


Abstract
The aim of this study was to evaluate the efficacy of 177Lu-prostate-specific membrane antigen (PSMA)-617 (177Lu-PSMA) and selective internal radiation therapy (SIRT) for the treatment of liver metastases of castration-resistant prostate cancer. Methods: Safety and survival of patients with metastatic castration-resistant prostate cancer and liver metastases assigned to 177Lu-PSMA alone (n = 31) or in combination with SIRT (n = 5) were retrospectively analyzed. Additionally, a subgroup (n = 10) was analyzed using morphologic and molecular response criteria. Results: Median estimated survival was 5.7 mo for 177Lu-PSMA alone and 8.4 mo for combined sequential 177Lu-PSMA and SIRT. 177Lu-PSMA achieved discordant therapy responses with both regressive and progressive liver metastases in the same patient (best vs. worst responding metastases per patient: −35% vs. +63% diameter change; P < 0.05). SIRT was superior to 177Lu-PSMA for the treatment of liver metastases (0% vs. 56% progression). Conclusion: The combination of 177Lu-PSMA and SIRT is efficient and feasible for the treatment of advanced prostate cancer. 177Lu-PSMA alone seems to have limited response rates in the treatment of liver metastases.
Despite marked progress in recent years, the therapy of metastatic castration-resistant prostate cancer (mCRPC) remains a substantial clinical challenge, especially since liver metastases are still associated with poor overall survival (1,2). This is partly caused by a dedifferentiation of the prostate cancer cells in liver metastases, a process that is called neuroendocrine transdifferentiation and is associated with poor survival (3,4). Radioligand therapies targeting the prostate-specific membrane antigen (PSMA) have been applied to patients with advanced mCRPC in multiple studies (5–8). Among the variety of available radioligands, 177Lu-PSMA-617 (177Lu-PSMA) is most commonly used. Preliminary data suggest that 177Lu-PSMA extends progression-free and overall survival while exhibiting a favorable toxicity profile (5,9,10). However, 177Lu-PSMA seems to be less efficacious for the treatment of liver and other visceral metastases (5). In contrast, selective internal radiation therapy (SIRT) specifically targets liver metastases with great efficacy and therefore represents a treatment option for unresectable primary liver cancer or metastases in the liver (11). To date, however, there is no systematic evaluation of 177Lu-PSMA therapy or SIRT as a local liver therapy for liver metastases in advanced prostate cancer. Therefore, the aim of the present retrospective single-center study was to evaluate the efficacy of 177Lu-PSMA and SIRT in mCRPC patients with liver metastases and elucidate the implications for overall survival.
MATERIALS AND METHODS
Patients
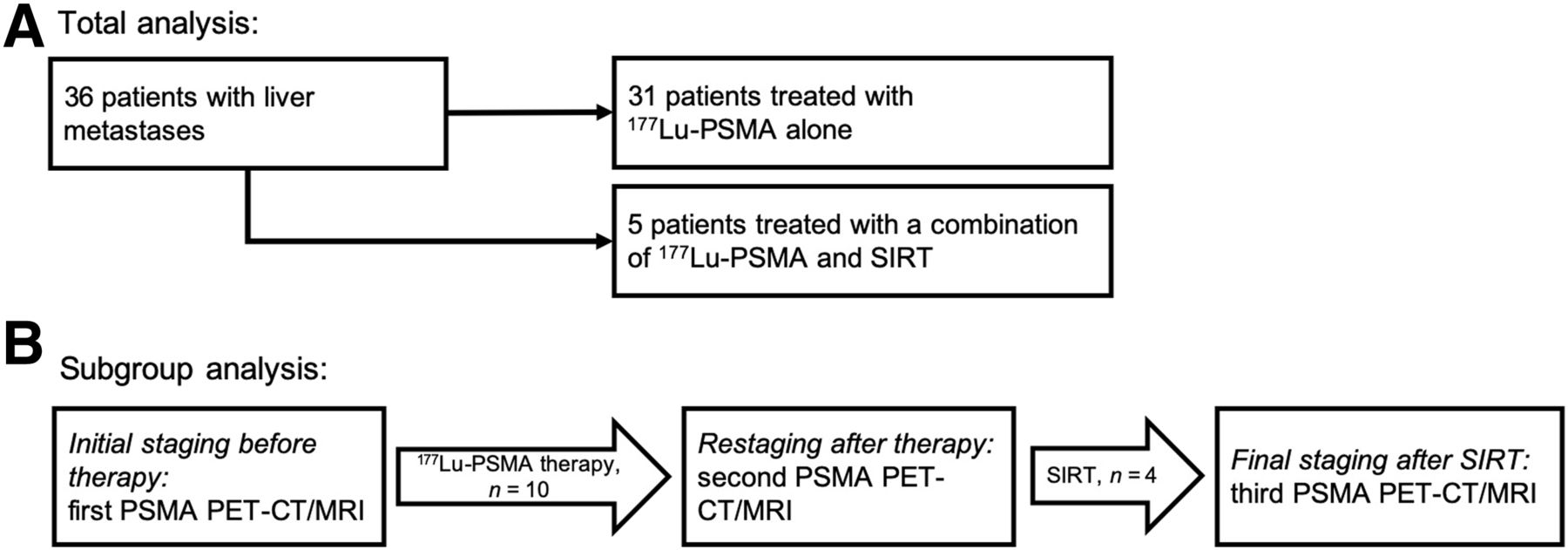
Figure 1 presents the flowchart for patient selection. All patients with mCRPC and liver metastases referred to the Department of Nuclear Medicine for therapy were considered for this case series (n = 36). Patients with metastases were treated with PSMA-targeted therapy alone (n = 31) or in combination with SIRT (n = 5) based on individual tumor board decisions and with informed consent (Supplemental Table 1; supplemental materials are available at http://jnm.snmjournals.org). SIRT was pursued if the extrahepatic tumor burden was controlled but the hepatic metastases were progressive (no overall therapy failure). Under this criterion, only 5 patients were eligible to be treated with SIRT. Toxicity was evaluated according to the Common Toxicity Criteria for Adverse Events (CTCAE, version 5.0).
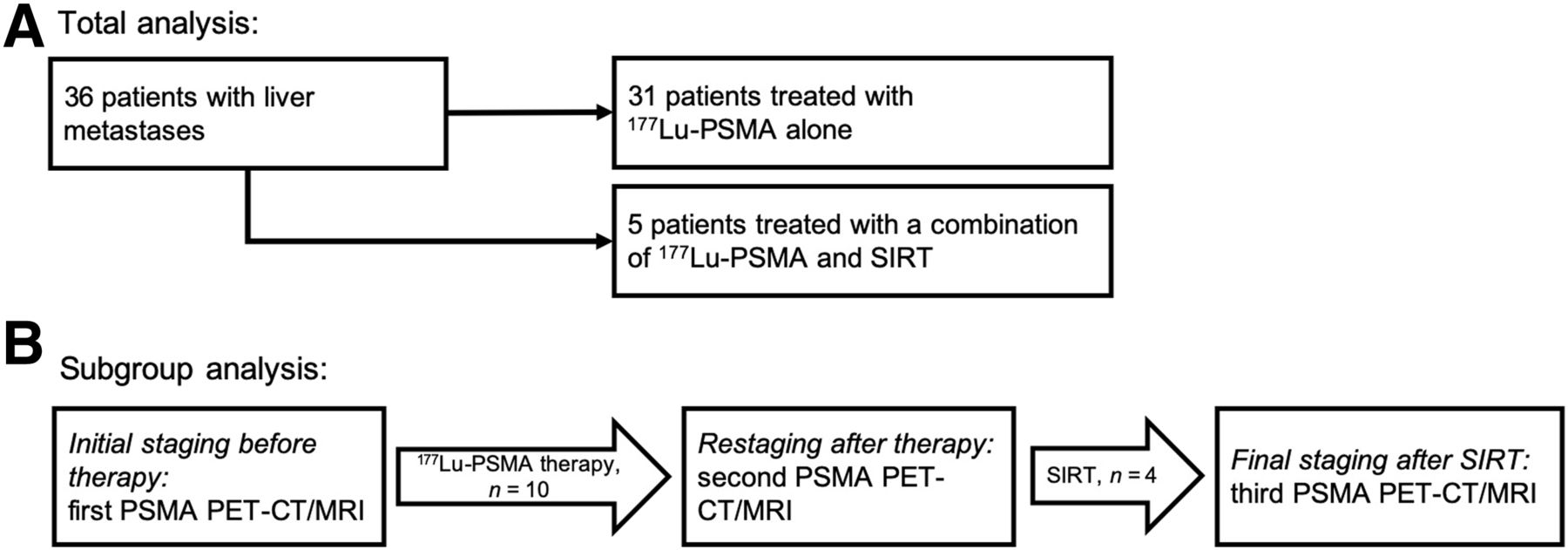
(A) Flowchart of patient selection for overall survival analysis. (B) Examination sequence for subgroup analysis (PSMA PET/CT or MRI before radionuclide treatment = baseline, after 177Lu-PSMA = restaging, and after SIRT = final staging).
The following 2 inclusion criteria were applied for the subgroup analysis: the presence of liver metastases and the availability of PET imaging before and after radionuclide therapy. All 10 patients analyzed in detail received 177Lu-PSMA therapy; 4 patients were additionally treated with SIRT because of hepatic progress despite controlled extrahepatic tumor burden (Supplemental Table 2). The retrospective analysis of patients treated with 177Lu-PSMA was approved by the local ethics committee (approval 2016-585-f-S, Ethikkommission der Ärztekammer Westfalen-Lippe und der Westfälischen Wilhelms-Universität Münster).
PSMA-Targeted Radionuclide Therapy
Conjugation of PSMA-617 with 177Lu has been described previously (12). The β-radiation of 177Lu (maximum energy, 0.497 MeV) has a maximum tissue range of 2 mm (13). PSMA-617 was manufactured by ABX GmbH. Whole-body scintigraphy was performed after 48 h to monitor the retention of 177Lu-PSMA in prostate cancer metastases. An administered target activity of 6–7.5 MBq was used per cycle, and the cycles were repeated after 7–8 wk. Exclusion criteria for 177Lu-PSMA were a leukocyte level of less than 2,000/μL, a platelet level of less than 75,000/μL, a hemoglobin level of less than 8 g/dL, a creatinine level of more than 2 mg/dL, and aspartate and alanine transaminase levels greater than 5 times the upper limit of normal (14).
SIRT
After selective catheterization, 90Y microspheres were directly injected into the hepatic artery or its branches to cause radioembolization of metastases. Microspheres were manufactured by SIRTEX Medical. The β-particles of 90Y (maximum energy, 2.27 MeV) have a maximum tissue range of 11 mm (13). The administered SIRT activity was calculated according to European Association of Nuclear Medicine guidelines (dependent on body surface area and relative tumor volume) (15). Exclusion criteria for radioembolization were the presence of ascites, elevated levels of bilirubin (cutoff, 2.0 mg/dL), a hepatopulmonary shunt of more than 20% (assessed by 99mTc-macroaggregated albumin [99mTc-MAA] scintigraphy), or persisting blood flow from the hepatic arteries to the gastrointestinal tract (evaluated by 99mTc-MAA scintigraphy and angiography) (16,17). Patients were evaluated by angiography and injection of 99mTc-MAA into the hepatic arteries 2 wk before the SIR treatment. SPECT and 99mTc-MAA scintigraphy were used to estimate the relative hepatic tumor volume and to determine whether the metastases were hypervascularized. All lesions showed an accumulation of 99mTc-MAA at least at the margin and also within the target lesions. An example is given in Supplemental Figure 1. Toxicity after SIRT and 177Lu-PSMA therapy was evaluated using Common Terminology Criteria for Adverse Events (version 5).
Imaging
Whole-body staging (vertex to proximal tibia) was done using PSMA-based PET imaging before the start of 177Lu-PSMA therapy (initial staging), after the last cycle of 177Lu-PSMA (restaging), and after SIRT, so that the therapy effect could be clearly attributed to the precedent therapy. Contrast-enhanced MRI or CT was performed.
The Department of Nuclear Medicine switched from 68Ga-PSMA-11 to 18F-PSMA-1007 for logistic reasons during the interval of this study. Therefore, whole-body staging was done using either tracer if no external acquisition was present. For 68Ga-PSMA-11-PET, 2 MBq per kilogram of body weight were injected, and the PET acquisition took place 60 min after tracer administration (the 68G was generated using a GalliaPharm [Eckert and Ziegler]; the PSMA-11 precursor was manufactured by ABX GmbH). For 18F-PSMA-1007, 4 MBq per kilogram of body weight were injected, and the scans were acquired 120 min after tracer administration (tracer synthesis was performed using a TracerLab MX synthesizer [GE Healthcare]; PSMA-1007 precursor was provided by ABX GmbH]).
A Biograph mMR PET/MRI system or a Biograph mCT PET/CT system was used to sequentially acquire PET/MRI and PET/CT images (Siemens Healthcare). Whole-body MRI comprised an axial T2-weighted HASTE (half-Fourier acquisition single-shot turbo spin-echo), an axial and coronal T1-weighted VIBE (volumetric interpolated breath-hold examination) with fat suppression (after injection of a gadolinium-containing contrast agent), and an axial T2-weighted turbo spin-echo sequence of the liver. Contrast-enhanced abdominal CT or MRI was performed using standard parameters.
Response Evaluation
Estimated mean overall survival was used as the primary endpoint to compare PSMA-targeted therapy alone (n = 31) or in combination with SIRT (n = 5). Additionally, the response to SIRT or 177Lu-PSMA was assessed using morphologic and molecular features in the subgroup analysis (n = 10). Morphologic response was assessed in analogy to RECIST, version 1.1, and was reported only for liver metastases: up to 4 of the largest hypervascularized hepatic metastases were defined as target lesions, and the sum of their long-axis diameters (LADs) was measured (progressive disease = 20% increase of LADs or newly formed metastases, partial response = 30% decrease of LADs, stable disease = neither progressive disease nor partial response, and complete response = no lesions definable) (18). SUVmax was measured at baseline in all liver metastases to determine whether 177Lu-PSMA therapy was feasible. Additionally, the change in PSMA expression caused by SIRT was analyzed as a molecular response.
Statistical Analysis
SPSS statistics, version 25 (IBM), was used for testing and descriptive statistics. Unpaired (Mann–Whitney U) and paired (Wilcoxon) nonparametric statistical tests were performed. Values are presented as median; the range or confidence intervals (CIs) are additionally specified. A statistically significant difference was assumed if the P value was less than 0.05; otherwise, nonsignificance is reported. The Kaplan–Meier method was used to estimate the median survival, and the log-rank method was used to test for survival differences.
RESULTS
Patient Characteristics and Therapies
All patients were treated with androgen deprivation therapy (Table 1). One additional patient was evaluated for SIRT but could not receive treatment because, in comparisons with previous imaging, the disease was found to be rapidly progressing. The average interval between 177Lu-PSMA administrations was 7.5 wk (95% CI, 6.7–9.3 wk); a median of 3 therapy cycles was administered, and the average dose was 6.2 GBq (95% CI, 6.2–6.5 GBq). A mean dose of 2.2 GBq of 90Y was used (range, 1.3–2.5 GBq) (n = 5).
Patient Characteristics
Survival
The estimated median overall survival (n = 31) was 5.7 mo (95% CI, 2.9–8.5 mo) for patients receiving only 177Lu-PSMA. For patients receiving 177Lu-PSMA and SIRT (n = 5), the estimated median overall survival was 8.4 mo (95% CI, 4.9–11.9 mo). The estimated overall survival for 177Lu-PSMA and SIRT was not significantly longer than that of 177Lu-PSMA alone (log rank P = 0.227).
Subgroup Analysis of Efficacy of PSMA-Targeted Therapy
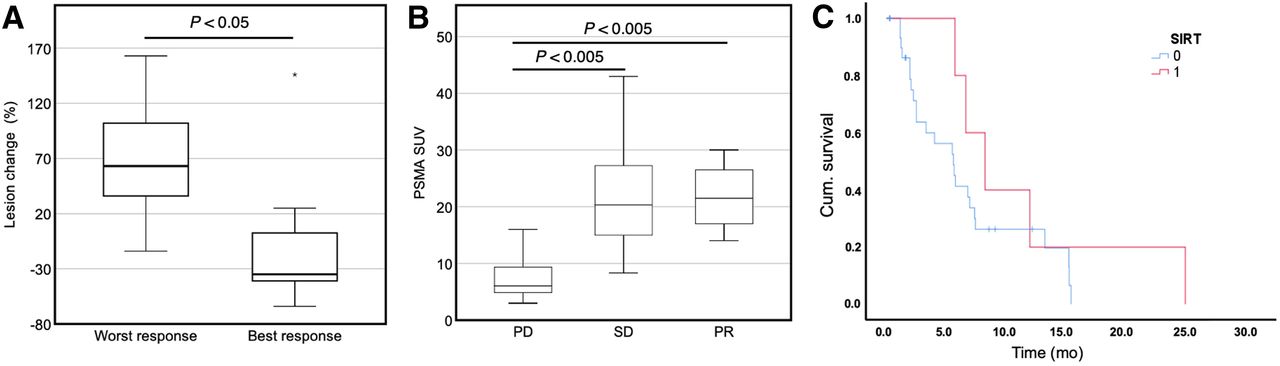
Treated by 177Lu-PSMA therapy, liver metastases showed progressive disease compared with the baseline examination in 56% of patients; however, 44% displayed stable disease (9 patients; patient 3 was not considered here because initial SIRT was followed by 177Lu-PSMA therapy). Liver metastases had a discordant response: the best- and worst-responding lesions were significantly different if multiple liver metastases were present (only patients with multiple liver metastases at baseline were included [n = 7]; +63% vs. –35% LAD change [P < 0.05]; Figs. 2 and 3).

Discordant response of liver metastases to 177Lu-PSMA in patient 6, who was treated with 6 cycles of 177Lu-PSMA. Shown are CT or MRI (top) and PET/CT or MRI (bottom) images. (A) Before start of 177Lu-PSMA therapy, major liver metastases were seen in both lobes (arrow). (B) After treatment with 4 cycles of 177Lu-PSMA, metastases were decreasing (dashed circle). (C) Small liver metastases were also detected in segment V. (D) However, after 2 additional cycles, metastases were progressive and showed only modest PSMA uptake caused by dedifferentiation (arrowheads).
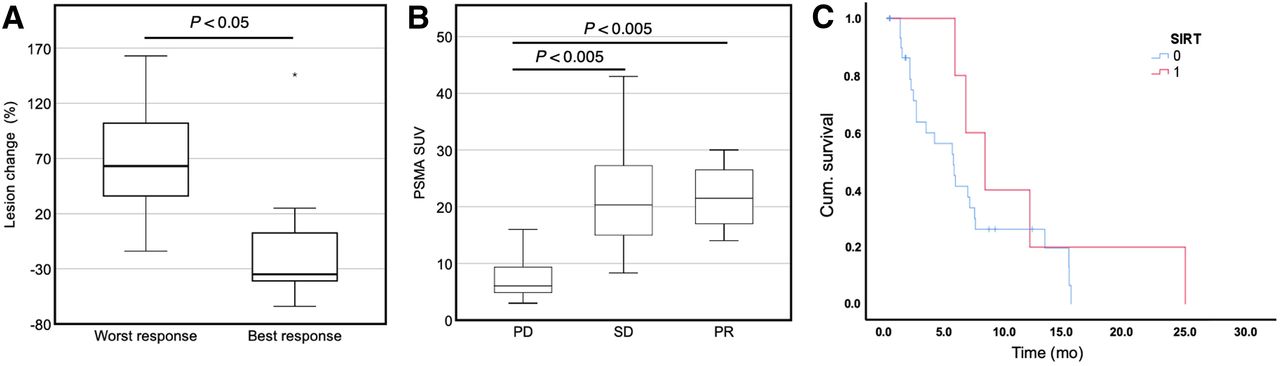
Evaluation of 177Lu-PSMA and SIRT efficacy. (A) 177Lu-PSMA achieved only discordant responses by liver metastases; therefore, changes in size for best- and worst-responding lesions were compared (only patients with multiple liver metastases at baseline were included [n = 7]). (B) Overall, liver metastases responded significantly differently to 177Lu-PSMA therapy. Treatment with 177Lu-PSMA therapy was efficient only in patients with strong 68Ga-PSMA-11 uptake by liver metastases. SUVmean of lesions was reported separately for progressive disease (PD), stable disease (SD), and partially responding (PR) liver metastases (only patients with 68Ga-PSMA-11 radionuclide were included [n = 8]). (C) Overall survival of patients treated with 177Lu-PSMA alone (median, 5.7 mo; blue) did not significantly differ from that of patients treated with combination of 177Lu-PSMA and SIRT (median, 8.4 mo; red).
When the liver metastases of all patients were rated individually, morphologically progressive lesions showed significantly less 68Ga-PSMA-11 uptake at baseline than did stable and regressive ones (only patients with 68Ga-PSMA-11 radionuclide were included [n = 8]; SUVmax of 6.1 for progressive disease, 20.3 for stable disease, and 21.5 for partial response [P < 0.005]; Fig. 3).
Subgroup Analysis of Efficacy of SIRT
The mean follow-up time point was 9 wk after SIRT (range, 3–13 wk; Fig. 4). When morphologic criteria were applied, 75% showed a partial response (3 patients) and 25% had stable disease (1 patient). The best- and worst-responding lesions did not significantly differ (n = 4; −19% vs. –44% LAD change).
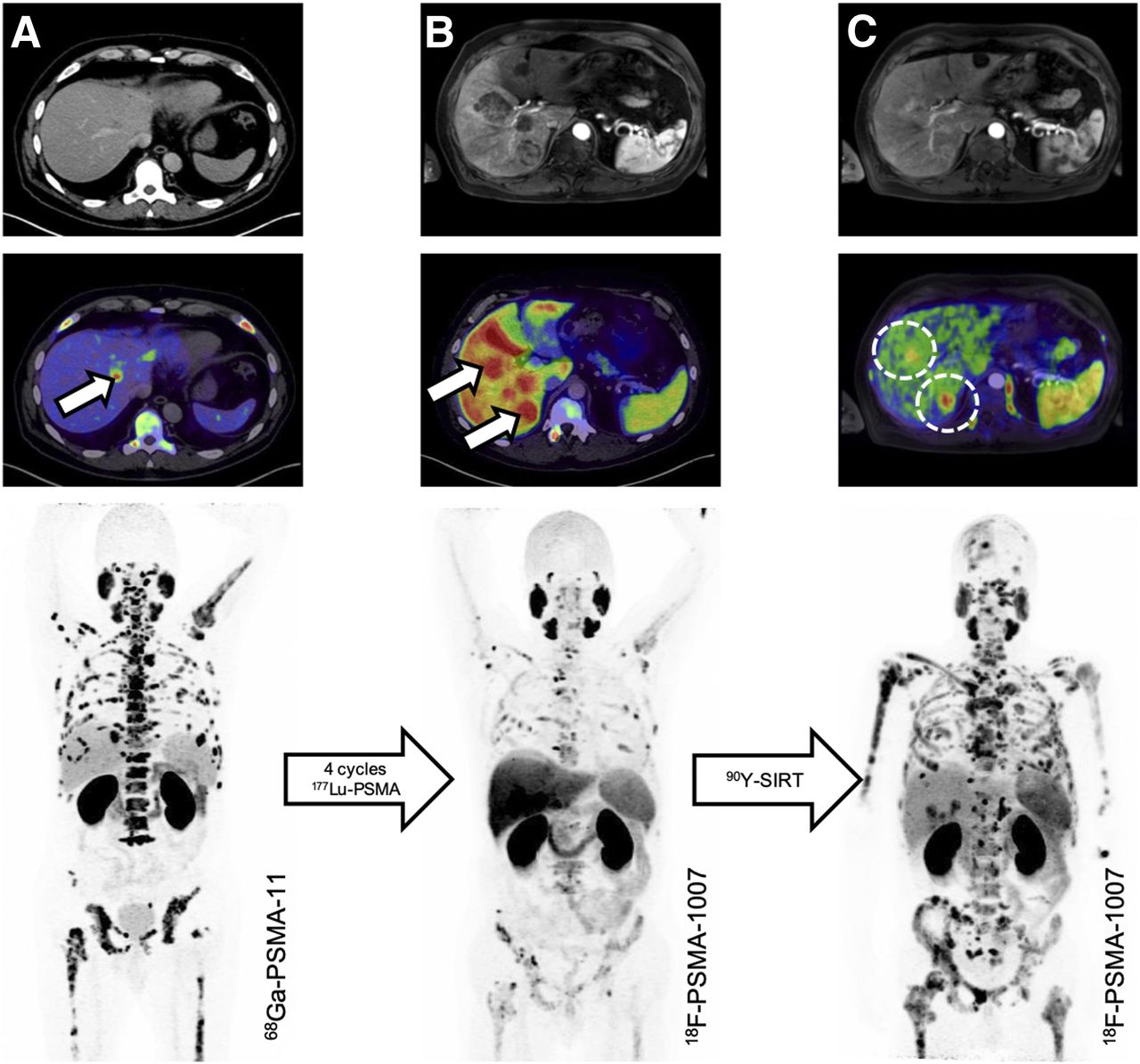
Response of liver metastases to 177Lu-PSMA and SIRT in patient 1, who was treated with 4 cycles of 177Lu-PSMA initially, followed by SIRT. Shown are CT (top), PET/CT (middle), and whole-body maximum-intensity projection (bottom) images before therapy (A), after 4 cycles of 177Lu-PSMA (B), and after 90Y-SIRT (C). Compared with pretherapy scan, liver metastases were progressive after 177Lu-PSMA and extrahepatic metastases were regressive (arrows). After SIRT, liver metastases had responded and had no relevant PSMA expression (dashed cycles). However, extrahepatic metastases were severely progressive, as can be seen on the maximum-intensity projection.
The molecular response evaluation revealed that PSMA uptake by liver metastases was reduced by a median of 39% after SIRT (range, +4% to −83%).
Toxicity
The hepatic toxicity of 177Lu-PSMA therapy alone versus 177Lu-PSMA therapy in combination with SIRT is presented in Supplemental Tables 3 and 4 according to the Common Terminology Criteria for Adverse Events (version 5). Briefly, there were significant differences in alanine aminotransferase (+160.0% vs. +14.6%; P = 0.006), aspartate aminotransferase (+130.3% vs. +25.42%; P = 0.007), and γ-glutamyltransferase (+652.1% vs. +2.6%; P = 0.0003) between 177Lu-PSMA and SIRT versus 177Lu-PSMA alone, but there was no significant difference in bilirubin.
DISCUSSION
The aim of this study was to evaluate the efficacy and safety of 177Lu-PSMA and SIRT for the treatment of advanced mCRPC with liver metastases, compared with 177Lu-PSMA alone. Patients treated with 177Lu-PSMA showed a discordant response to therapy, with both regressing and progressing metastases at the same time. The reason for this discordance currently remains unclear. Even initial responses to PSMA therapy may be misleading for a long-term response prediction. Initial responses to 177Lu-PSMA may not be associated with long-term remission, as newly occurring metastases might not respond to additional 177Lu-PSMA cycles. This behavior might partly be explained by the neuroendocrine transdifferentiation of prostate cancer cells, which is associated with poor overall survival (3,19). In the transdifferentiation process, neuroendocrine cell markers (such as the neuron-specific enolase) are expressed, whereas adenocarcinoma markers (such as the prostate-specific antigen) are lost (19). The neuroendocrine differentiation is frequently present in liver metastases, which might partially explain the occurrence and progression of PSMA-negative metastases under 177Lu-PSMA therapy that was shown in the present study (3). However, the fact that patients treated with SIRT did not show a discordant hepatic response indicates its superiority for the treatment of liver metastases. This superiority might be due to the independence of SIRT from target molecules; therefore, neuroendocrine differentiation should not decrease its efficacy. Moreover, initial treatment of liver metastases with SIRT might prevent the spread of neuroendocrine differentiated tumor cells to other organs.
SIRT obtained higher response rates and a longer mean overall survival for the treatment of liver metastases than 177Lu-PSMA. The mean SIRT-delivered tumor dose for colorectal metastases is 55 Gy (20). 177Lu-PSMA therapy delivers mean tumor dosages of 32 Gy (for 6 GBq of 177Lu) (21). For colorectal metastases, a deposition of at least 60 Gy is favorable for prolonged overall survival (20). Despite the fundamental difference in tumor biology between prostate cancer and colorectal cancer, the distinct efficacy of 177Lu-PSMA and SIRT might be partially explained by the delivered doses.
The increase in aspartate aminotransferase, alanine aminotransferase, and γ-glutamyltransferase levels was significantly higher in the SIRT group than in patients treated with 177Lu-PSMA alone. However, baseline and posttherapeutic liver enzymes were compared in order to evaluate the overall toxicity. Therefore, the increase in liver enzymes is at least partly attributable to the progression of hepatic metastases rather than to hepatotoxicity. Moreover, the increase in bilirubin levels was not significantly different.
The limitations of the present study comprise the retrospective data analysis, small patient cohort, and potential selection bias. However, liver metastases are an end-stage phenomenon of prostate cancer and thus generally rare. Therefore, the presented initial results are valuable and have direct implications for the treatment of prostate cancer and liver metastases, especially in cases of castration resistance and 177Lu-PSMA evaluation. In the present article, SIRT was the only evaluated local treatment for the liver metastases. Therefore, future studies should investigate whether other local therapies of liver metastases, such as transcatheter arterial chemoembolization or extracranial stereotactic radiotherapy, are efficient as well. An additional limitation is the efficacy assessment of 177Lu-PSMA and SIRT therapy, which was based on morphologic features. Future studies should consider additional imaging modalities such as 18F-FDG PET or diffusion-weighted MRI for the evaluation of treatment response, especially in the context of neuroendocrine transdifferentiation (22).
CONCLUSION
The combination of 177Lu-PSMA and SIRT is efficacious and feasible for the treatment of liver metastases in advanced mCRPC. 177Lu-PSMA alone seems inferior to SIRT for the treatment of liver metastases.
DISCLOSURE
Kambiz Rahbar reports being a compensated consultant for ABX and has received consultant fees from Bayer and lectureship fees from Janssen Cielag, Amgen, AAA, and SIRTEX. The University of Münster received consulting fees from ABX GmbH, Radeberg, Germany, for Kambiz Rahbar and Martin Boegemann. No other potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: Is the combination of a local (SIRT) and a systemic (177Lu-PSMA) radionuclide therapy feasibly tolerable in patients with mCRPC to the liver?
PERTINENT FINDINGS: This retrospectively analyzed patient group indicated that the combination of SIRT and 177Lu-PSMA is feasible and effective. Use of 177Lu-PSMA alone yields discordant responses by liver metastases, whereas SIRT efficiently targets all liver metastases.
IMPLICATIONS FOR PATIENT CARE: In addition to systemic 177Lu-PSMA therapy, local therapies targeting liver metastases should be evaluated in further clinical studies.
Footnotes
Published online Oct. 10, 2019.
- © 2020 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication July 8, 2019.
- Accepted for publication September 20, 2019.





{kind=link}
{kind=link}
{kind=link}
{kind=link}