency of inducible ischemia is substantial, even in asymptomatic patients. (ii) CCS of 100−400 constitutes a “gray zone” relative to the issue of who may require stress test referral after CAC imaging. For CCS in this range, clinical factors—such as sex, concomitant chest pain, diabetes, the metabolic syndrome, or other specific combinations of coronary risk factors—are likely to determine whether ischemia testing is needed, but prospective study is needed in this regard. (iii) The wide range of CCS in patients with normal MPS studies exposes an important limitation relevant to all forms of stress testing: they do not effectively screen for subclinical atherosclerosis (38). However, there are no available data yet to compare the relative short-term and long-term risks for cardiac events among patients with various combinations of MPS results and CCS, such as those presenting with the combination of very high CCS but normal MPS. It is reasonable to hypothesize that such patients might be at low short-term risk but at high long-term risk for cardiac events, as supported by a preliminary analysis (44). If borne out by further study, the CCS could then be unmasking a subgroup of patients who would receive more aggressive antiatherosclerotic intervention than would have been indicated on the basis of the results of MPS testing alone. Accordingly, future study that incorporates the prognostic follow-up data from patients undergoing both studies would be of interest to determine which patients with normal stress imaging tests are best suited for undergoing subsequent CAC scanning.
PROGNOSTIC APPLICATIONS OF CTA
To date, most published reports dealing with coronary CTA using MSCT have described the diagnostic accuracy of this test. As discussed extensively in our earlier review (45), many published articles have reported high sensitivity and specificity of 16-slice MSCT for detection of CAD (46), and studies are beginning to be reported with the 64-slice scanners (47). One of the key advantages of coronary CTA over nuclear testing is that the results are very unlikely to be normal in patients in whom revascularization would be warranted, in contrast to MPS, in which balanced reduction in flow can occasionally result in a normal study despite the presence of severe and extensive CAD.
Whether CCS should also be measured in patients undergoing coronary CTA is a matter of controversy because of the added radiation burden—approximately 25% as much as that of coronary CTA. Although the CCS cannot be measured accurately during the contrast infusion acquisition of the CTA itself, many investigators consider the ability to assess the presence and extent of coronary calcium adequate to provide sufficient information with regard to early atherosclerosis to guide management decisions without the additional radiation exposure. This visual estimate of the coronary calcium is routinely reported with coronary CTA. The current clinical applications of coronary CTA are listed in Table 1.
Clinical Applications of CTA
Although the diagnostic use of CTA in symptomatic patients with a low-to-intermediate likelihood of CAD is now commonly accepted and in the view of many already established, there are no data yet with regard to the use of CTA for risk stratification of patients with known or suspected CAD. There has not yet been adequate time for the collection of the prognostic data needed to fully investigate this potential of CTA with MSCT.
Nonetheless, since the extent and severity of coronary obstructive lesions on selective coronary angiography have been known to be a potent predictor of outcome and to identify subgroups of patients likely to benefit from revascularization (6), it is likely that coronary CTA will also have strong prognostic power. In some patients, sufficiently high risk may be defined by the location of severity of CT-defined coronary stenosis, leading directly to selective coronary angiography after the CT procedure. However, the ability of selective coronary angiography to predict benefit from revascularization in randomized trials was dependent on the extent and severity of inducible ischemia (48,49). Furthermore, in these previous trials, inducible ischemia was evaluated only by traditional ECG stress testing (6,48). We consider it likely that, in a large proportion of patients found to have coronary lesions by CTA, further assessment of the extent and severity of ischemia by SPECT or PET will prove useful in effective identification of patients who are likely to derive a survival benefit from coronary revascularization.
SCREENING FOR CORONARY ATHEROSCLEROSIS: APPROACH TO USE OF CT FOR CCS, CTA, AND MPS IN ASYMPTOMATIC PATIENTS
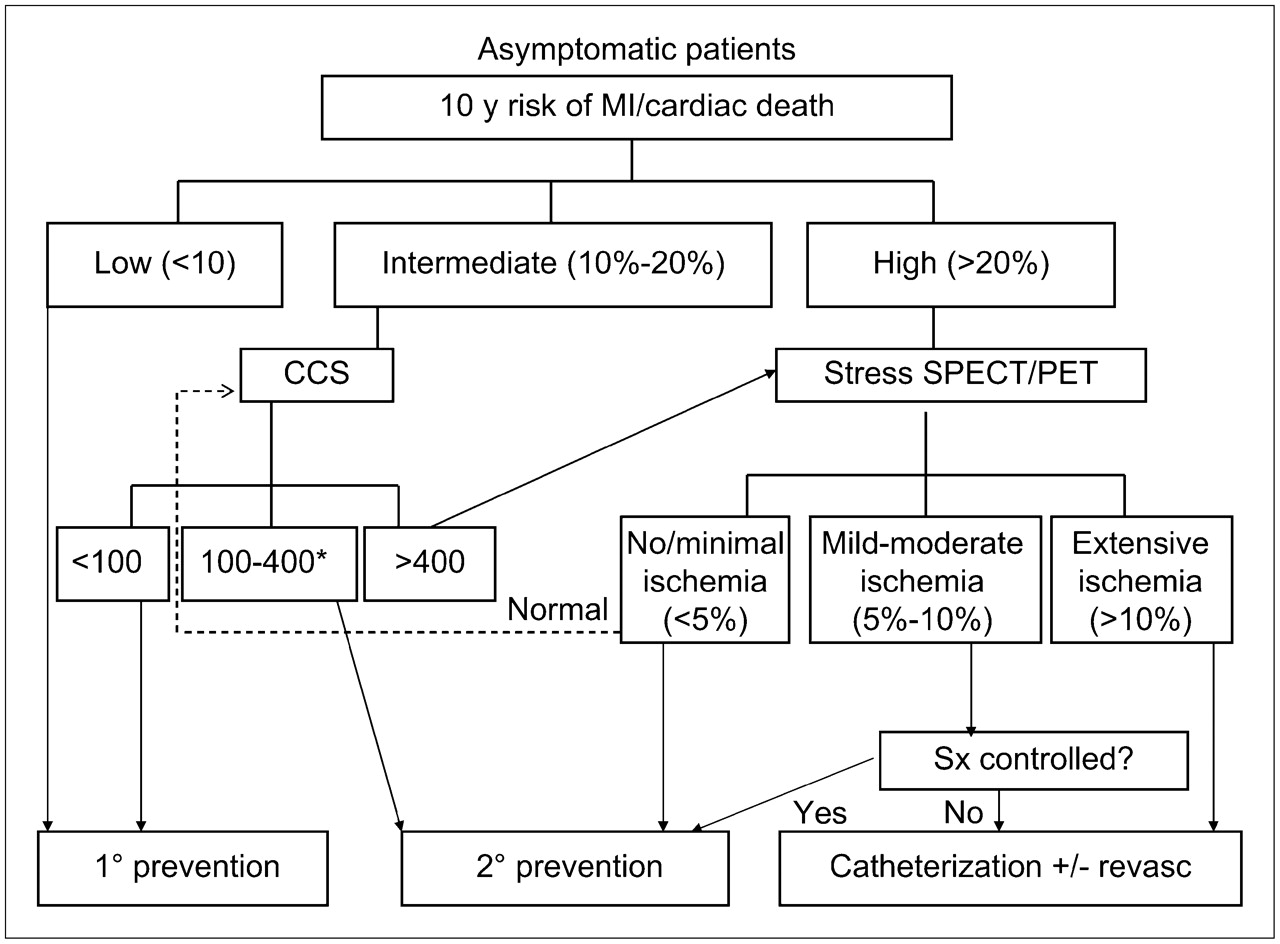
Figure 7 illustrates our conceptual approach to the use of atherosclerosis imaging, coronary CTA, and nuclear testing in CAD diagnosis and risk stratification with respect to screening of asymptomatic patients. Although screening for CAD with imaging is not yet widely reimbursed, the approach is gaining in acceptance. In the asymptomatic patient, the initial assessment involves estimation of the 10-y risk of developing MI or cardiac death, on the basis of measures such as the FRS, as recommended by standard Adult Treatment Program (ATP) III guidelines with the addition of family history of early CAD and assessment of the metabolic syndrome. Then, patients are assigned to groups corresponding to the <10%, 10%−20%, and >20% 10-y risk of MI or cardiac death categories recently advocated as low, intermediate, and high risk (50). Patients with a very low risk would need only counseling with regard to diet and exercise. Patients with a high 10-y risk (>20%) are considered to have a CAD risk equivalent meriting treatment using secondary prevention guidelines. In these patients, atherosclerosis testing is not generally recommended, although it might be appropriate to determine the need for ischemia testing. In this regard, data from the Detection of Ischemia in Asymptomatic Diabetics (DIAD) study (51), in conjunction with data from Anand et al. with regard to the relationship between CCS and ischemia in diabetics (40), have suggested that CCS might be routinely performed in asymptomatic diabetic adults. Given the high frequency of silent ischemia in diabetics, atherosclerosis imaging may be useful to identify those with advanced coronary atherosclerosis in whom stress MPS would be appropriate. The remaining large group of patients with an intermediate 10-y risk (10%−20%) are excellent candidates for atherosclerosis screening using the CCS.

Approach to use of coronary calcium scanning and nuclear testing in screening for CAD in asymptomatic patients. CCS = CCS by EBT or multislice spiral CT; Sx = symptoms; revasc = revascularization. *Consider SPECT/PET in higher-risk subsets.
Patients would then have the intensiveness of their medical therapy guided by the degree of CCS. As shown in Figure 7, scores < 100 are generally considered low enough that aggressive medical therapy may not be needed. Scores > 100 are generally accepted as the cutoff for recommending aggressive medical therapy with target LDL < 70 and the target blood pressure would be 120/80 (50). Patients with scores ≥ 10 but < 100 might be considered as appropriate for aggressive medical therapy when CCS is at or above the 90th percentile for age and sex (38), although the exact thresholds remain controversial. With regard to further testing, patients with CCS > 400 would be candidates for further testing with MPS for purposes of risk–benefit assessment with respect to the possible need to consider revascularization. The specific cutoff points for CCS shown in Figure 7 are somewhat arbitrary. In this regard, an increasing proportion of cardiologists interested in primary prevention are treating aggressively at cutoffs lower than 100. The exact cutoff above which patients should be referred for stress imaging is also unclear; however, as noted earlier, in asymptomatic patients, the threshold of 400 for this referral may be appropriate. In the CCS = 100−400 category it would not be cost-effective to refer all patients for myocardial perfusion scanning; however, if one is tailoring this referral to the individual patient, on the basis of age, sex, and risk factors, selective referral for stress imaging might be appropriate. In this regard, recent studies have suggested that the CCS = 100−400 category would deserve testing if the patient is diabetic (40) or has the metabolic syndrome (39).
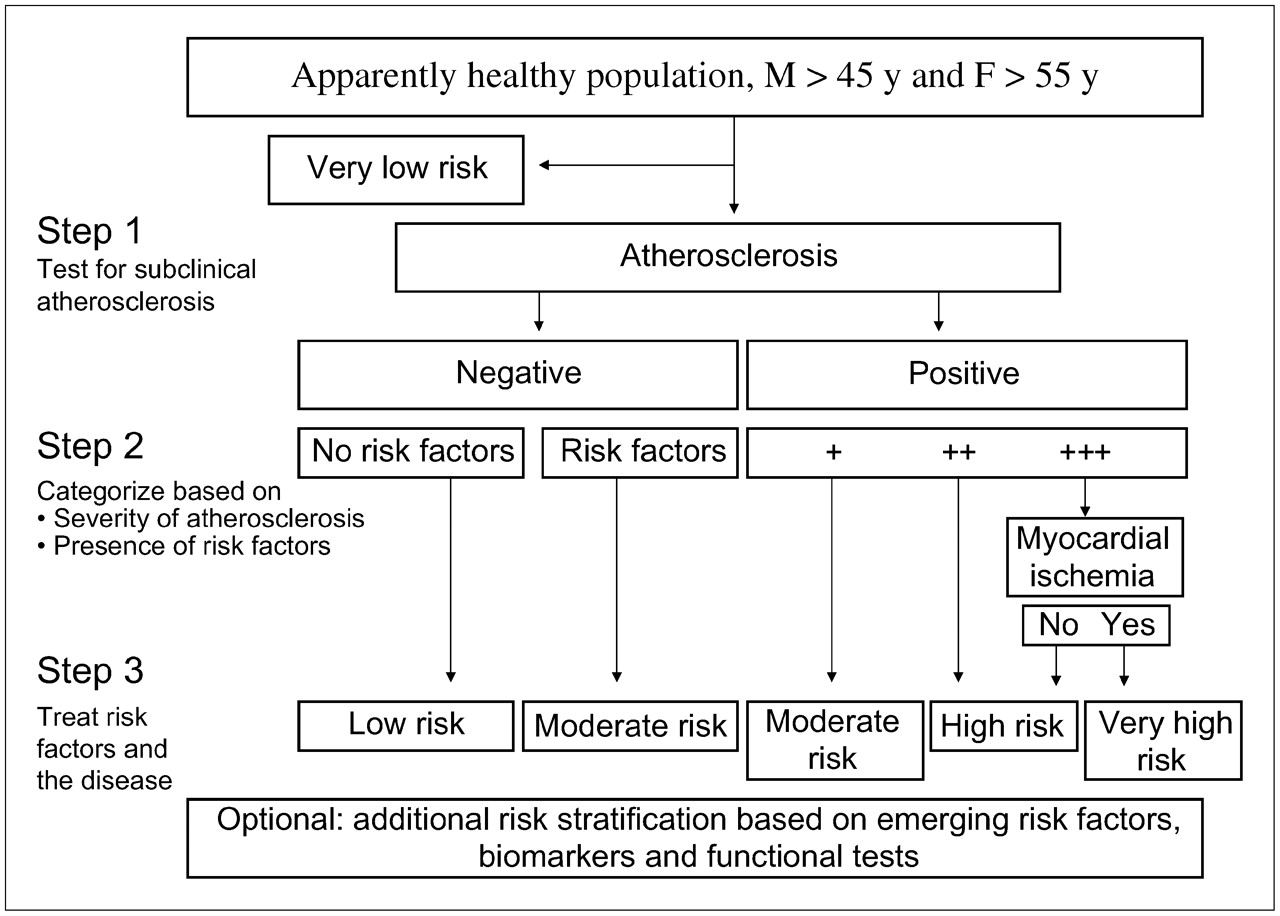
A modification of this approach has recently been adopted by the Association for the Eradication of Heart Attacks as shown in Figure 8. In an attempt to eradicate heart attacks rather than to simply reduce their frequency, this group recommends screening of all men of age >45 y and women of age >55 y, as a substantial proportion of heart attacks occurs in patients with a low Framingham risk. After atherosclerosis imaging, the intensity of therapy and the need for ischemia testing is governed by the postatherosclerosis imaging assessment of risk. In general, the use of coronary CTA or MPS would not be recommended for initial testing, as reflected for the latter in recent guidelines (4). However, in some high-risk asymptomatic individuals, particularly those with high-risk occupations, MPS or coronary CTA might be appropriate.

Approach to screening for atherosclerosis advocated by the Association for the Eradication of Heart Attacks (AHEA).
DETECTION AND MANAGEMENT OF CAD: APPROACH TO USE OF CT FOR CCS, CTA, AND MPS IN SYMPTOMATIC PATIENTS
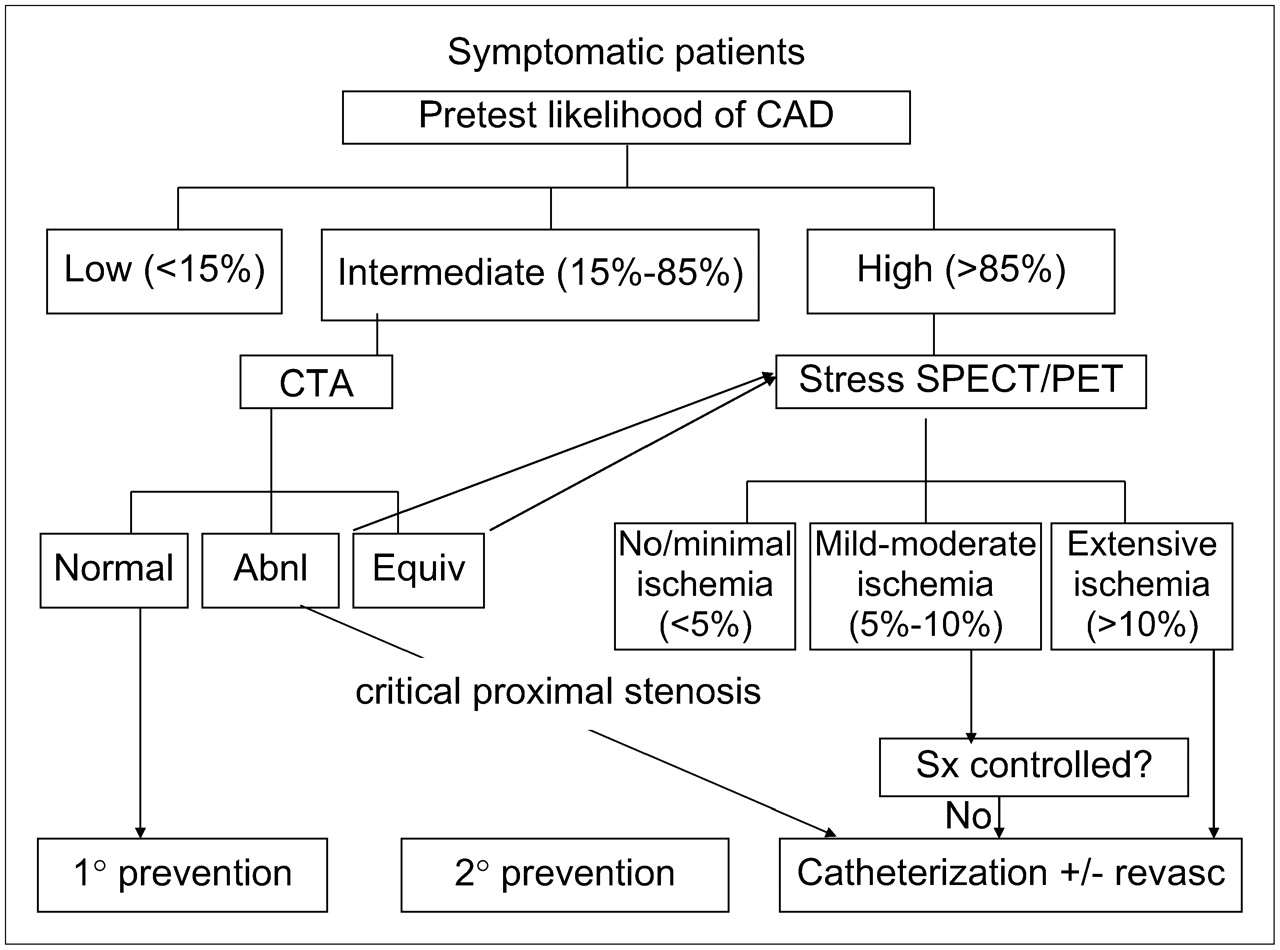
Figure 9 illustrates our approach to patients with symptoms of possible ischemic origin in the setting where 16-slice or greater coronary CTA is available. In symptomatic patients, the pretest likelihood of angiographically significant CAD, using age, sex, risk factors, and symptoms, as initially suggested by Diamond et al. (52,53), becomes the starting point for the clinician—rather than the 10-y risk used for screening. As noted earlier (45), although various pretest likelihood cutoff points have been recommended, we have adopted the cutoff points 15% and 85% on the basis of our prognostic observations (54), resulting in 3 likelihood groups: low (<15%), intermediate (15%−85%), and high (>85%). In general, patients with chest pain symptoms or shortness of breath have at least a 15% likelihood of CAD. Because the value of diagnostic testing is greatest in patients with an intermediate likelihood of disease, these patients become excellent candidates for coronary CTA—the test with the highest accuracy, combining sensitivity and specificity. In general, patients in this group have an intermediate risk of developing a clinical cardiovascular event over 10 y (10%−20%) (50), described for the asymptomatic patient. Although existing guidelines recommend exercise testing without imaging for these patients (55), because coronary CTA provides a far more sensitive test for CAD in this population, we consider it more useful than the exercise ECG in selecting patients for aggressive medical management and for additional testing. After coronary CTA, further testing and therapy would be guided by the posttest likelihood of CAD and the extent and severity of the observed disease. If coronary CTA (including the estimated or measured CCS) is normal, primary prevention would be appropriate. It is likely that the definitive ability to rule out CAD will become a principal driving force in the application of coronary CTA. If critical proximal stenoses are observed (e.g., >90%), direct referral to selective coronary angiography would appear to be recommended. If the results of coronary CTA are equivocal for a proximal coronary stenosis or if CTA is clearly abnormal but the anatomy is not “compelling” with regard to the need for revascularization, referral for ischemia testing with MPS would appear appropriate to determine the need to consider coronary revascularization. In older men and very elderly women with an intermediate likelihood of CAD, the frequency of a CCS > 400 is quite high. In these patients, it may be more appropriate to begin with the CCS and MPS, because in the presence of dense CAC, coronary CTA is nondiagnostic for the presence of CAD (56).
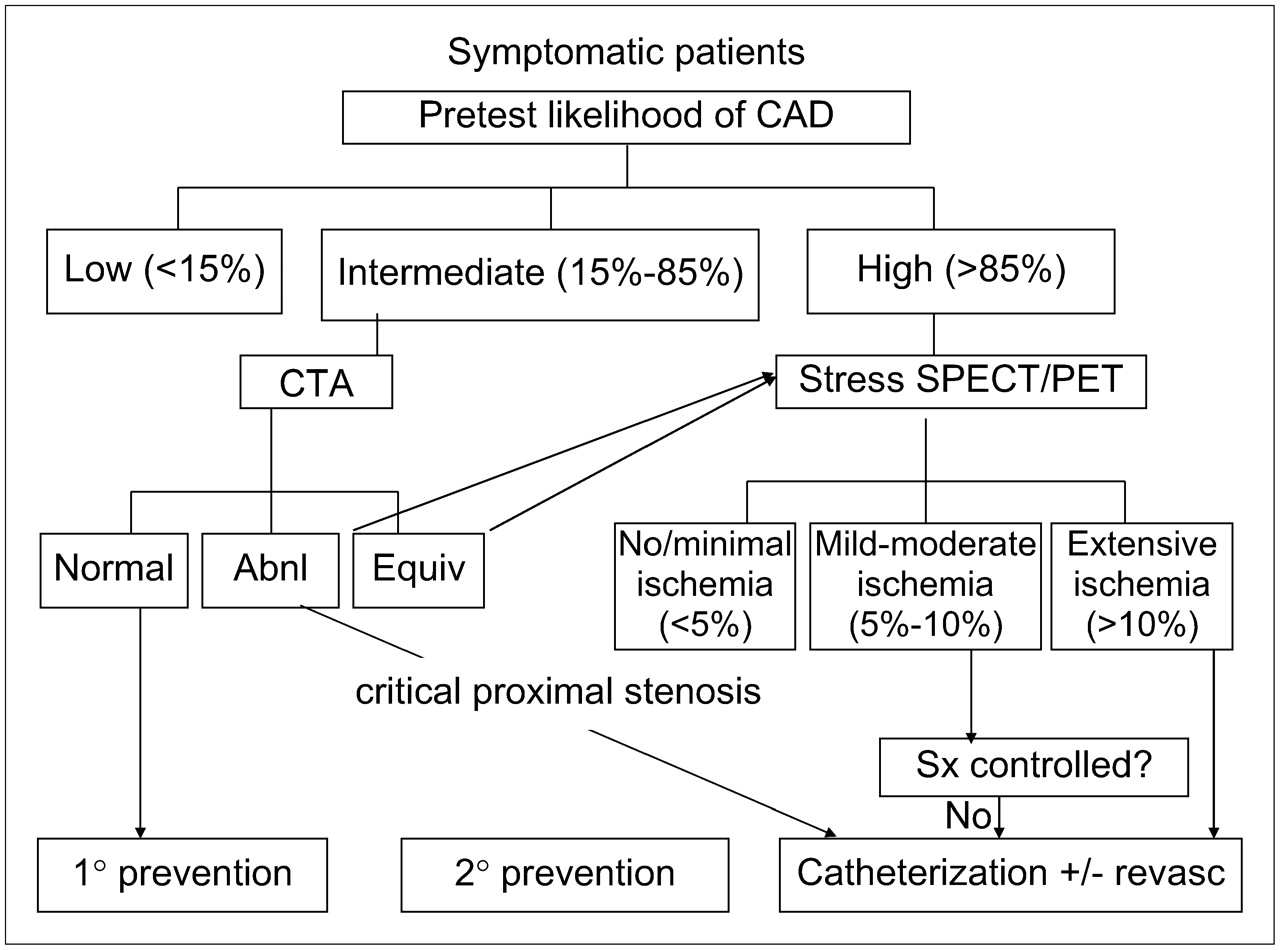
Approach to diagnosis and management of CAD in symptomatic patients using coronary CTA and stress SPECT or PET. Abnl = abnormal; Equiv = equivocal; Sx = symptoms; revasc = revascularization.
Patients deemed to have a high (>85%) likelihood of CAD or those with known CAD are often directly catheterized, particularly if they have symptoms that persist after maximal medical therapy. In those without limiting symptoms, it may be most effective to start with MPS for purposes of determining the need for consideration of revascularization. Because these patients in general have a >20% 10-y risk of CAD, they would usually already be suited for secondary prevention treatment. The likelihood of disease is sufficiently high that it is generally assumed that their symptoms are from the disease. We have recently reported data supporting the effectiveness and cost-effectiveness of this approach (57). Similar findings have also been reported by the Mayo Clinic group (58), who showed that, even in patients with a normal resting ECG, if the clinical risk of CAD is high, a low-risk treadmill test alone is insufficient to predict a low risk of cardiac events. If the resting ECG is abnormal or otherwise uninterpretable (e.g., digoxin or left bundle branch block) or the patient cannot exercise adequately, there is a concordance of opinion that direct referral to a stress imaging procedure is appropriate (4,55).
If stress imaging is performed, patients with extensive ischemia by nuclear testing (or those who are, for other reasons, considered to be at high risk by clinical assessment after stress imaging) would be candidates for coronary angiography. Patients with ischemia of lesser magnitude might be candidates for angiography, depending on the clinical presentation. In this regard, we have described several clinical and nonperfusion MPS indicators of risk that should be considered in making the decision with regard to the need for coronary angiography (Table 2). Patients considered to be at high risk despite having only 5%−10% ischemia include those with low LV ejection fraction (9), transient ischemic dilation (10), lung uptake (59), diabetes (11,60), or atrial fibrillation (61). In patients with equivocal MPS results or those with marked discordance between the clinical or ECG responses to stress and the MPS results, coronary CTA after MPS might be useful.
Clinical (Nonnuclear) and Nuclear Factors Useful in Guiding the Decision to Proceed with Selective Coronary Angiography After Stress MPS
Figure 10 illustrates our approach to the symptomatic patient in settings where coronary CTA is not available. Although not yet shown to be cost-effective in the lower range of intermediate likelihood of CAD (15%−50%), most investigators would agree that MPS would appear to be the initial test of choice in patients with a high intermediate likelihood (≥50%−85%) or high likelihood of CAD. In those within the lower intermediate range, it may be sufficient to perform atherosclerosis imaging as the initial step (Fig. 10). In those sent directly to MPS, the management after MPS would be as described earlier. However, an important distinction is worthy of mention. In selected patients with normal or nearly normal nuclear scans, CCS might be appropriate after MPS to evaluate the extent of atherosclerosis and help guide medical management decisions (62) and to avoid missing extensive atherosclerosis simply because there is no stress-induced ischemia. Although atherosclerosis imaging may not be needed in patients who are already following an aggressive medical management approach using secondary prevention guidelines, CCS in this setting may help motivate patients to follow medical approaches to the control of CAD as well as help guide the intensity of medical management in settings in which the need for secondary prevention is not clear (45). We have also found that CCS after MPS is very effective in defining further management in patients with equivocal MPS results, occasionally helping recognize patients in whom the MPS severely underestimates the ischemic burden.
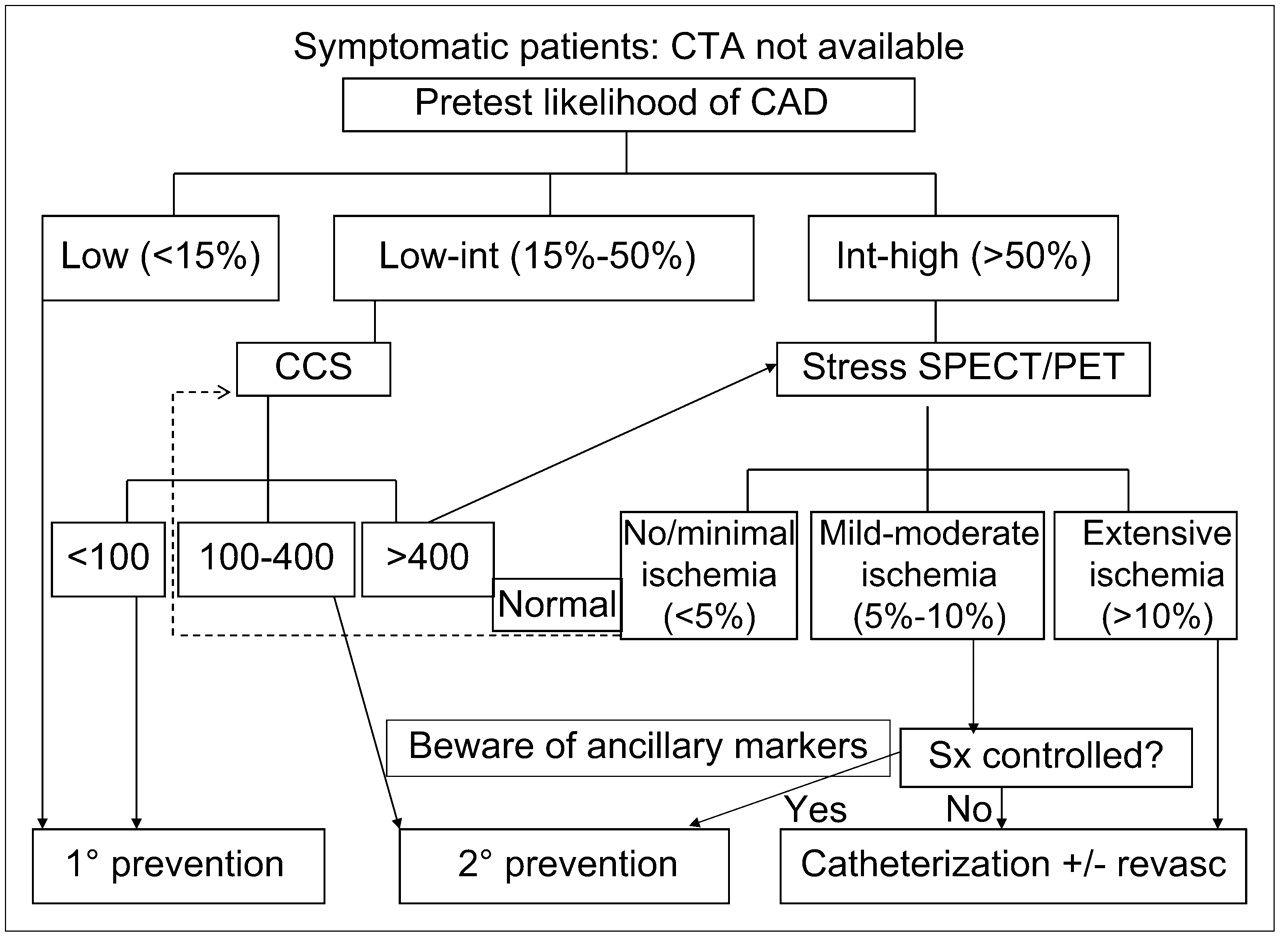
Approach to diagnosis and management of CAD in symptomatic patients using CCS, stress SPECT, or PET, in situations in which coronary CTA is unavailable. This approach is the same as that used for screening, except that the starting point becomes the likelihood of CAD rather than the 10-y risk of events. Low-int = low to intermediate; Int-high = intermediate to high; Sx = symptoms; revasc = revascularization.
Rest–stress cardiovascular MRI may emerge as being similar to MPS for assessment of the extent and severity of ischemia; to date, however, there are only minimal prognostic data with regard to this application, as large numbers of patients studied in this manner have not yet been monitored.
EVALUATING RESPONSE TO TREATMENT
Another application for which noninvasive testing is frequently used is assessing the response to therapy.
CCS
Serial CCS measurement may be of use to track the progression of disease, although the data in this regard are less well documented than in guiding the intensity of medical management (63–65). Work by Callister et al. (63) and others (42,64) suggests that serial assessment of the calcified coronary volume score as determined by EBT can be effective in documenting that therapy has slowed the accumulation of CAC in individual patients, although there have been several reports noting no treatment benefit (66,67). In a randomized clinical trial, a part of the St. Francis Heart Study showed a trend to less progression of the CCS in patients treated with statins versus a control group but failed to reach statistical significance (68).
Studies are beginning to appear reporting the prognostic significance of changes in CCS over time. In a series of 817 asymptomatic intermediate-risk patients undergoing serial CCS measurement, those having an acute MI after the second scan had an average rate of progression of 47% ± 50%, a rate of increase that was nearly double that of event-free survivors (26% ± 32% per year; P < 0.001) (43). In a related report from these investigators examining the patients who also had serial lipid assessments, 495 asymptomatic individuals underwent serial EBT scanning and were followed for 3 y for the occurrence of the first acute MI (69). LDL control (mean, 119 mg/dL) was similar for those patients having an event as for those nonevent individuals. However, CCS progression was 42% ± 23% per year for those patients who were hospitalized for an acute MI compared with 17% ± 25% per year for those event-free survivors (P < 0.001). Thus, early data suggest that a change in CCS over time may be an important determinant of outcome and perhaps of greater prognostic value than the degree of LDL control.
MPS
In patients with chronic CAD, nuclear cardiology techniques have been demonstrated to be effective in monitoring the effects of medical or invasive therapies over time (70,71). Though we believe that reassessment of a patient after initiation of therapy will provide early evidence with regard to alteration of patient risk, this application has achieved only class IIb status (i.e., usefulness/efficacy less well established) in the current guidelines (4). Of interest, there are data with both MPS and PET suggesting that these methods may start to show abnormal findings at a stage when atherosclerosis is nonobstructive, depending on the activity of the disease (71–73). Serial MPS data are being studied in large randomized trials that may clarify the use of this approach to evaluate therapy in chronic CAD, notably a substudy within the COURAGE (Clinical Outcomes Using Revascularization and Aggressive druG Evaluation) trial and the BARI 2D (Bypass Angioplasty Revascularization Investigation 2 Diabetes) trial.
In the setting of acute CAD, rest MPS has been shown to be of value on a research basis in assessing the effectiveness of therapeutic approaches to limiting infarct size. Stress MPS can also be of use in the subacute setting. In this regard, The INSPIRE (AdenosINe Sestamibi Post-InfaRction Evaluation) trial has recently been completed, assessing the value of serial assessment of survivors of acute MI. In this trial 205 patients with ejection fraction ≥ 35% demonstrating 10%−20% ischemia by quantitative rest/adenosine 99mTc-sestamibi SPECT were randomized to aggressive medical treatment versus aggressive medical treatment with angioplasty. The results of follow-up adenosine MPS performed an average of 3 mo after randomization revealed similar substantial improvements in ischemia and in ejection fraction in both groups. Also, the longer-term prognosis was similar in the patients randomized to medical therapy and in those treated with angioplasty. These results illustrate that the response to therapy can be assessed by serial MPS and that substantial improvements in ischemia can be achieved with medical therapy alone, potentially allowing a lower-risk subset to be identified after MI in whom angioplasty may not be beneficial over medical therapy alone. Results from the COURAGE and BARI 2D trials may allow extension of these concepts to patients with chronic CAD.
In patients undergoing revascularization after MPS, a postrevascularization study can objectively document the effectiveness of the revascularization procedure. Though this is often of research interest, it is not considered necessary for clinical care as a routine on all postrevascularization patients. In selected high-risk patients for whom improvement in risk needs to be documented (e.g., diabetic patients with silent ischemia subjected to percutaneous coronary intervention) such testing may be warranted.
CMR TO TRACK PROGRESSION OF ATHEROSCLEROTIC DISEASE
CMR for assessment of the response to therapy offers some interesting potential applications. Several studies have demonstrated that CMR can be used to provide reproducible noninvasive assessment of atherosclerotic lesions. Though assessment of coronary plaque has to date proven difficult because of the small size and motion of the coronary arteries, the carotid arteries and the aorta have been successfully imaged. Yuan et al. have documented that carotid imaging is able to characterize different parts of carotid lesions and to objectively evaluate regression of lesions on therapy (74). The thoracic aorta offers the advantage of greater size over the carotids and may become a commonly used target for CMR assessment of plaque. This plaque imaging approach could be used to document the end-organ effect of novel antiatherosclerosis therapies, potentially being of value in the development of new therapies as well as in monitoring the effectiveness of therapy in the individual patient. Furthermore, because of the highly accurate assessments of myocardial volumes, ejection fraction, and infarct size of cardiac CMR studies, these studies could also be effective in monitoring the effects of therapy.
FUTURE CONSIDERATIONS
Given the recent emergence of coronary CTA as an effective noninvasive procedure for CAD detection, it is likely that the growth rate of MPS will be reduced over the next several years from the double-digit annual growth that has been experienced for nearly 20 y; at the same time, the need for MPS in patients with equivocal coronary CTA studies, and the increased number of patients with known CAD in whom coronary CTA is not currently effective, will be counterbalancing this effect, resulting in a probable modest continued growth of MPS in the United States.
In patients with known CAD, MPS and PET approaches are likely to remain cost-effective for identification of which of these patients are most likely to benefit from medical therapy versus coronary revascularization or myocardial reshaping procedures. If problems of cardiac and respiratory motion can be solved, nuclear imaging, in conjunction with coronary CTA, could potentially image rupture-prone coronary plaque. CMR procedures are also likely to grow, given the unique capabilities of MRI for assessment of scars and its ability to evaluate effectively many different aspects of the cardiovascular system without radiation. However, the similarity of CMR to simpler, cheaper, and more patient friendly and widely available echocardiography approaches may limit the growth, particularly in the cardiac area (as opposed to the vascular area).
CONCLUSION
This review has indicated that there is an interaction between the noninvasive assessment of coronary anatomic abnormality—through the CCS or possibly even the noninvasive coronary angiogram—and the assessment of the functional consequences of atherosclerosis using gated MPS, PET, or, potentially, CMR. Additional information of clinical importance may come from assessment of biomarkers of inflammation such as elevated levels of high-sensitivity C-reactive protein (75) or, more recently, lipoprotein-associated phospholipase A2 (76), which appears to be even more specific for vascular inflammation. Because of the strength of the evidence supporting the use of MPS and PET, the ease and effectiveness with which these approaches can be used in patients with known disease and in the elderly, and the great, untapped potential of these approaches in molecular imaging, we consider it likely that there will continue to be growth for several years in the use of MPS and PET for assessing patients with known or suspected cardiovascular disease.
Acknowledgments
This research was funded in part by a grant from The Eisner Foundation.
Footnotes
-
Guest Editor: H. William Strauss
-
↵* NOTE: FOR CE CREDIT, YOU CAN ACCESS THIS ACTIVITY THROUGH THE SNM WEB SITE (http://www.snm.org/ce_online) THROUGH JULY 2007.
-
↵ † Opinions expressed in this article are those of the authors alone. The Journal of Nuclear Medicine welcomes differing opinions in order to stimulate discussion with the ultimate goal of enhancing patient diagnosis and treatment.
-
COPYRIGHT © 2006 by the Society of Nuclear Medicine, Inc.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.
- 32.
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- Received for publication July 8, 2005.
- Accepted for publication April 26, 2006.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
- Article
- Abstract
- PROGNOSTIC APPLICATIONS OF MYOCARDIAL PERFUSION SPECT (MPS)
- POST-MPS PATIENT OUTCOMES
- ADDED VALUE OF FUNCTION PARAMETERS FROM MPS
- USING MPS FOR DECIDING BETWEEN MEDICAL AND REVASCULARIZATION THERAPY
- PROGNOSTIC SIGNIFICANCE OF CORONARY CALCIUM SCORE (CCS)
- GUIDING PATIENT MANAGEMENT DECISIONS BY CCS
- PROGNOSTIC APPLICATIONS OF CTA
- SCREENING FOR CORONARY ATHEROSCLEROSIS: APPROACH TO USE OF CT FOR CCS, CTA, AND MPS IN ASYMPTOMATIC PATIENTS
- DETECTION AND MANAGEMENT OF CAD: APPROACH TO USE OF CT FOR CCS, CTA, AND MPS IN SYMPTOMATIC PATIENTS
- EVALUATING RESPONSE TO TREATMENT
- CCS
- MPS
- CMR TO TRACK PROGRESSION OF ATHEROSCLEROTIC DISEASE
- FUTURE CONSIDERATIONS
- CONCLUSION
- Acknowledgments
- Footnotes
- References
- Figures & Data
- Info & Metrics
Related Articles
Cited By...
- The Future of Nuclear Medicine as an Independent Specialty
- Impact of an Automated Multimodality Point-of-Order Decision Support Tool on Rates of Appropriate Testing and Clinical Decision Making for Individuals With Suspected Coronary Artery Disease: A Prospective Multicenter Study
- Non-ST-Segment Elevation Acute Coronary Syndromes: Targeted Imaging to Refine Upstream Risk Stratification
- Prognostic Value of CT Angiography in Patients With Inconclusive Functional Stress Tests
- Can Coronary Computed Tomographic Angiography Trigger Coronary Revascularization?: Questioning the Appropriateness of the Question
- Noninvasive Diagnostic and Prognostic Assessment of Individuals With Suspected Coronary Artery Disease: Coronary Computed Tomographic Angiography Perspective
- Nuclear Cardiac Stress Testing in the Era of Molecular Medicine
- Added Value of Coronary Artery Calcium Score as an Adjunct to Gated SPECT for the Evaluation of Coronary Artery Disease in an Intermediate-Risk Population