


Abstract
Paragangliomas are rare neuroendocrine tumors that may arise anywhere along the paraganglial system, with a high frequency of hereditary forms or multifocal disease. Most often, paragangliomas are benign and progress slowly, but metastases may occur in about 10% of patients. In this respect, nuclear imaging in combination with anatomic imaging may be required to fully delineate the extent of the disease. PET has been increasingly used in imaging paraganglioma, paralleled by great efforts toward the development of new tracers. Recent data indicate that the choice of PET tracers should be tailored to tumor localization and to the patient's genetic status. This article provides insight into the many PET radiotracers that are currently available and others that are still only under research and guides clinicians toward appropriate use in relation to genetic carrier status. In addition, this article provides nuclear medicine physicians with the background knowledge required for understanding relationships between imaging phenotypes and molecular genetics.
Paragangliomas are tumors that develop from endocrine cells derived from pluripotent neural crest stem cells and are associated with neurons of the autonomic nervous system. They may arise anywhere along the paraganglial system and can be associated with the sympathetic nervous system or the parasympathetic nervous system. The former derive from the adrenal medulla, the organ of Zuckerkandl, or other chromaffin cells that may persist beyond embryogenesis, whereas the latter develop from endocrine cells in parasympathetic branchiomeric paraganglia (chemoreceptors), mainly located in the head and neck. Thus, paragangliomas can be distributed from the skull base to the sacrum, with a preference for certain sites: middle ear (glomus tympanicum), the dome of the internal jugular vein (glomus jugulare), between the carotid arteries (carotid body), along the vagus nerve, in the mediastinum (from the aortopulmonary body or the thoracic sympathetic chain), in the adrenal medulla, and in the abdominal paraaortic regions. Based on the classification published in 2004 by the World Health Organization, the term pheochromocytoma should be reserved solely for adrenal paraganglioma. Although catecholamine hypersecretion is almost a constant feature in pheochromocytoma and sympathetic paragangliomas, only 5% of parasympathetic paragangliomas are norepinephrine-secreting tumors.
Paragangliomas are characterized by a high frequency of hereditary forms (overall, 25%) with a propensity for multifocal disease (1–5). Most often, paragangliomas are benign and progress slowly, but metastases may occur in about 10% of patients.
Nuclear imaging in combination with anatomic imaging may be required to fully delineate the extent of the disease. Recent data indicate that the choice of PET tracer should be tailored to tumor localization and to the patient's genetic status.
SPECTRUM OF GENE MUTATIONS IN PARAGANGLIOMAS
Paragangliomas are characterized by diverse anatomic locations. Some correlations between the gene involved and tumor location have been found.
Molecular genetic research has so far resulted in identification of 10 susceptibility genes for tumors of the entire paraganglial system, including succinate dehydrogenase SDHB, SDHC, SDHD, Von Hippel-Lindau disease (VHL), RET (REarranged during Transfection) in Multiple Endocrine neoplasia type 2 (MEN2), neurofibromatosis type 1 (NF1), and the very recently reported susceptibility genes SDHAF2, transmembrane protein 127 (TMEM127), SDHA, and myc-associated factor X (MAX).
Pheochromocytoma may coexist with other tumor types in MEN2A and MEN2B, VHL, and NF1. In MEN2 patients, medullary thyroid carcinomas most often (>95%) reveal the disease. VHL is an autosomal dominant disorder, which also predisposes to renal clear cell carcinoma, pancreatic serous cystadenoma and neuroendocrine tumor, and hemangioblastoma of the eye and central nervous system. NF1 is characterized by the presence of multiple neurofibromas, café au lait spots, Lisch nodules of the iris, and other rare disorders. Extraadrenal paraganglioma may also occur in multiple neoplasia syndromes such as VHL, Carney–Stratakis dyad, and Carney triad (of unknown origin).
In this direction, fundamental work has been done by Baysal et al. in Pittsburgh, who identified the SDHD gene as the susceptibility gene of paraganglioma syndrome type 1 (paraganglioma type 1) (6). It was anticipated that other subunits could become candidates for recognition. Consequently, paraganglioma types 3 and 4 have been described as associated with germline mutations of the genes SDHC and SDHB, respectively (7,8).
A study was conducted by an international consortium for finding germline mutations in 989 patients with apparently nonsyndromic, adrenal, extraadrenal retroperitoneal, and thoracic paraganglial tumors (5). Predictors for an SDHx mutation were family history for paraganglial tumors, previous adrenal or extraadrenal pheochromocytoma, multiple paragangliomas, and age 40 y or more. The mutations were found in about two thirds in the SDHB gene, followed by mutations of the genes SDHD and VHL.
Mutations in susceptibility genes, other than SDHx, are rare in head and neck paragangliomas (HNPs) (9). The likelihood of identifying germline mutations in HNP patients was addressed by Neumann et al. in 2009 (10). Of 598 HNP patients, 31% had SDHx germline mutations (52% were SDHD mutations, 34% SDHB, and 14% SDHC). Predictors for an SDHx mutation were family history of paraganglial tumors, previous adrenal or extraadrenal pheochromocytoma, multiple HNPs, age 40 y or more, and male sex.
Paragangliomas with an underlying SDHB mutation are associated in about 30% of the carriers with an aggressive behavior and the development of metastatic disease (11).
The susceptibility gene for paraganglioma type 2 is SDHAF2 (also called SDH5) and was identified after years of intensive research by an American–Dutch cooperation in 2009 (12). Only HNPs have been reported. So far, a single mutation is known, and potentially all patients are related (13).
The search continued until 2010, when the SDHA gene—which had been a candidate since 2000—was also recognized as a tumor suppressor gene associated with paraganglial tumors (14,15).
Meanwhile, Dahia's group identified the gene TMEM127 as a susceptibility gene for paraganglial tumors, though her report suggested that only the adrenal was shown as the site of such tumors (16,17). Recently, the spectrum of manifestations in patients with TMEM127 mutations has been extended also to HNPs (18). Finally, in 2011, the MAX gene was identified using exome sequencing (19). So far, only 12 patients with MAX mutations are known, and all had adrenal tumors only.
CHALLENGES OF NUCLEAR IMAGING
Pheochromocytomas and abdominal extraadrenal paraganglioma usually cause symptoms of catecholamine oversecretion. By contrast, HNPs are often nonsecreting tumors but can be revealed by symptoms of compression or infiltration of the adjacent structures. The diagnosis can be established biochemically or, in cases of typical imaging features, by using different anatomic and functional imaging modalities.
Functional imaging is probably not necessary in the preoperative work-up of patients with negative genetic testing and a small pheochromocytoma. However, since the genetic status is often not available before surgery, the possibility of multifocal or metastatic disease should be considered (or excluded) in all cases, and nuclear imaging is useful in this regard (20). If there is no family history, the need to exclude multiple lesions is particularly important in younger patients (≤40 y) and patients with a larger pheochromocytoma (>5.0 cm) (21).
In extraadrenal paraganglioma or hereditary syndromes, as well as in identifying metastatic paraganglioma, the role of pretherapy imaging is crucial for accurately staging the disease. In this respect, nuclear imaging has a leading role. Precise identification of clinical context and genetic status of patients enables a personalized use of functional imaging studies (22,23). Although the extra cost and availability of new PET tracers can prove problematic, the option of not using them could lead to inappropriate management, with an adverse effect on management that should not be underestimated. It is expected that the early detection of paraganglioma may minimize complications related to mass effect and hormonal excess, facilitate curative treatment, and potentially reduce metastatic spread.
One important but unresolved question is whether early detection of small and biochemically silent paragangliomas in family members would improve the prognosis of patients.
LIMITATIONS OF SPECT
131I/123I-metaiodobenzylguanidine (MIBG) scintigraphy and 111In-diethylenetriaminepentaacetic acid (DTPA)-pentetreotide scintigraphy are the most commonly used conventional nuclear imaging techniques. MIBG is taken up from the circulation by adrenergic/sympathomedullary tissues via norepinephrine transporter (NET) (type I uptake), whereas pentetreotide binds to somatostatin receptor (SST) 2. 131I/123I-MIBG scintigraphy is the traditional imaging modality for catecholamine-secreting tumors. Scanning is usually performed after 48 h for 131I-MIBG or after 24 h for 123I-MIBG. Based on studies conducted without comparison to high-resolution PET, 131I-MIBG scintigraphy has sensitivity of 77%–90% and specificity of 95%–100% in the detection of pheochromocytomas. 123I-MIBG scintigraphy has better sensitivity (88%–96%) than 131I-MIBG because the energy of 123I photons is better suited for detection with γ-cameras, has no β-emission, and has a shorter isotope half-life (13 h vs. 8 d). Thus, there is reduced dosimetry that allows for the administration of higher activity. 123I-MIBG allows more convenient SPECT imaging, which is more sensitive than planar imaging. The 3-dimensional SPECT data can be fused with CT images for anatomic correlation, which is now quite simply obtained on hybrid SPECT/CT instruments. However, 123I is more expensive than 131I, has to be synthesized shortly before administration, and is not commercially available in all countries. Normal adrenal medulla is visualized with 131I-MIBG in about 10% of cases and with 123I-MIBG in 50%–80% of cases, and this physiologic uptake might obscure small lesions. In the MEN2 patients, with propensity for bilateral pheochromocytoma, such physiologic uptake may be a critical problem in the initial workup of patients or during follow-up after adrenal-sparing surgery. Overall, the sensitivity of MIBG imaging is lower in extraadrenal paragangliomas, metastatic paragangliomas, and recurrences.
Scanning with 111In-DTPA-pentetreotide is usually performed at 4 and 24 h after tracer injection. Imaging may need to be repeated later. The sensitivity of SST scintigraphy with 111In-DTPA-pentetreotide is lower than that of 131I/123I-MIBG in pheochromocytomas and sympathetic paragangliomas (24–26). The sensitivity of 111In-DTPA-pentetreotide is also inferior to MIBG in metastatic paragangliomas, even though 111In-DTPA-pentetreotide can provide additional information in some patients with rapidly progressing metastatic paraganglioma (24–27). However, considering parasympathetic paragangliomas, several studies have demonstrated the superiority of 111In-DTPA-pentetreotide scintigraphy over 131I/123I-MIBG, with sensitivities of 89%–100% and 18%–50%, respectively (28–33). SPECT with 111In-DTPA-pentetreotide is the current scintigraphy modality of reference in HNPs. However, its sensitivity needs to be revised downward in patients with hereditary syndromes because some additional lesions can be at the millimeter stage and not detectable by conventional scintigraphy (34).
Conventional 123I-MIBG SPECT and 111In-DTPA-pentetreotide SPECT are well-established nuclear imaging modalities in the staging and restaging of paragangliomas. Also, in recent years, SPECT/CT has become more widely available and has the advantage of simultaneous acquisition of both morphologic and functional data, increasing diagnostic confidence in image interpretation and enhancing sensitivity in some cases. However, these examinations are associated with practical constraints such as long imaging times, thyroid blockage and need for withdrawal of interfering medications (for MIBG scintigraphy), and gastrointestinal tract artifacts requiring bowel cleansing in some cases. The main disadvantage is probably the still-low resolution of the SPECT image, which is prone to artifacts and attenuation, limiting the ability to detect tiny lesions. SPECT also does not provide a quantifiable estimate of tumor metabolism (tracer uptake). Thus, PET has been growing rapidly in the imaging of paragangliomas, paralleled by great efforts toward the development of new tracers.
PET IMAGING AND METABOLIC PHENOTYPES
The sensitivity and resolution of PET are superior to those of SPECT scintigraphy (the current theoretic resolution of PET on phantoms is 4–5 mm, and in true clinical settings the resolution is close to 7–10 mm). PET is also a quantitative imaging technique. Most commonly, the standardized uptake value (SUV) is used to estimate the degree of tracer concentration in a defined region. In cases of small lesions, the partial-volume phenomenon affects images both qualitatively and quantitatively, underestimating the SUV and sometimes missing such lesions. However, detection of subcentimetric lesions remains possible in cases of high tracer avidity with a favorable signal-to-noise ratio, as is frequently observed with the specific tracers used to investigate paragangliomas.
PET is a cornerstone in the evaluation of paragangliomas. The broad diversity of PET biomarkers enables assessment of different metabolic pathways that appear to be determined largely by the underlying genotypes and related tumor cell characteristics. 18F-FDG is the most accessible tracer and plays an increasingly important role in paraganglioma imaging. 6-18F-fluoro-l-dopa (18F-FDOPA) is also available from different pharmaceutical suppliers. Other tracers, such as 18F-fluorodopamine (18F-FDA), 11C-hydroxyephedrine (11C-HED), and 68Ga-labeled peptides, are still in the evaluation stage and are used in the setting of clinical trials, though 68Ga-peptides are currently used in many centers for clinical purposes.
Glucose Metabolism Phenotype
18F-FDG uptake reflects glucose uptake and, indirectly, energy metabolism. 18F-FDG is taken up by tumor cells via glucose membrane transporters (mainly GLUT-1 and GLUT-3) and are phosphorylated by hexokinase into 18F-FDG-6P (Fig. 1). Because increased uptake of 18F-FDG is not specific to paragangliomas and because the first clinical results were disappointing (35,36), its use for this indication was delayed. Yet, as explained later, most paragangliomas are avid for 18F-FDG despite their relative indolence. This finding contrasts with the observation that other endocrine tumors (i.e., follicle-derived thyroid carcinoma, medullary thyroid carcinomas, and endocrine tumors of the digestive tract) generally exhibit a 2-phase metabolic profile: an initially low or absent 18F-FDG uptake that increases in the later stages of the disease (37,38).

Schematic display of mechanisms of uptake and retention of some PET tracers in tumor cells of neural crest origin. LAT1 requires dimerization with CD98 for targeting to plasma membrane. HK = hexokinase; AADC = aromatic L-amino decarboxylase.
Catecholaminergic Phenotype
11C-HED and 18F-FDA illustrate the properties of uptake and storage of catecholamines (chromaffin-derived cells) and were first developed to investigate the sympathetic innervation of the myocardium. Their storage in cytoplasmic vesicles requires the expression of vesicular monamine transporters (VMAT-1 and VMAT-2) (Fig. 1). 11C-HED PET was first evaluated in paragangliomas by Shulkin et al. from the University of Michigan (39). 11C-HED is captured by tumor cells via NET (Fig. 1) and has the same reuptake and storage characteristics as norepinephrine but is resistant to the action of both catechol-O-methyltransferase and monoamine oxidase enzymes. 11C-HED has shown excellent sensitivity for paragangliomas. However, its synthesis is complex, and the short half-life of 11C (20 min) requires an on-site cyclotron, a major drawback for routine clinical use.
18F-FDA has been developed as an alternative to 11C-HED PET. Its synthesis has been standardized at the National Institutes of Health, and it is currently used as an experimental tracer at the National Institutes of Health (40). Dopamine is a catecholamine precursor. In vitro, 18F-FDA has not demonstrated any difference from dopamine concerning its membrane transport by NET. After cellular uptake, 18F-FDA is stored in intracellular vesicles. NET and VMATs are strongly expressed in pheochromocytomas and paragangliomas (Fig. 1). Furthermore, dopamine can also potentially bind to specific receptors expressed in paragangliomas, in particular D2 receptors (41).
Amine Precursor Uptake and Decarboxylation Phenotype
In addition to expressing NET, paragangliomas can also decarboxylate amino acids such as dihydroxyphenylalanine. This property, common to tumors in the amine precursor uptake and decarboxylation system, depends on an enzyme that catalyzes the limiting step in the synthesis of catecholamines and of serotonin: aromatic amino acid decarboxylase. Dihydroxyphenylalanine is the precursor of all endogenous catecholamines. Dihydroxyphenylalanine is taken up through the sodium-independent large neutral amino acid transporter type 1 (LAT1). Membrane localization of this transporter requires heterodimerization with CD98, the heavy chain of 4F2 cell surface antigen (Fig. 1).
18F-FDOPA was initially developed to investigate dopaminergic neurotransmission. Hoegerle et al. were the first to demonstrate the utility of 18F-FDOPA PET to evaluate paraganglioma (42). 18F-FDOPA binds to LAT1 with high affinity and is converted into 18F-FDA by cytosolic aromatic amino acid decarboxylase. Since 18F-FDOPA is quickly converted into 18F-dopamine in the proximal renal tubule and eliminated in the urine, premedication with carbidopa (an aromatic amino acid decarboxylase inhibitor) is used by some authors to improve bioavailability of the tracer (43). 18F-FDOPA is available from different suppliers in the setting of the marketing authorization.
SST Expression Phenotype
Expression of SST has been demonstrated in paragangliomas by different techniques. SST2 is the most prevalent subtype in paragangliomas. SST1 is also strongly expressed in some paragangliomas, whereas other receptor subtypes are expressed there only slightly or not at all. The low expression of SST5 observed in paragangliomas constitutes a major difference from some endocrine tumors of the gastrointestinal tract. Based on experience with conventional scintigraphy using 111In-radiolabeled pentetreotide, PET using 68Ga-labeled somatostatin agonists has been evaluated in endocrine tumors with promising results. Tracer binding and retention depend on the density of SSTs on the cell surface and the degree of internalization of the ligand–receptor complex (Fig. 1). All radiolabeled agonists can target SST2 effectively, which is the SST most overexpressed in paragangliomas. Targeting of SSTs with PET tracers is obtained with DOTA-coupled somatostatin agonists (SSTa) labeled with 68Ga. Currently, 3 DOTA-coupled peptides—DOTATOC (Tyr3-octreotide), DOTATATE (Tyr3-octreotate), and DOTANOC (Nal3-octreotide)—have excellent affinity for SST2 receptors (50% inhibitory concentration: 2.5, 0.2, and 1.9 nM, respectively). DOTANOC also binds specifically to SST3, SST4, and SST5 receptors (44–46).
CLINICAL RESULTS OF PET
Normal Versus Tumoral Adrenal Tracer Uptake
The problem of normal uptake in the adrenal medulla potentially arises with all PET tracers but occurs mainly with 11C-HED (47,48), 18F-FDA (49), and 68Ga-DOTA-somatostatin agonists. It has been recommended that adrenal maximal SUV be measured to differentiate normal uptake from pathologic uptake (49). However, there is some overlap, and the proposed thresholds might be difficult to apply in clinical practice.
The utility of 18F-FDOPA is its low physiologic uptake in healthy adrenal glands (50). As regards 18F-FDG, the level of physiologic uptake in normal glands does not raise major diagnostic problems (51). Increased physiologic 18F-FDG uptake in the remaining adrenal gland may nevertheless occur after unilateral adrenalectomy for primary adrenocortical carcinoma but has not been reported for pheochromocytoma (52).
Apparently Sporadic Pheochromocytomas
There is no clear advantage of PET tracers over 123I-MIBG SPECT in these clinical situations (53). 123I-MIBG scintigraphy is sufficient to confirm the diagnosis of apparently sporadic pheochromocytoma even in rare cases of nonhypersecreting pheochromocytoma. No correlation exists between test sensitivity and secretory levels of tumors. With its whole-body screening, 123I-MIBG can rule out extraadrenal disease and guide subsequent CT and MRI investigations. Its negativity should lead to consideration of interference but can also be due to low expression of VMAT-1 (54). If MIBG is negative, and diagnostic presumption of pheochromocytoma is high, any of the specific PET tracers discussed earlier (18F-FDOPA (42,50,54–59), 18F-FDA (40,60), or 11C-HED (39,47,61)) can be attempted, with a sensitivity approaching 100% with modern PET/CT cameras. 18F-FDOPA PET and 18F-FDG PET can be performed without the need to withdraw drugs that interfere with MIBG. 18F-FDG PET is a highly sensitive modality in paragangliomas, even in cases of pheochromocytoma with low proliferative index and no mitosis. In the case of a high adrenal 18F-FDG uptake (tumor-to-liver maximal SUV ratio > 2), 4 main potential differential diagnoses should be considered: pheochromocytoma, malignant adrenal cortex tumor, primary lymphoma, and metastasis. Some features that may orientate toward pheochromocytoma are solitary lesion without vena cava involvement, decreased uptake in the central area of the tumor evidencing cystic or hemorrhagic alterations, and calcifications visible on the CT scan. Increased 18F-FDG uptake in brown adipose tissue, due to stimulation by circulating norepinephrine, should not be confused with extraadrenal lesions; such uptake can be visualized in about 20% of patients (62).
MEN2-Related Pheochromocytomas
A special advantage of 18F-FDOPA PET over MIBG and other specific PET tracers is the lack of significant uptake in normal adrenal glands. This is particularly important in MEN2 patients for differentiating normal or hyperplastic adrenal glands from those that are tumoral. Luster et al. made a retrospective evaluation of 25 patients (including 12 with MEN2) with 18F-FDOPA PET/CT (50). Overall sensitivity and specificity in detecting pheochromocytoma were 100% and 89%. A combination of 18F-FDOPA PET/CT and CT/MRI was found to be the optimal imaging strategy in another study (56). 18F-FDOPA PET has also been used to identify metastases from medullary thyroid carcinomas in MEN2 patients (50).
Extraadrenal Retroperitoneal Paragangliomas
In the case of a retroperitonal extraadrenal nonrenal mass, imaging should differentiate a paraganglioma from a neurogenic tumor, lymph node disease, or a mesenchymal tumor. Despite the high performance of conventional imaging, the diagnosis may remain uncertain. A biopsy is not always contributive and can carry risks. Therefore, the specificity of functional imaging provides an important contribution. Once the diagnosis of paraganglioma has been established, multiplicity of extraadrenal localizations should be considered.
MIBG is clearly superior to SST scintigraphy (24) in abdominal paraganglioma but may be suboptimal in cases of small lesions or those with special phenotypic aspects, such as VHL-related paragangliomas (42,63). Studies that have included a high number of extraadrenal, multiple, or hereditary paragangliomas found reduced sensitivity for MIBG (52%–75%) (24,53,56,60). Furthermore, MIBG may miss additional HNPs in hereditary syndromes. 18F-FDOPA PET was found to be more sensitive than MIBG scintigraphy in the staging and restaging of paragangliomas (42,50,54–59). In some studies, 18F-FDOPA PET significantly detected more lesions than CT/MRI. Reported sensitivities range from 81% to 100%. However, 18F-FDOPA PET should not be considered similar to MIBG scanning with higher sensitivity but is rather a new specific radiotracer with its own advantages and limitations. The main limitation relates to patients with SDHx mutations. In a prospective study by Fottner et al., all sympathetic paragangliomas associated with SDH mutations were positive with 123I-MIBG, whereas 2 extraadrenal paragangliomas were not detected with 18F-FDOPA PET despite the centimeter size of the lesions (54). This possibility of missing certain retroperitoneal tumors has also been noted in 3 other studies (34,53,56). 18F-FDA PET is highly sensitive but may also miss some tumors (24,60).
Taïeb et al. showed that 18F-FDG PET positivity was not indicative of malignancy or histologic dedifferentiation in paraganglioma but rather was related to genetic status (64). In that study, SDHx and VHL-related tumors were notable in being the most 18F-FDG–avid tumors. 18F-FDG PET appears especially sensitive in detecting sympathetic extraadrenal paragangliomas, probably as a result of the higher prevalence of SDHB mutations in this setting.
The new PET tracers targeting SST receptors are now under evaluation in paragangliomas, and published data are limited to case reports (65–69) and small series (70). 68Ga DOTATOC and 68Ga-DOTATATE PET/CT were found to be superior to 123I-MIBG SPECT in some cases of aggressive paraganglioma, probably associated with a certain level of functional dedifferentiation.
Metastatic Paragangliomas/Pheochromocytomas
Imaging work-up might entail the use of more than 1 tracer. MIBG scintigraphy has been compared with 11C-HED (39,48,61,71), 18F-FDA (24,60,72), 18F-FDOPA (54,56,57,73), and 68Ga-DOTA-TOC (74) and has been considered inferior to these PET tracers in most studies. The sensitivity of MIBG scintigraphy in terms of detected lesions is about 65%. Thus, 123I-MIBG SPECT may lead to significant underestimation of the disease, with potential inappropriate management in apparently oligometastatic disease.
The presence of SDHB mutation markedly impacts on the choice of tracers (53,75). In a prospective study by Timmers et al. (53), 28 patients had metastatic paragangliomas: 13 pheochromocytomas (3 SDHB, 1 SDHD, 1 VHL, 1 MEN2, and 7 sporadic) and 15 extraadrenal paragangliomas (12 SDHB, 1 SDHD, and 2 sporadic). These patients were imaged with different tracers. In reference to CT/MRI, overall sensitivities for 123I-MIBG SPECT, 18F-FDG PET/CT, 18F-FDOPA PET, and 18F-FDA PET/CT were, respectively, 57%, 74%, 45%, and 76%. On per-patient analysis, 18F-FDG PET was more frequently contributive in SDHB-positive patients, whereas 18F-FDOPA PET was more frequently contributive in SDHB-negative patients. The percentage of sites detected was 57% with 123I-MIBG (57% for SDHB-positive vs. 59% SDHB-negative, not statistically significant), 74% for 18F-FDG PET (83% SDHB-positive vs. 62% SDHB-negative, P < 0.001), 45% for 18F-FDOPA PET (20% SDHB-positive vs. 93% SDHB-negative, P < 0.001), and 76% for 18F-FDA PET (82% SDHB-positive vs. 93% SDHB-negative, P = 0.037). This study demonstrated the phenotypic heterogeneity of tumors in imaging studies and the need to combine functional imaging modalities. The main limitation of the study is that 18F-FDOPA, in contrast to the other tracers, has been evaluated using PET alone and not with a modern hybrid PET/CT camera, which might have decreased the value of the technique. To date, 18F-FDOPA PET may be the imaging modality of choice in the absence of SDHB mutation or when genetic status is unknown (Fig. 2). 18F-FDG PET is considered the imaging modality of reference for SDHB-positive paraganglioma cases (Fig. 3; Table 1). When more widely available, 18F-FDA PET will possibly be used as a first-line diagnostic imaging modality in patients with a metastatic pheochromocytoma, whatever their genetic status (53,75,76). It might be too early to abandon 123I-MIBG scintigraphy, as it may offer additional information in some patients. Furthermore, 123I-MIBG scintigraphy remains an important modality to determine whether a patient is eligible for treatment with 131I-MIBG. Bone scintigraphy is also useful in SDHB-positive patients (75).
Clinical Features and Suggestions for Imaging Work-up in Paraganglioma Syndromes
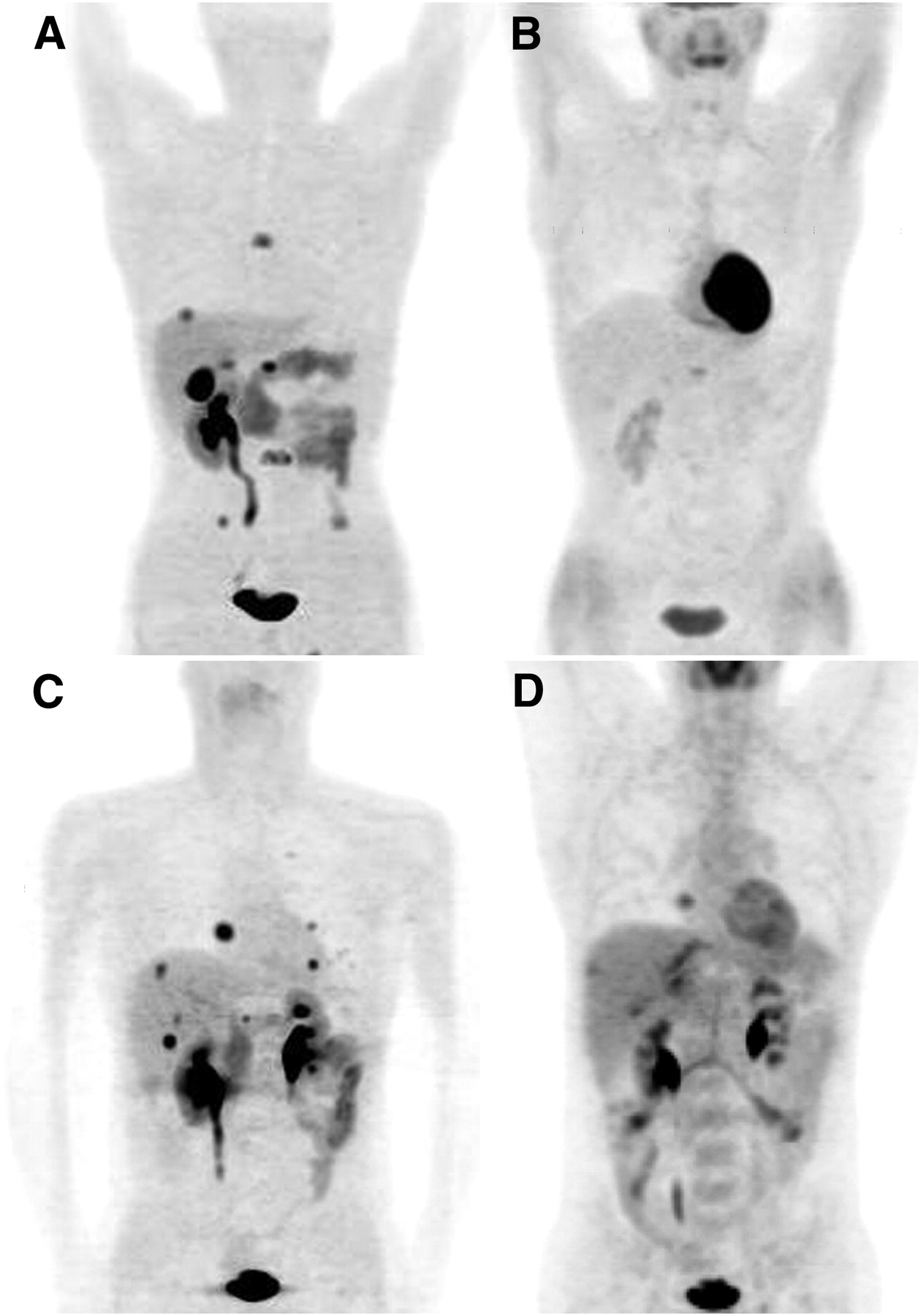
Comparison between maximal-intensity-projection 18F-FDOPA and 18F-FDG PET images in restaging of 2 patients with metastatic paraganglioma without SDHB mutation. (A and B) A 34-y-old man with persistent biochemical abnormalities after resectioning of multiple abdominal paragangliomas. Postoperative 18F-FDOPA PET found 2 liver metastases and thoracic and lumbar spine metastases (T6, T12, and L3; maximal SUV, 9.9), as well as osteolytic lesion of right iliac bone. Physiologic uptake is seen in kidneys, pancreas, gallbladder, and digestive tract (via bile elimination) (A). 18F-FDG PET depicted only 1 metastasis (T12; maximal SUV, 2.1) (B). (C and D) A 43-y-old man with biochemical persistence after resection of large pheochromocytoma and liver metastases. Postoperative 18F-FDOPA PET shows multiple liver and lung metastases (C). 18F-FDG PET underestimated number of foci; visible lesions have lower SUVs (D)
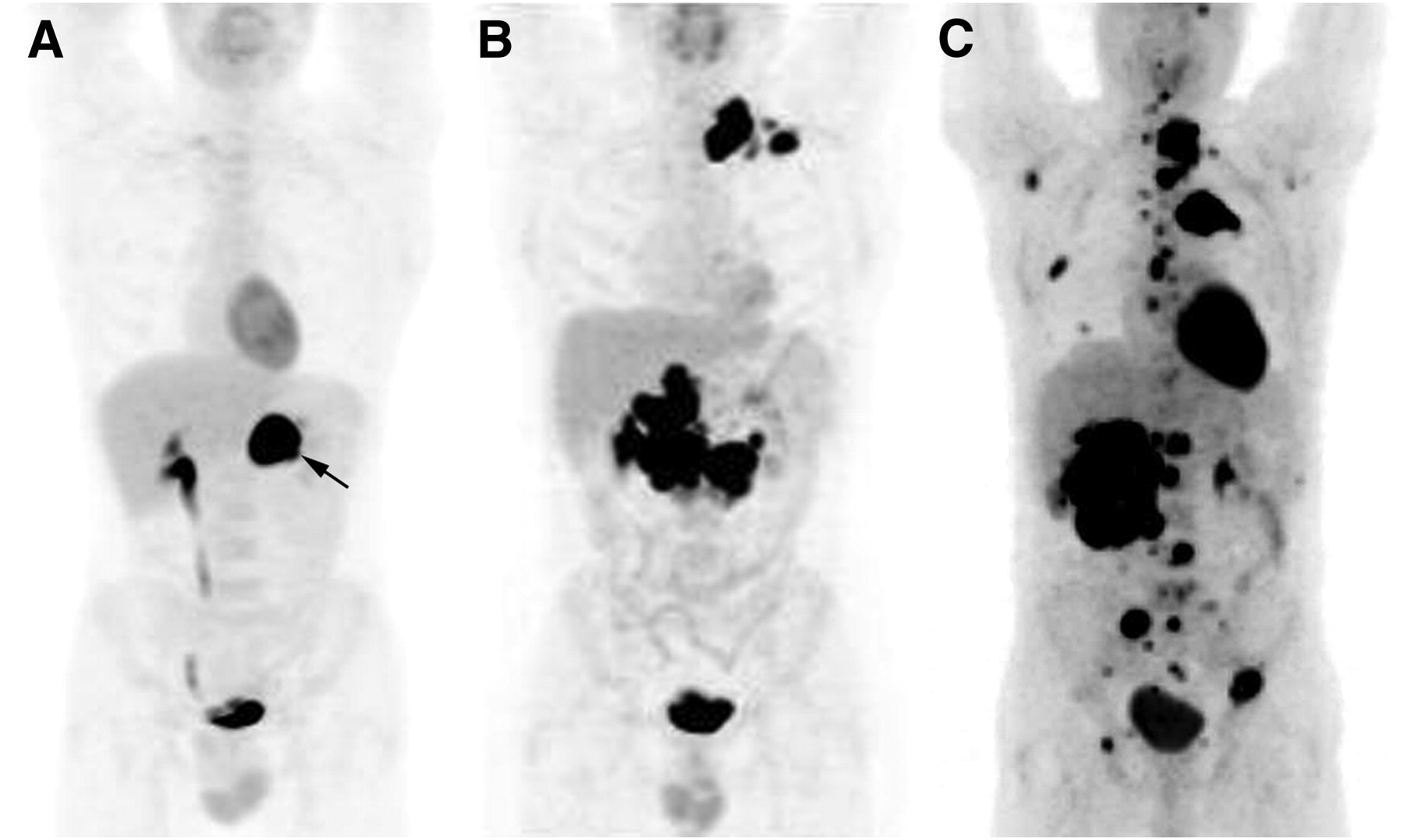
Maximal-intensity-projection 18F-FDG PET images of SDHB-related paraganglioma. (A) A 38-y-old man presenting with hypertensive crises. 18F-FDG PET depicted left adrenal tumor with marked avidity (maximal SUV, 49) and no extraadrenal foci. Pathologic examination found a 33-mm pheochromocytoma without unfavorable histologic features (PHEO of Adrenal Scaled Score [PASS] = 0, Ki-67 < 1%). (B) A 41-y-old man with multiple abdominal paragangliomas and left metastatic supraclavicular lymph nodes. (C) A 36-y-old man with large pheochromocytoma and extensive bone metastases (spine, ribs, skull base, and hip).
Data with 68Ga-labeled agonists are still limited. 68Ga PET was found to be sensitive in the detection of rapidly progressing metastatic paraganglioma (Fig. 4) (65,67,74,77). 68Ga-DOTA-SSTa should also give valuable information on tumor cell receptor status for the planning of peptide receptor radionuclide therapy (78).
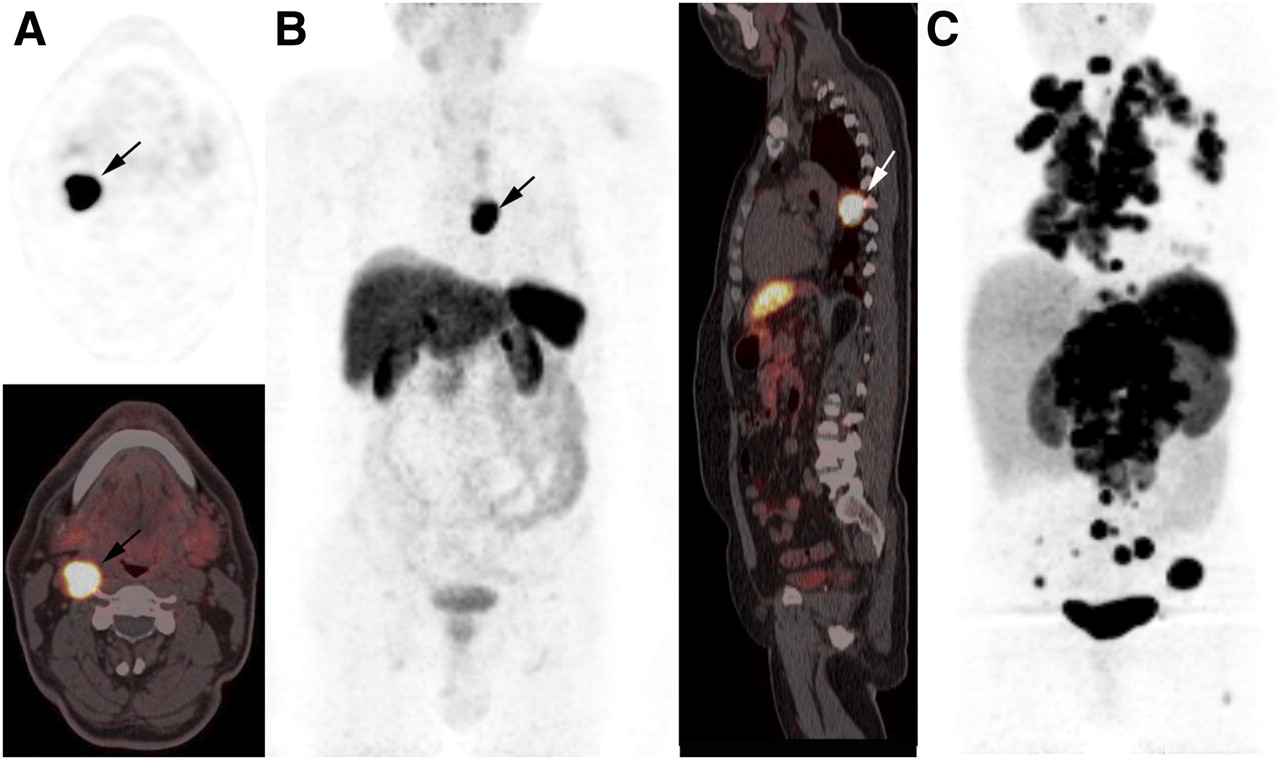
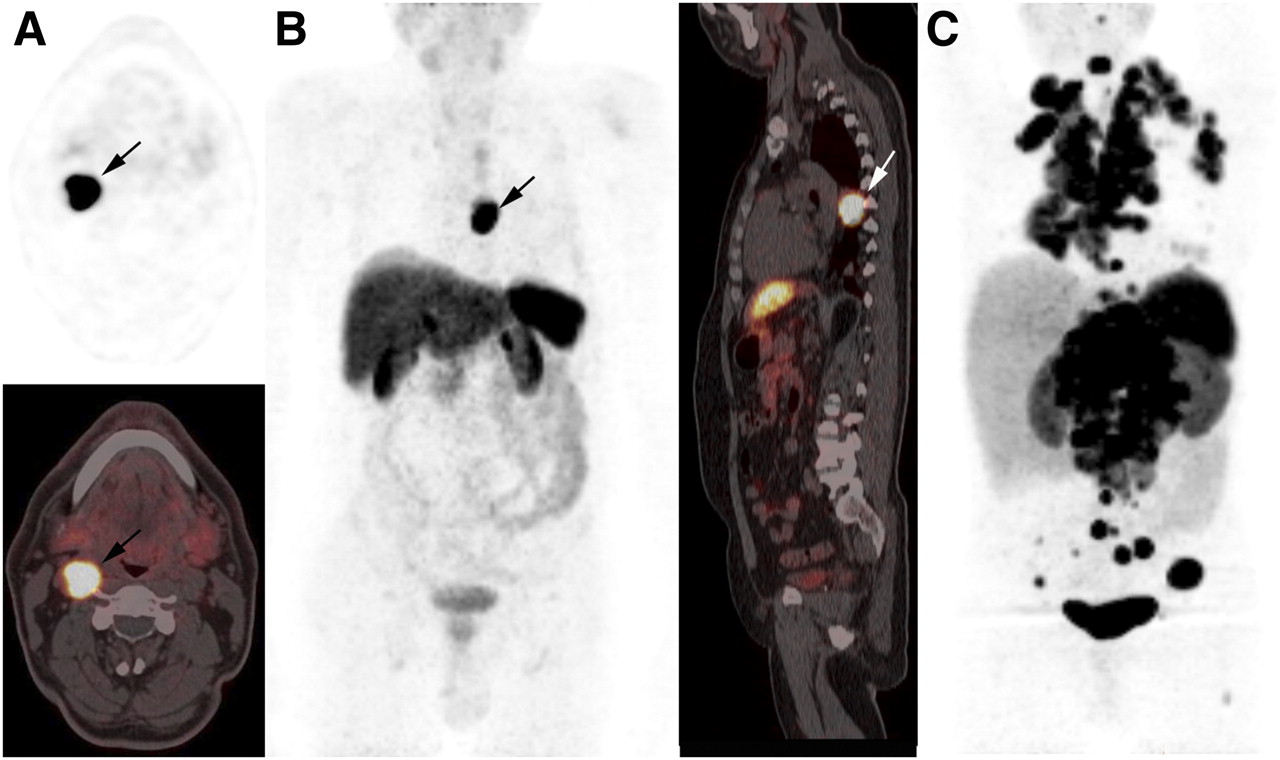
68Ga-DOTATATE findings in 3 different paraganglioma patients. (A) Right carotid glomus paraganglioma (top: axial PET image; bottom: axial PET/CT fusion image). (B) Thoracic sympathetic paraganglioma (left: maximal-intensity-projection image; right: sagittal PET/CT fusion image). (C) Metastatic paraganglioma with multiple lymph nodes and metastases in lungs and bones (maximal-intensity-projection image).
HNPs
HNPs raise the problem of locoregional extension and multifocality. Metastatic forms are rare.
The results of PET in HNPs have rarely been addressed in isolation (34,53,54,56,65,66,68,79–81). Hoegerle et al. have compared 18F-FDOPA PET/CT and MRI in 10 patients (79). All paragangliomas were visualized with 18F-FDOPA PET, whereas 1 tiny lesion remained occult on MRI even after correlation with PET results. This study demonstrates that HNPs are highly avid for 18F-FDOPA and that favorable signal-to-noise uptake ratios enable the detection of subcentimetric tumors.
These results are in line with those obtained by Charrier et al., who found a sensitivity of 97% for 18F-FDOPA PET/CT versus 67% for SST scintigraphy (34). This lower sensitivity of SST scintigraphy probably is related to the limited resolution of SPECT. King et al. also reported results widely in favor of 18F-FDOPA PET/CT in the localization of SDHx-related HNPs (sensitivity, 100%), followed by CT/MRI (81%), 18F-FDG PET (77%), SST scintigraphy (64%), and 18F-FDA PET (46%) (80).
Taken together, these studies show that 18F-FDOPA PET/CT appears to be an excellent first-line imaging tool in HNPs (Fig. 5; Table 1). 18F-FDOPA PET might miss extraadrenal retroperitoneal paraganglioma, which can potentially coexist with HNPs (34,53,54,56). This leading position for 18F-FDOPA PET/CT may of course further evolve if a future head-to-head comparison of 18F-FDOPA PET and 68Ga-SSTa PET is achieved. Preliminary results for 68Ga-labeled DOTA peptides are encouraging (Fig. 4) (65,66,68).
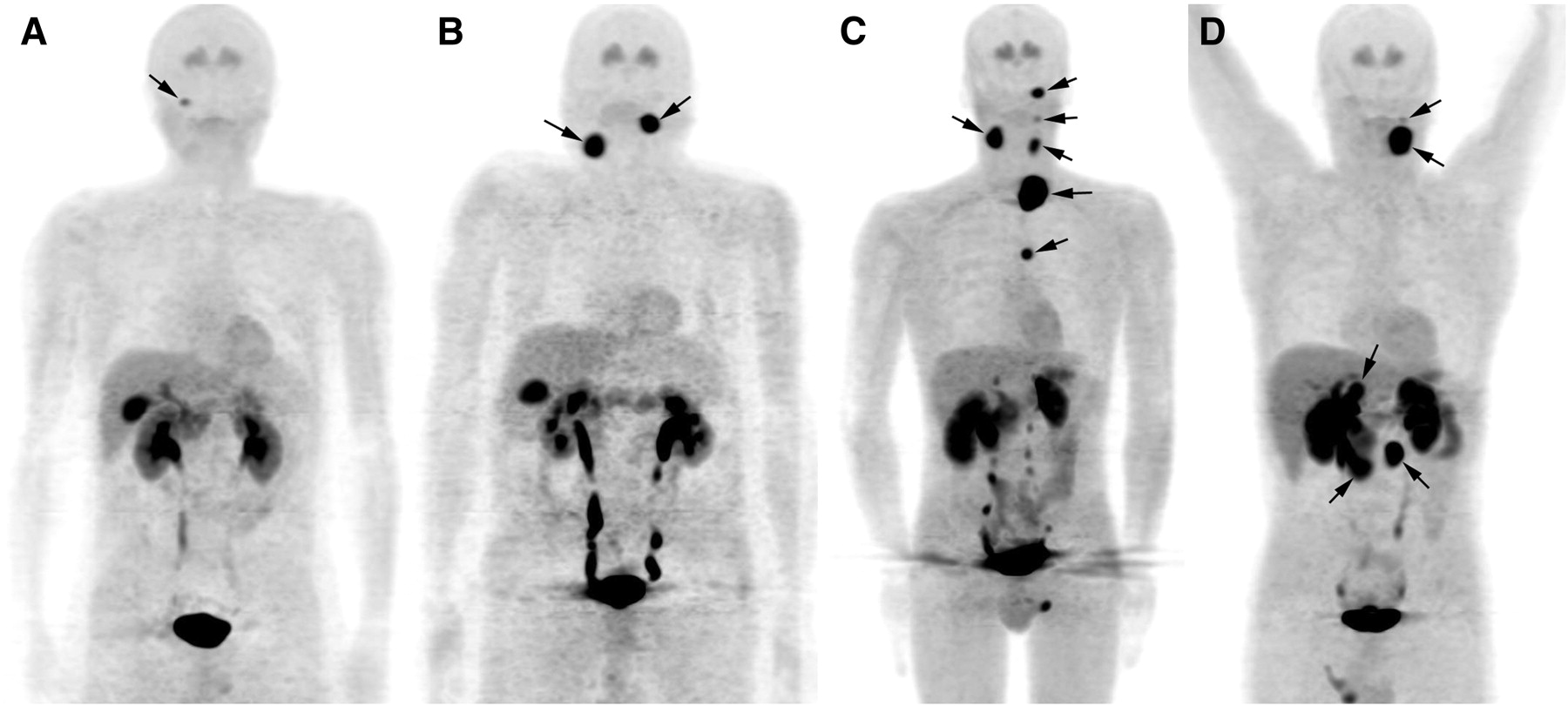
Maximal-intensity-projection 18F-FDOPA PET images of SDHx-related HNPs. (A) SDHB: A 57-y-old man who previously underwent surgery for left large carotid glomus paraganglioma associated with metastatic lymph nodes. Follow-up 18F-FDOPA PET found tiny right jugular paraganglioma. 18F-FDG PET was also positive. (B) SDHC: A 71-y-old man with bilateral incidentally discovered neck paragangliomas. (C) SDHD: A 47-y-old man with 6 asymptomatic parasympathetic 18F-FDOPA–avid paragangliomas. Two abdominal paragangliomas were missed by 18F-FDOPA PET. (D) SDHD: A 39-y-old man admitted to hospital for cardiogenic shock after use of β-blocker eye drops. Imaging work-up found 2 parasympathetic paragangliomas and 6 abdominal paragangliomas. 18F-FDOPA PET identified 2 HNPs and 3 abdominal paragangliomas (arrows) but failed to identify 3 additional abdominal tumoral sites that were identified by 18F-FDG PET.
GENOTYPE-IMAGE PHENOTYPE
Despite the rapid and important progress achieved since the discovery of the first SDHD gene mutation a decade ago, the tumorigenesis pathways remain to be determined. Many of the predominant mutations observed in paraganglioma also control tumor cell metabolism (82–84). There is, for example, growing evidence that suggests a link between increased 18F-FDG uptake in some of the genetic mutations and activation of hypoxia signaling in tumor cells.
SDHB-mutated paragangliomas are notable in being the most 18F-FDG–avid tumors (64). It has been suggested that SDH and VHL-mutated tumors may have a genetically driven Warburg effect (aerobic glycolysis) (82).
In normoxia, HIF-α isoforms are rapidly ubiquitinylated and targeted for proteasomal degradation. The oxygen-sensitive signal is generated by prolyl hydroxylases that catalyze hydroxylation of HIF-α isoforms. Prolyl hydroxylation targets the proteins for proteasomal degradation by promoting their interaction with VHL, a component of an E3 multiprotein ubiquitin–ligase complex.
Under hypoxic conditions, prolyl hydroxylase activity decreases, prolyl hydroxylation rate slows, and proteasomal degradation rate of HIF slows, leading to stabilization of HIF-α isoforms and activation of genes involved in response to hypoxia. Hypoxia-induced changes in gene expression extend to several hundred transcripts, including glucose transporters, glycolytic enzymes, angiogenic factors, and erythropoietin.
SDH or VHL inactivation induces a hypoxic response in the presence of oxygen, called a pseudohypoxia state. VHL mutations may disrupt VHL–HIF interaction, leading to HIF accumulation even in the presence of oxygen. SDH inactivation, on the other hand, may impair HIF hydroxylation through increased production of succinate or reactive oxygen species (85–88). As a result, glucose uptake is increased, which can be visualized with 18F-FDG PET. Consistent with this idea, HIF-1α and its downstream targets were found to be upregulated in SDHx and VHL-related tumors (89). Transcriptional profiling studies also revealed pseudohypoxic signatures in SDHx/VHL tumors that can differentiate them from RET/NF1 cases that usually have lower 18F-FDG avidity (90–92). However, even if both VHL and SDHB/D inactivations may disrupt the HIF-dependent pathway, the transcriptional targets that mediate the changes may well be different. It has been found that HIF-1α target genes were activated predominantly in the VHL pheochromocytomas (90–92). Taken together, these results suggest that inactivation of VHL and SDHx genes can upregulate specific HIF downstream targets and promote tumor growth, angiogenesis, metastasis, as well as 18F-FDG uptake (93). However, further investigation is required to understand the sequence of events involved for a specific mutation. In the meantime, it is important to recognize that other potential key signaling pathways may regulate 18F-FDG uptake and require further basic research.
Mutations in susceptibility genes also influence secretory profiles and imaging phenotypes of paraganglioma. These sets of genes are possibly essential in the control of key proteins involved in the catecholamine secretory pathway. It is notable that SDHB tumors may weakly concentrate 18F-FDOPA. 18F-FDOPA PET may miss abdominal paragangliomas in patients with SDHx mutations (34,54), and false-negative MIBG findings have also been reported in VHL tumors. The relationship between determinants of cellular uptake, synthesis or secretion machinery, and germline mutations requires further evaluation.
CONCLUSION
These new findings open a range of possible insights into the association of genotype and image phenotype that could guide clinicians in better tailoring paraganglioma-imaging modalities.
Acknowledgments
We thank Dr. Henri Timmers for his helpful comments and thoughtful suggestions.
Footnotes
↵* Contributed equally to this work.
Learning Objectives: On successful completion of this activity, participants should be able to describe (1) the best nuclear imaging procedures to detect pheochromocytomas/paragangliomas according to the clinical situation (e.g., sporadic vs. hereditary; primary vs. metastatic; sympathetic vs. parasympathetic) and (2) the differences in the phenotypic information obtained by various PET tracers.
Financial Disclosure: The authors of this article have indicated no relevant relationships that could be perceived as a real or apparent conflict of interest.
CME Credit: SNM is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to sponsor continuing education for physicians. SNM designates each JNM continuing education article for a maximum of 1.0 AMA PRA Category 1 Credit. Physicians should claim only credit commensurate with the extent of their participation in the activity.
For CE credit, participants can access this activity through the SNM Web site (http://www.snm.org/ce_online) through February 2013.
- © 2012 by the Society of Nuclear Medicine, Inc.
REFERENCES
- 1.↵
- 2.
- 3.
- 4.
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.
- 26.↵
- 27.↵
- 28.↵
- 29.
- 30.
- 31.
- 32.
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.
- 56.↵
- 57.↵
- 58.
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.
- 84.↵
- 85.↵
- 86.
- 87.
- 88.↵
- 89.↵
- 90.↵
- 91.
- 92.↵
- 93.↵
- Received for publication September 8, 2011.
- Accepted for publication December 27, 2011.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Nuclear Imaging of a Cardiac Paraganglioma
- Functioning metastatic paraganglioma of the urinary bladder in a 10-year-old child
- Clinical Value of 18F-fluorodihydroxyphenylalanine Positron Emission Tomography/Contrast-enhanced Computed Tomography (18F-DOPA PET/CT) in Patients with Suspected Paraganglioma
- Superiority of [68Ga]-DOTATATE PET/CT to Other Functional Imaging Modalities in the Localization of SDHB-Associated Metastatic Pheochromocytoma and Paraganglioma
- Semiquantitative 123I-Metaiodobenzylguanidine Scintigraphy to Distinguish Pheochromocytoma and Paraganglioma from Physiologic Adrenal Uptake and Its Correlation with Genotype-Dependent Expression of Catecholamine Transporters
- Targeting Neuropeptide Receptors for Cancer Imaging and Therapy: Perspectives with Bombesin, Neurotensin, and Neuropeptide-Y Receptors
- 68Ga-DOTANOC PET/CT for Baseline Evaluation of Patients with Head and Neck Paraganglioma