


Abstract
In vitro studies have demonstrated that 99mTc-methoxyisobutylisonitrile (99mTc-MIBI) is a transport substrate of multidrug resistance (MDR)-related proteins. The aim of this clinical study was to evaluate whether 99mTc-MIBI scintigraphy was a functional imaging tool for in vivo detection of multidrug resistance-associated protein (MRP) expression in osteosarcoma and to investigate the role of MRP and 99mTc-MIBI imaging to predict the clinical outcome. We also examined whether the scintigraphic parameters would help to distinguish the functional capacity of P-glycoprotein (Pgp) and MRP. Methods: Twenty-four patients with a diagnosis of osteosarcoma were studied before neoadjuvant chemotherapy. Tumor-to-background ratios of both early (10 min) and delayed (1 h) images and the percentage washout rate (WR%) of 99mTc-MIBI were calculated. Immunohistochemical analysis of MRP and Pgp was performed on biopsy specimens, and the response to preoperative chemotherapy was assessed by histopathologic examination. Results: Fifteen of 24 osteosarcoma samples in our series (62.5%) showed significant expression of MRP. The level of MRP expression was significantly correlated with the WR% of 99mTc-MIBI (r = 0.58, P = 0.003), and the WR% of 99mTc-MIBI was significantly faster in patients with high MRP expression than in those with a low MRP score (P = 0.007). The clearance rate of 99mTc-MIBI was significantly slower in tumor samples with negative or low expression of both Pgp and MRP (16% ± 6.2%) when compared with osteosarcomas with high expression of both proteins (31.7% ± 8.7%) (P = 0.001). There was not a significant difference between the WR% of 99mTc-MIBI in tumors with coexpression of both proteins and in tumors with high expression of either Pgp or MRP. Both the rate of MRP expression and the WR% of 99mTc-MIBI were significantly correlated with response rate. Conclusion: Our results suggest that the WR% of 99mTc-MIBI is correlated with MRP expression. Both the WR% of 99mTc-MIBI and MRP expression are correlated with therapy response. 99mTc-MIBI can be used as a general probe for functional imaging of both Pgp and MRP; however, it is not capable of differentiating the functional status of either MDR-related glycoprotein.
- multidrug resistance
- multidrug resistance-associated protein
- P-glycoprotein
- osteosarcoma
- 99mTc-methoxyisobutylisonitrile
Osteosarcoma is the most frequent primary malignant bone tumor. Although the outcome of osteosarcoma has improved considerably with the application of multiagent chemotherapy regimens, systemic relapses are observed in 50% of cases (1,2). The cross-resistance to many structurally unrelated drugs limits the success of multidrug-based chemotherapy regimens.
One type of multidrug resistance (MDR) is caused by the transport of drugs over the plasma membrane, which is mediated by adenosine triphosphate (ATP)-dependent transmembrane transporter proteins, P-glycoprotein (Pgp) and multidrug resistance-associated protein (MRP) (3,4). Conventional cytotoxic agents used in the treatment of osteosarcoma are substrates of Pgp and MRP, including doxorubicin, which is the most effective agent for osteosarcoma management (1,5). Several authors have described the expression of Pgp in tumor samples and defined this membrane transport protein as an important adverse prognostic factor in patients with osteosarcoma (2,6–9). On the other hand, overexpression of MRP has been reported in various tumors, including hematologic malignancies (10,11), human soft-tissue sarcoma (12,13), lung cancer (14), and Ewing’s sarcoma (15). In these studies, various detection assays were applied to obtain information about the presence of transport proteins at messenger RNA and protein levels. However, MDR is not only defined by the number of Pgp or MRP on tumor cells but also by the functional transport capacity of drug efflux pumps (16). 99mTc-Methoxyisobutylisonitrile (99mTc-MIBI) is one of the agents that have been studied to measure Pgp and MRP transport function (17–20). Bone and soft-tissue tumors constitute an ideal model to study the role of 99mTc-MIBI, and in a recent report we observed significant correlation between the efflux rate of 99mTc-MIBI and the Pgp expression in patients with musculoskeletal sarcomas (21). On the other hand, MRP expression in osteosarcomas has not been extensively studied. There are a few in vitro studies in the literature about the presence of MRP in osteosarcomas (22,23) but, to our knowledge, no clinical data regarding the expression of MRP in these tumors have been published.
The aim of this clinical study was to investigate the level of MRP expression in osteosarcoma and to evaluate whether 99mTc-MIBI scintigraphy was an adequate functional imaging tool for in vivo detection of MRP expression in patients with osteosarcoma. We also compared 99mTc-MIBI uptake and washout kinetics with the expression of Pgp. Because 99mTc-MIBI was reported to be a substrate of both transmembrane transport proteins, we intended to examine whether scintigraphic parameters would help to distinguish the functional capacity of the 2 MDR pumps in patients with osteosarcoma.
MATERIALS AND METHODS
Patients
A total of 24 patients who were referred to Ege University Musculoskeletal Oncology Council with a diagnosis of osteosarcoma were enrolled in this study. There were 17 males and 7 females (age range, 9–66 y; mean age, 25.33 ± 15 y). Twelve osteosarcomas were located in the distal femur, 6 in the proximal tibia, 4 in the proximal humerus, and 2 in the proximal femur.
Before starting any treatment, all patients were studied by 99mTc-MIBI scintigraphy. The patients were also evaluated by radiography, CT, MRI, and 3-phase bone scintigraphy. The local ethics committee approved the study protocol; all patients or their parents gave informed consent.
99mTc-MIBI Imaging Protocol
Dynamic flow imaging was performed on all patients after intravenous injection of 370–720 MBq 99mTc-MIBI while the patient was positioned supine on the imaging table. The detector was placed in the position that was closest to the whole tumor, and the images were obtained from the projection in which the tumor was best visualized. The data were acquired every 3 s for 3 min using a large-field-of-view gamma camera (Sophy DSX) equipped with a low-energy, general-purpose collimator (matrix, 64 × 64 pixels). After dynamic imaging, static planar images of the involved area (matrix, 256 × 256 pixels) were obtained at 10 min (early) and 1 h after injection (delayed) while the patient was lying in the same position.
Data Analysis
From early dynamic images, the ratio of tumor perfusion (TP) was calculated using identical regions of interest (ROIs) drawn over the lesion and the contralateral normal tissue. Ratios of average counts per pixel were determined.
Tumor-to-background (T/B) ratios of early and delayed images and the washout rate of 99mTc-MIBI were determined by the protocol defined previously (21). To calculate T/B ratios, a manual ROI was set on the lesion (T) and a symmetric ROI was set on the contralateral side (B) on 10-min images. Identical ROIs were applied to delayed images. The T/B ratio of both early and delayed images was calculated. After decay correction of the mean counts in the ROIs drawn on the delayed images, the percentage washout rate (WR%) of 99mTc-MIBI from the tumor was determined using the following formula:
Immunohistochemistry
Within 7 d after the scintigraphic procedure, the orthopedic surgeon performed at least 2 thick-needle biopsies from the different regions of the osteosarcoma.
Immunohistochemical staining was performed according to the standard streptavidin-biotin method. MRP6 (8770–01; Signet) was used as the primary antibody against MRP, and C494 (Dako) was used against Pgp. Sections (3-μm thick) were cut from 10% formalin-fixed and paraffin-embedded materials that were mounted on gelatin-coated glass slides. The sections were deparaffinized with xylene solution and washed in ethanol. The materials were treated with 3% methanol/hydrogen peroxidase to block endogenous peroxidase activity. To improve the antigenic determinants, an antigen-retrieval procedure was applied. The slides were washed with distilled water and replaced in a lam carrier. The sections were treated with sodium citrate solution (pH 6) and boiled in a microwave oven for 20 min. After washing with distilled water, the slides were treated for 3 min with Tris buffer (pH 7.6) washing solution, and a protein-blocking procedure (X0909; Dako) was applied to inhibit nonspecific protein binding. The specimens were incubated with primary antibodies, MRPm6 in a 1:75 dilution and C494 in a 1:150 dilution for 30 min and then washed with Tris buffer (pH 7.6). Antibody-bridge labeling was developed using the streptavidin biotin-peroxidase method. The final reaction product was revealed by exposure to diaminobenzidine solutions, and the nuclei were counterstained with hematoxylin.
Normal lymph nodes were used as positive controls for MRP, and tissue sections from normal kidneys including proximal tubules and adrenal cortex were accepted as positive samples for Pgp. Two independent observers who had no knowledge about the clinical information interpreted the results of immunostaining.
MRP expression was graded according to a semiquantitative scoring system from 0 to 3 as follows: 0 = absence of staining; 1 = rare immunostaining, scattered positive cells <10%; 2 = weak immunostaining, >10% positive cells; 3 = diffuse and strong immunostaining, >50% positive cells. The significant MRP expression was accepted as diffuse and strong immunostaining in >50% positive cells. The lowest point of the significantly positive immunostaining was score 3.
Positive expression of Pgp was based on the immunostaining of the plasma membrane and cytoplasm. The results were graded according to a semiquantitative scoring system covering both the distribution of positivity and the degree of immunostaining as follows: 0 = absence of staining; 1 = weak immunostaining, scattered positive cells <10%; 2 = strong immunostaining, scattered positive cells <10%; 3 = weak immunostaining, 10%–50% positive cells; 4 = strong immunostaining, 10%–50% positive cells; 5 = weak immunostaining, >50% positive cells; 6 = strong immunostaining, >50% positive cells. Detection of positive immunostaining in >10% of the cells was accepted as significant expression. The lowest point of significantly positive immunostaining was score 3.
Clinical Follow-Up
After the final diagnosis, all patients were treated with neoadjuvant chemotherapy under the supervision of an experienced medical oncologist in various combinations, including doxorubicin, cisplatin, ifosfamide, cyclophosphamide, vincristine, and high-dose methotrexate. Before surgical resection, each patient was reevaluated and the extent of the tumor was defined. A limb-salvage operation was performed on 19 patients, whereas 5 patients underwent an amputation procedure because of the progression of the primary lesion. Response to preoperative chemotherapy was assessed by histopathologic examination on surgically resected materials. Patients with a percentage of necrosis of >90% were considered as responders.
T/B ratios of both early and delayed images and the WR% of 99mTc-MIBI were compared with MRP and Pgp expression. All parameters were compared with therapy response.
Statistical Analysis
The data are expressed as mean ± SD. MRP and Pgp expression levels were compared with the T/B ratio and the WR% of 99mTc-MIBI using simple regression analysis and the Spearman rank correlation coefficient. The Levene test was used to test whether the samples had equal variance. When the data were distributed normally, differences in the mean values were assessed by the 2-tailed unpaired Student t test. The correlation between immunostaining, 99mTc-MIBI parameters, and therapy response was assessed by the Fisher exact test. P < 0.05 was accepted as significant.
RESULTS
Immunohistochemical Analysis
In 15 of 24 osteosarcoma samples (62.5%), MRP immunostaining was diffuse and strong (grade 3). In 3 cases, the expression of MRP was also diffuse but weak in intensity (grade 2). In this series, the lowest point of the significantly positive immunostaining was accepted as score 3. On this basis, the patients were divided into 2 groups with which the parameters of 99mTc-MIBI were correlated:
Immunostaining of group A was absent, rare, or weak immunostaining in <50% of the cells (scores 0, 1, and 2) and group B was consistent with strong MRP expression in >50% of the cells (score 3). The majority of the patients (15 patients) in our series demonstrated significant MRP expression (group B) and there were 9 patients in group A.
The expression rate of Pgp was determined according to our previous study (21). The lowest point of significantly positive immunostaining was score 3 for Pgp. There were 13 patients with strong Pgp expression. When coexpression of MRP and Pgp was analyzed, there were 10 patients in our series with strong expression of both transmembrane glycoproteins.
99mTc-MIBI Imaging Results
The patients’ characteristics are listed in Table 1. It was interesting to observe that all of the osteosarcomas in our series showed significant perfusion and 99mTc-MIBI uptake in early images. The mean ratio of TP was 3.15 ± 0.94. The smallest TP was observed in patient 8 as 1.5. The TP values were closely correlated with the early T/B ratios of 99mTc-MIBI (r = 0.55, P = 0.001). When we evaluated the uptake ratios of 99mTc-MIBI, the mean T/B ratios derived from early and delayed images were found to be 3.20 ± 1.4 and 2.35 ± 1, respectively. There was a significant difference between early and delayed uptake ratios (r = 0.51, P = 0.01). When we examined whether either early or delayed T/B ratios of 99mTc-MIBI were correlated with MRP expression, the results were not significant (r = 0.37 and r = 0.26, respectively). Furthermore, the early and delayed T/B ratios of patients with high MRP expression (group B) (3.59 ± 1.5 and 2.54 ± 1.2, respectively) were not significantly different from those of patients with low MRP expression (group A) (2.56 ± 0.8 and 2.02 ± 0.6, respectively).
Characteristics of Patients with Osteosarcoma and 99mTc-MIBI Parameters with Respect to MRP and Pgp Expression
Next, the rate of MRP expression was compared with the WR% of 99mTc-MIBI, and a significant positive correlation was observed (r = 0.58, P = 0.003) (Fig. 1). Figure 2 also demonstrates 99mTc-MIBI imaging of a patient (patient 14, Table 1) with strong MRP expression. The clearance rate of 99mTc-MIBI was fast (WR%, 40%) in correlation with the significant MRP expression. After neoadjuvant chemotherapy, the percentage of necrosis in the resection material was <90%.

WR% of 99mTc-MIBI with respect to level of MRP expression. Positive correlation is found between 99mTc-MIBI efflux and MRP score (P = 0.003).
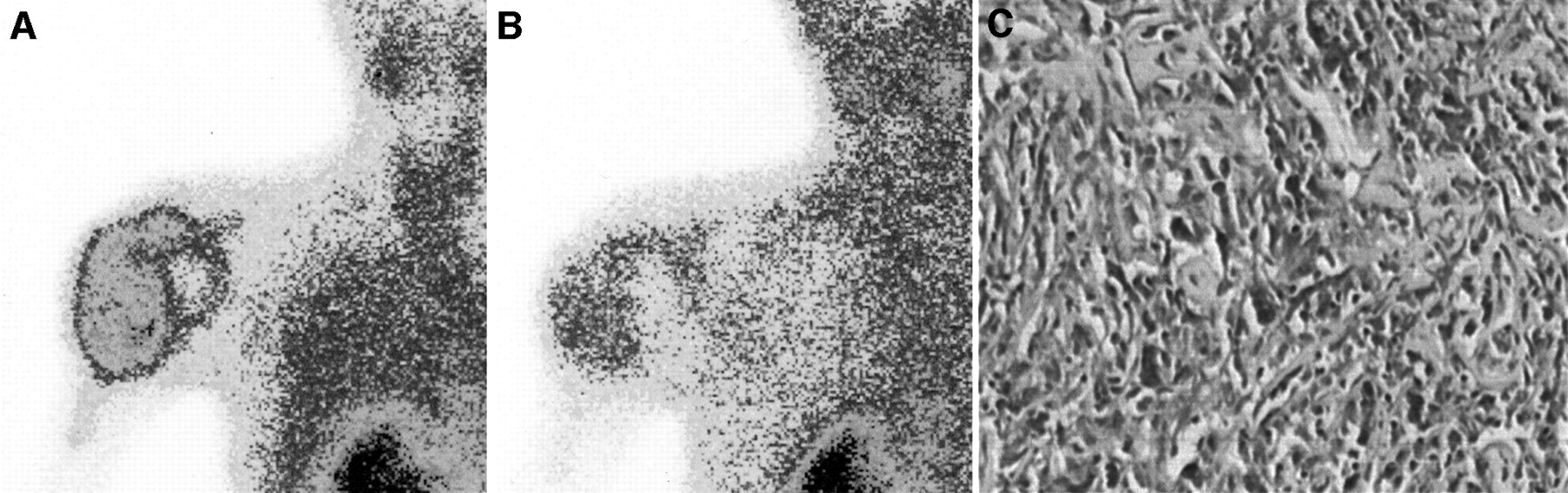
A 24-y-old woman with osteosarcoma in left humerus (patient 14). (A) Early 99mTc-MIBI image shows intense tracer accumulation in tumor. (B) Late 99mTc-MIBI study demonstrates significant clearance of 99mTc-MIBI (WR%, 40%). (C) Immunohistochemical analysis of biopsy specimen is consistent with strong and diffuse MRP expression.
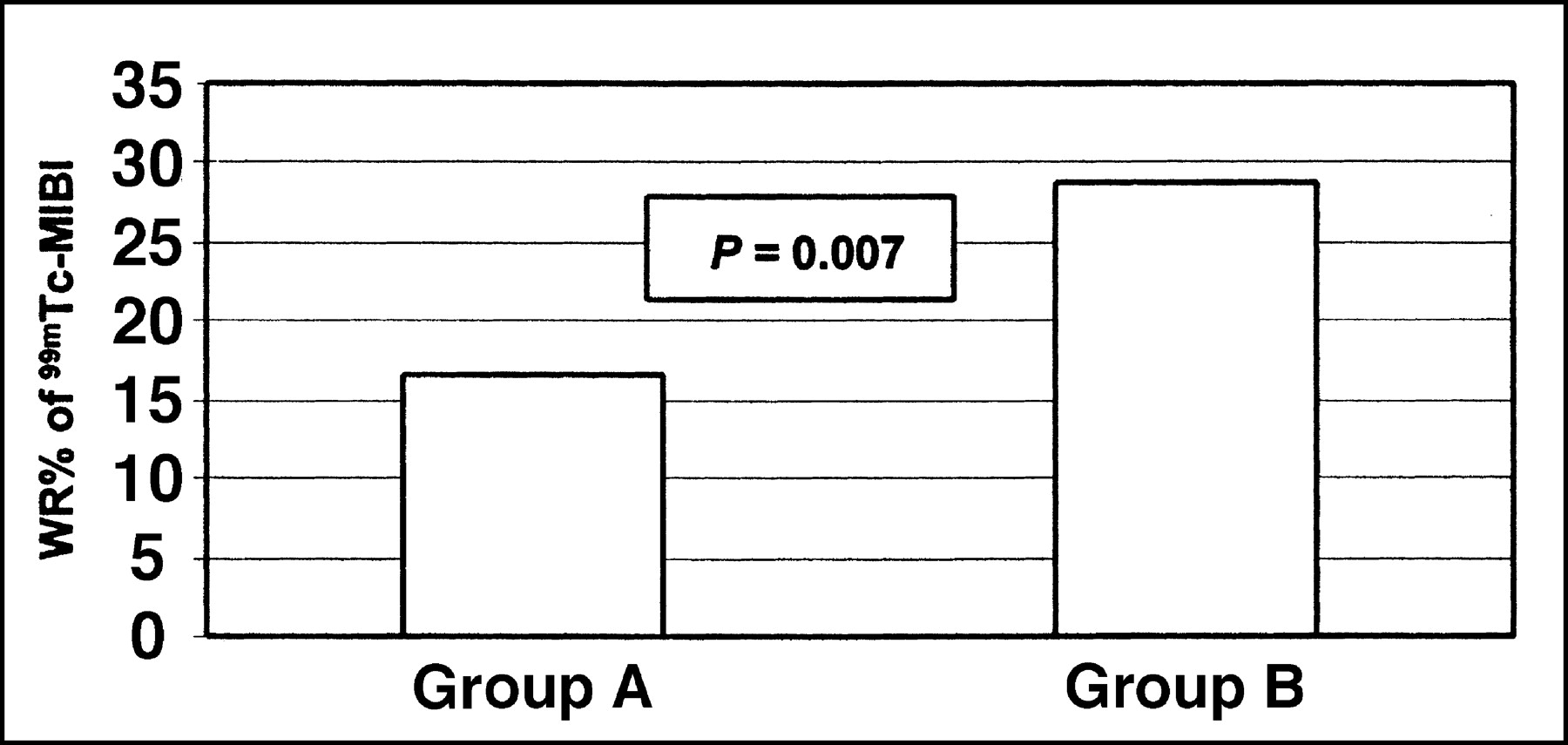
When the WR% values of patients in group B were compared with those of patients in group A, it was interesting to note that the WR% values of 99mTc-MIBI were significantly faster in patients with high MRP expression than those of patients with a low MRP score (30.1% ± 8.6% vs. 20% ± 7.7%; P = 0.007) (Fig. 3). When a cutoff value of 1 SD below the mean WR% was used (<22%) to discriminate the cases with high and low MRP expression, there were 4 patients (patients 2, 6, 9, and 22) with discordant results. In 3 of these patients (patients 2, 6, and 9), there was significant Pgp expression with respect to a low MRP score. In patient 22, both transmembrane proteins were significantly expressed, although the WB% 99mTc-MIBI was low. There were also 3 borderline cases with a WR% equal to 22% (patients 7, 10, and 16) (Table 1).

Significant difference is found between WR% of patients with high MRP expression (group B) and those with low MRP score (group A) (30.1% ± 8.6% vs. 20% ± 7.7%; P = 0.007).
Correlation of 99mTc-MIBI Results with MRP and Pgp Expression
The rate of Pgp expression in osteosarcomas in our series is demonstrated in Table 1. Because we intended to investigate whether the scintigraphic parameters would help to distinguish the functional capacity of the 2 MDR-related proteins, MRP and Pgp, we divided the cases into 3 groups according to the immunostaining results as follows: There were 6 patients with negative or low expression of both Pgp and MRP (group 1), 10 patients with high expression of both Pgp and MRP (group 2), and 8 patients with high expression of either Pgp or MRP (group 3).
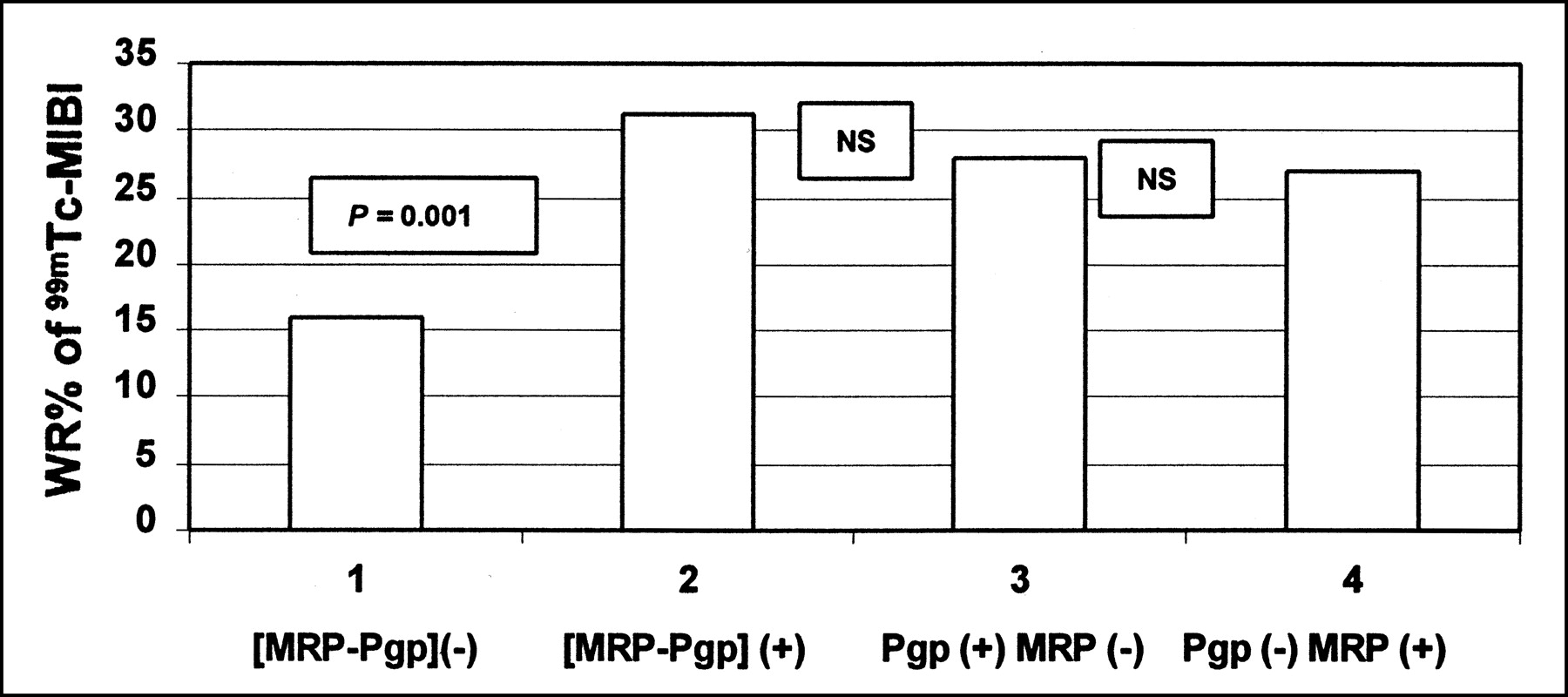
The mean WR% of 99mTc-MIBI in group 1 was calculated as 16% ± 6.2%. On the other hand, the mean WR% of 99mTc-MIBI in osteosarcomas with strong expression of both MRP and Pgp (group 2) was 31.7% ± 8.7%, and this value was significantly different from that of the group that had low expression of both membrane proteins (P = 0.001) (Figure 4). When we analyzed the WR% of 99mTc-MIBI in cases with high expression of either MRP or Pgp (group 3), it was interesting to observe that the mean WR% of 99mTc-MIBI in osteosarcomas with high Pgp and low MRP expression was not different from that of patients with strong MRP expression and a low Pgp score (28% ± 1% vs. 27.8% ± 4.3%; P > 0.05). Also, the mean WR% of 99mTc-MIBI in groups 2 and 3 was not significantly different, whereas both groups showed faster washout rates of 99mTc-MIBI with respect to group 1. These results suggested that the WR% of 99mTc-MIBI would help to distinguish osteosarcomas with low or negative Pgp/MRP expression from tumors that express significant levels of both or either of the transmembrane proteins.
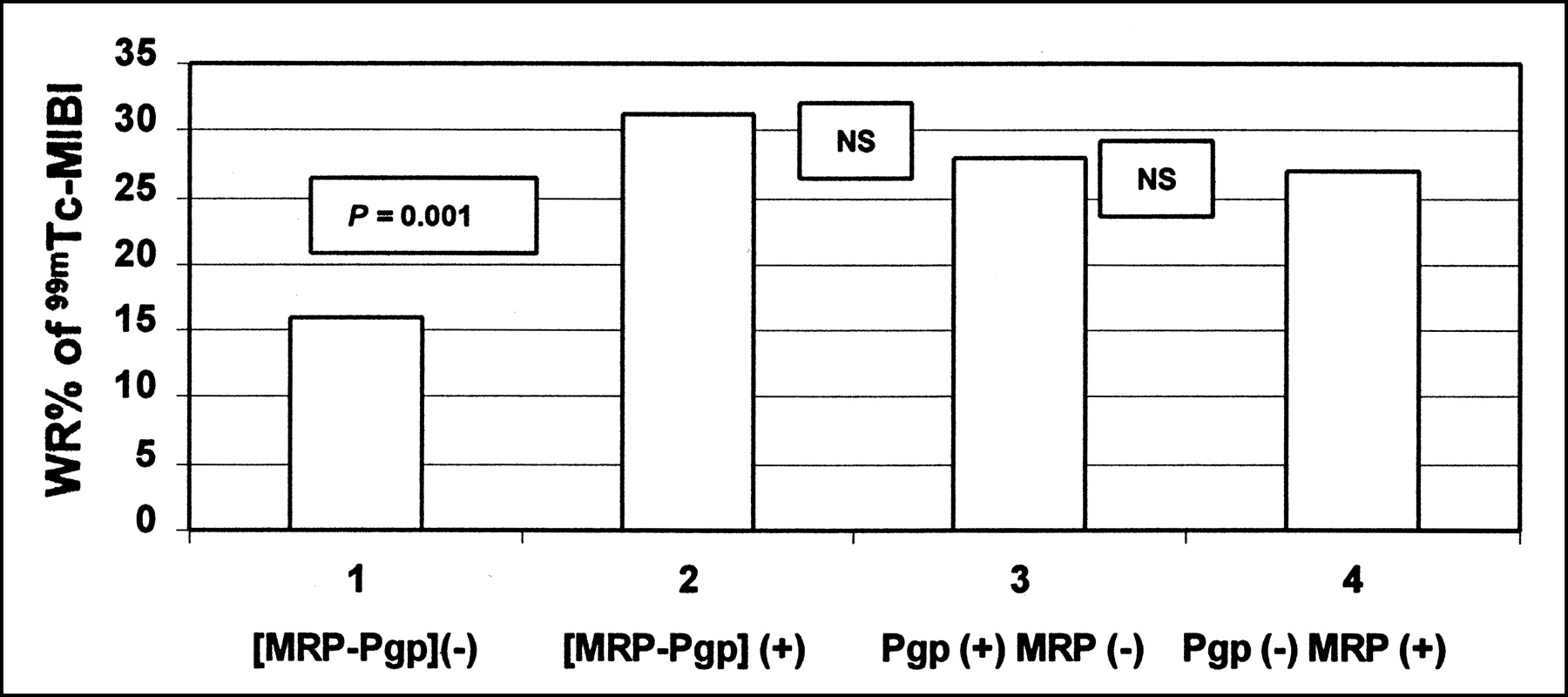
WR% of 99mTc-MIBI in group 1 (both Pgp and MRP negative) is significantly slower than that of group 2 (both Pgp and MRP positive), group 3 (Pgp positive and MRP negative), and group 4 (MRP positive and Pgp negative). Difference between groups 2, 3, and 4 is not significant (NS).
Response to Multiagent Chemotherapy
After neoadjuvant chemotherapy, only 6 of 24 patients (25%) were considered as good responders (histologic tumor necrosis, ≥90%). The remaining 18 patients were accepted as nonresponders. Although the size of the patient population is limited, we found a significant negative correlation between the rate of MRP expression and the percentage of necrosis of the resection materials (r = −0.46, P = 0.02) (Table 2). When the cutoff value of 22% (derived from 1 SD below the mean WR% of 99mTc-MIBI) was used, there was also a close correlation between WR% values and the therapy response in patients with osteosarcoma (r = −0.55, P = 0.005) (Table 2). We did not identify any correlation between the chemotherapy response and the level of Pgp expression in osteosarcomas in our series.
Relationship Between Chemotherapy Response and Degree of MRP Expression and WR% of 99mTc-MIBI
DISCUSSION
The survival rate of osteosarcoma is not encouraging, despite the use of aggressive therapeutic regimens. Because the main cause of treatment failure is drug resistance, preoperative risk evaluation is important to predict response to chemotherapy at the time of diagnosis to limit the long-term morbidity and to reduce the economic consequences of intensive therapy programs. Many clinical prognostic parameters have been investigated so far to select groups of patients who are at a higher risk of systemic relapse. In this respect, the expression of Pgp, the MDR product of the gene MDR1, was studied and Pgp expression was reported to be associated with drug resistance, recurrence, and poor prognosis in patients with osteosarcoma (2,6–9). Another transmembrane glycoprotein, MRP, was also characterized as a drug exporter belonging to the ATP-binding super family (5,22). The significant expression of MRP was reported in osteogenic sarcoma cell lines in preclinical cell culture studies (23,24), but there have been no clinical published data about the expression of MRP in these tumors. To our knowledge, our study group is the first series to demonstrate significant MRP expression in patients with osteosarcoma. Fifteen of 24 osteosarcoma samples (62.5%) showed high levels of MRP. This finding is important because membrane transport by MRP involves a large drug spectrum, consisting of doxorubicin, one of the most effective drugs in the treatment of osteosarcoma (25). Therefore, overexpression of MRP should be kept in mind in osteosarcomas with low or negative Pgp expression. Despite a considerable overlap in substrate specificity between Pgp and MRP, major differences have been reported. Although the mechanism of MRP-mediated transport has not been clearly defined, MRP may act as a glutathione-S-conjugate efflux pump (GS-X pump) by transporting chemotherapeutic agents, which are conjugated or cotransported with glutathione (GSH) (16,26,27). GSH plays an important role in cellular defense against alkylating agents. Increased GSH levels were reported to be consistent with cisplatin resistance (28). An in vitro study demonstrated the correlation between intrinsic GSH content and cisplatin resistance in osteosarcoma cell lines (29), and the overexpression of glutathione-S-transferase was also found to be associated with failure of preoperative chemotherapy (30). These reports address the need for further studies with a large number of patients to validate the interaction between MRP and GSH in osteosarcoma.
The MDR in osteosarcoma is not only defined by the expression of transmembrane transporter proteins but also by the functional transport capacity of these drug efflux pumps. In this respect, our study demonstrated that the WR% of 99mTc-MIBI was significantly correlated with the rate of MRP expression and was higher in patients with high MRP expression than in those with a low MRP score. In full agreement with our previous study (21), we did not find a significant correlation between T/B uptake ratios of 99mTc-MIBI and MRP expression. Therefore, on the basis of our results, early imaging with 99mTc-MIBI may not be sufficient to evaluate the expression of MRP in osteosarcomas. Delayed imaging is recommended to determine the WR% of 99mTc-MIBI. When a cutoff value of 1 SD below the mean WR% of group B (<22%) was used to discriminate the patients with high or low MRP expression, the sensitivity of 99mTc-MIBI imaging was 93%. Fourteen of 15 tumors with high MRP expression had an efflux rate higher than the cutoff value. However, 5 of 9 osteosarcomas with low MRP expression showed an efflux rate slower than the cutoff value; the specificity was found to be 55%. Although there is a close correlation between the WR% of 99mTc-MIBI and the MRP score, our patient population is not large enough to determine a standard cutoff value to discriminate the tumors with high and low MRP expression. Because 99mTc-MIBI was also a substrate for Pgp, the high number of false-positive results in this study (44%) may be explained by the significant expression of Pgp in osteosarcoma samples, which have a negative MRP score. There were 4 patients with discordant results and, in 3 of them (patients 2, 6, and 9) (Table 1), Pgp expression was significant and the WR% of 99mTc-MIBI was high, whereas MRP was negative. Although the pump function of transmembrane transport proteins is regulated by many factors, coexpression of Pgp may also affect and reduce the specificity of 99mTc-MIBI imaging for predicting the functional status of MRP.
To examine whether the scintigraphic parameters would help to discriminate the functional capacity of MRP and Pgp, we divided the patients into 3 groups according to the immunostaining results and compared the WR% of 99mTc-MIBI. It was interesting to observe that the clearance rate of 99mTc-MIBI was significantly slower in tumors with negative or low expression of both Pgp and MRP when compared with that of tumors with high expression of both proteins (P = 0.001). Preclinical studies showed that 99mTc-MIBI was actively pumped, not only by Pgp but also by MRP, and the active efflux efficiency was very similar for both transporters (20). Our study in osteosarcomas supports this in vitro observation in a clinical manner and demonstrates that the WR% of 99mTc-MIBI is closely correlated with the pump function of MDR-related proteins. On the other hand, the significant difference between the scintigraphic parameters of tumors with high and low glycoprotein expression led to the hypothesis that negative scintigraphy may support the low expression of MDR-related proteins in osteosarcoma. Those tumors may benefit from the standard regimens that may provide a reasonably good chance of long-term survival. On the other hand, there was not a significant difference between the WR% of 99mTc-MIBI in tumors with coexpression of both proteins and high expression of either Pgp or MRP. This means that, with 99mTc-MIBI imaging, it may not be possible to distinguish osteosarcomas with significant expression of both Pgp and MRP from the tumors expressing either transport protein.
The histologic response to multiagent chemotherapy is generally considered one of the most reliable indicators of the clinical outcome of osteosarcoma. In our series, therapy response was determined by analysis of the percentage of necrosis in the resection materials. When ≥90% tumor necrosis was accepted as a good response to multiagent chemotherapy, 18 of 24 patients in our series (75%) were nonresponders. Although the number of patients is not large, we observed a significant correlation between the rate of MRP immunostaining and the percentage of necrosis in the resection materials. In accordance with MRP expression, there was also a significant correlation between the WR% of 99mTc-MIBI and the therapy response when the previously defined cutoff value (22%) was used to distinguish the cases with fast and slow 99mTc-MIBI clearance. In the light of these findings, 99mTc-MIBI imaging seems to be a promising modality to identify the overexpression of MRP in osteosarcoma as an indicator of therapy response, thereby enabling selection of patients for new treatments that combine drugs that are capable of overcoming the MRP-mediated mechanism of drug resistance. Because our study group is not large enough to make conclusions about the prognostic value of MRP in predicting event-free survival in osteosarcoma, the accuracy of our findings should be reproduced by further studies with an extended number of patients.
We did not find any correlation between the chemotherapy response and the level of Pgp expression in our study. The relation between the level of Pgp expression and the extent of tumor necrosis after chemotherapy has not been clarified yet. Many studies stress the overexpression of Pgp as a significant determinant in prediction of the therapy response (7,9,31), whereas others report that the level of Pgp expression is not correlated with therapy failure (32). The controversies between those investigations may be caused mainly by methodologic differences. No single technique is ideal for the detection of MDR. Methods such as polymerase chain reaction and Northern blotting are able to measure surface glycoproteins at messenger RNA levels. However, these are applied to bulk tumor homogenates and suffer from the interference by nontumor stromal cells. In this respect, immunohistochemistry is more practical and is able to detect MDR-related proteins in individual cells or small clusters of tumor cells. In our study, the expression rate of MRP and Pgp was based on both the degree and the extent of immunostaining of tumor cells by comparison with that of the stromal cells. On the other hand, we believe that, the use of 2 or more anti-glycoprotein antibodies may improve the reliability of immunohistochemical detection by recognizing different epitopes of the transport proteins.
CONCLUSION
This preliminary study demonstrates the significant level of MRP expression in patients with osteosarcoma and supports earlier reports that the washout rate of 99mTc-MIBI is correlated with MRP expression, with a significant difference between patients with high and low MRP activity. 99mTc-MIBI imaging is a promising modality to predict preoperative chemotherapy response in osteosarcoma because both the WR% of 99mTc-MIBI and the rate of MRP expression are closely correlated with clinical outcome. Functional imaging with 99mTc-MIBI may provide a unique modality to characterize in vivo resistance in osteosarcoma to direct patients to specific cancer therapies, thereby monitoring reversal agents. Our results demonstrate that 99mTc-MIBI can be used as a general probe for functional imaging of the 2 MDR proteins; however, 99mTc-MIBI imaging is not capable of differentiating the functional presence of MRP from that of Pgp.
Acknowledgments
This work was supported by a grant from University Agreement between l’Université Paris XIII, Bobigny, France, and Ege University Medical Faculty, İzmir, Turkey.
Footnotes
Received Jan. 18, 2003; revision accepted May 15, 2003.
For correspondence or reprints contact: Zeynep Burak, MD, Department of Nuclear Medicine, Ege University Medical Faculty, Bornova 35100 İzmir, Turkey.
E-mail: zburak{at}egenet.com.tr
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Effects of Neoadjuvant Chemotherapy on Image-Directed Planning of Surgical Resection for Distal Femoral Osteosarcoma
- Retention of the Radiotracers 64Cu-ATSM and 64Cu-PTSM in Human and Murine Tumors Is Influenced by MDR1 Protein Expression
- Characterization of a 67Ga/68Ga Radiopharmaceutical for SPECT and PET of MDR1 P-Glycoprotein Transport Activity In Vivo: Validation in Multidrug-Resistant Tumors and at the Blood-Brain Barrier