


Abstract
Several studies outlined the sensitivity of 68Ga-labeled PET tracers against the prostate-specific membrane antigen (PSMA) for localization of relapsed prostate cancer in patients with renewed increase in the prostate-specific antigen (PSA), commonly referred to as biochemical recurrence. Labeling of PSMA tracers with 18F offers numerous advantages, including improved image resolution, longer half-life, and increased production yields. The aim of this study was to assess the PSA-stratified performance of the 18F-labeled PSMA tracer 18F-DCFPyL and the 68Ga-labeled reference 68Ga-PSMA-HBED-CC. Methods: We examined 191 consecutive patients with biochemical recurrence according to standard acquisition protocols using 18F-DCFPyL (n = 62, 269.8 MBq, PET scan at 120 min after injection) or 68Ga-PSMA-HBED-CC (n = 129, 158.9 MBq, 60 min after injection). We determined PSA-stratified sensitivity rates for both tracers and corrected our calculations for Gleason scores using iterative matched-pair analyses. As an orthogonal validation, we directly compared tracer distribution patterns in a separate cohort of 25 patients, sequentially examined with both tracers. Results: After prostatectomy (n = 106), the sensitivity of both tracers was significantly associated with absolute PSA levels (P = 4.3 × 10−3). Sensitivity increased abruptly, when PSA values exceeded 0.5 μg/L (P = 2.4 × 10−5). For a PSA less than 3.5 μg/L, most relapses were diagnosed at a still limited stage (P = 3.4 × 10−6). For a PSA of 0.5–3.5 μg/L, PSA-stratified sensitivity was 88% (15/17) for 18F-DCFPyL and 66% (23/35) for 68Ga-PSMA-HBED-CC. This significant difference was preserved in the Gleason-matched-pair analysis. Outside of this range, sensitivity was comparably low (PSA < 0.5 μg/L) or high (PSA > 3.5 μg/L). After radiotherapy (n = 85), tracer sensitivity was largely PSA-independent. In the 25 patients examined with both tracers, distribution patterns of 18F-DCFPyL and 68Ga-PSMA-HBED-CC were strongly comparable (P = 2.71 × 10−8). However, in 36% of the PSMA-positive patients we detected additional lesions on the 18F-DCFPyL scan (P = 3.7 × 10−2). Conclusion: Our data suggest that 18F-DCFPyL is noninferior to 68Ga-PSMA-HBED-CC, while offering the advantages of 18F labeling. Our results indicate that imaging with 18F-DCFPyL may even exhibit improved sensitivity in localizing relapsed tumors after prostatectomy for moderately increased PSA levels. Although the standard acquisition protocols, used for 18F-DCFPyL and 68Ga-PSMA-HBED-CC in this study, stipulate different activity doses and tracer uptake times after injection, our findings provide a promising rationale for validation of 18F-DCFPyL in future prospective trials.
After radical prostatectomy, concentrations of prostate-specific antigen (PSA) typically decrease below detection threshold. A renewed increase in PSA levels to above 0.2 μg/L, commonly referred to as biochemical recurrence (BCR), signifies a potential relapse of prostate cancer after surgery (1). Similarly, BCR is defined as a PSA increase of at least 2 μg/L above the minimum PSA level after radiotherapy. The prostate-specific membrane antigen (PSMA) is particularly overexpressed on the surface of prostate cancer cells (2). Tracers for PET, that bind specifically to PSMA, have gained increasing attention for localization of tumors in BCR patients (3–12). In particular, 68Ga-PSMA-HBED-CC displays substantial sensitivity in detecting tumor relapse after prostatectomy, even when PSA levels are low (≥0.2 μg/L) (3–9). Furthermore, 4 studies have consistently shown that approximately 95% of the 68Ga-PSMA-HBED-CC–positive lesions have histologic tumor correlates in biopsies and surgical resections (13–16).
The short half-life of 68Ga makes 68Ga-PSMA-HBED-CC inconvenient for longer transport, so that cost-intensive, local gallium generators are required, which typically have lower yields at the end of their first half-life (17). Furthermore, the resolution of 68Ga-labeled tracers is physically limited because of positron range effects (18). In contrast, 18F labels avoid these intrinsic difficulties and can be produced at high yields in central cyclotrons. In 2011, the first preclinical data with the 18F-labeled PSMA ligand DCFPyL were published (10). Recently, 2 proof-of-principle studies demonstrated the general capability of 18F-DCFPyL to detect relapsed tumors in 9 (11) and 14 BCR patients (12), respectively. Here, we examined 62 BCR patients with 18F-DCFPyL and benchmarked the PSA-stratified sensitivity of 18F-DCFPyL against 68Ga-PSMA-HBED-CC (n = 129 patients).
MATERIALS AND METHODS
Patients
We examined 191 consecutive prostate cancer patients with BCR after radical prostatectomy (n = 106) or radiotherapy (n = 85), either with 18F-DCFPyL (n = 62) or 68Ga-PSMA-HBED-CC (n = 129) (Table 1). Patients were selected according to the following criteria: for the prostatectomy cohort—complete removal of the entire prostate gland (R0 or R1 resection) and a recent PSA increase to 0.2 μg/L or more after nadir; and for the radiotherapy cohort—organ-preserving local treatment (external-beam radiation therapy, brachytherapy, seed implantation, high-intensity focused ultrasound) and a PSA increase of at least 2.0 μg/L above the minimum PSA value after therapy, as determined by the referring urologist.
Characteristics of Patients Examined in This Study
Additionally, we required that no distant metastases had been detected in previous examinations, that patients did not receive antiandrogen therapy, and a time period of at least 6 mo had elapsed between the initial therapy and the PET scan. Forty-seven of our prostatectomy patients received additional salvage radiotherapy before the PET scanning (16 18F-DCFPyL cases, 31 68Ga-PSMA-HBED-CC cases).
As an additional approach, we continued our efforts of a previous study (12) (n = 14 patients) and sequentially examined prostate cancer patients with 68Ga-PSMA-HBED-CC and 18F-DCFPyL. This allowed a direct comparison of the tracer distribution pattern within a separate validation cohort of 25 patients. Inclusion criteria for this validation cohort were described previously (12).
This study was conducted in accordance with the Institutional Review Board. All patients gave written informed consent to PET imaging and inclusion of their data in a retrospective analysis. All procedures were performed in compliance with the regulations of the responsible local authorities (District Administration of Cologne, Germany).
Imaging
PSMA PET tracers were synthesized as previously described for 18F-DCFPyL (10,12) and 68Ga-PSMA-HBED-CC (19,20). Each week, we produced 3 independent batches of 68Ga-PSMA-HBED-CC and 1 batch of 18F-DCFPyL. Patients were randomly assigned by tracer availability. Images were acquired on a Biograph mCT Flow (Siemens) PET/CT scanner. In accordance with standard acquisition protocols (3,5,7,12), patients fasted for at least 4 h before intravenous injection of 68Ga-PSMA-HBED-CC (158.9 ± 45.1 MBq) or 18F-DCFPyL (269.8 ± 81.8 MBq). PET images were acquired 1 or 2 h after injection, respectively. The same filters and acquisition times were used for both tracers. Non–contrast-enhanced (low-dose) CT scans were acquired in parallel to PET imaging. Images were reconstructed on the basis of the ultra-high definition algorithm (21).
PSMA PET scans were analyzed through visual inspection by at least 1 specialist in nuclear medicine and 1 specialist in radiology. A scan was scored as positive if focal tracer accumulation was detected in the prostate fossa, in a lymph node, or at a distant site. To be interpreted as a PET-positive lymph node, we required a morphologic correlate on the CT scan. A tumor relapse was interpreted as limited if tracer accumulation was limited to the prostate fossa or to locoregional lymph nodes. Otherwise, a positive scan was scored as advanced. Furthermore, we scored PET positivity based on the number of PET-positive lesions (score 0, negative scan; score 1, 1 lesion; score 2, 2 lesions; score 3, more than 2 positive lesions).
Confirmation of PET-Positive Lesions Through Biopsies
As an external validation of our imaging results, 15 BCR patients with PET-positive tissue within the prostate fossa underwent biopsy (4 18F-DCFPyL and 11 68Ga-PSMA-HBED-CC cases). For each patient, we obtained 12 local biopsies from the residual prostate gland (13 radiotherapy patients) or prostate fossa (2 prostatectomy patients), guided by ultrasound. We compared histology with tracer distribution and categorized the findings as follows: full concordance—all PSMA-positive segments histologically confirmed, all PSMA-negative segments tumor-free; partial concordance—all PSMA-positive segments histologically confirmed, but not all PSMA-negative segments tumor-free; false-positive cases—at least 1 PSMA-positive segment lacking histologic confirmation; and full discordance—PSMA-positive segments lacking histologic confirmation, PSMA-negative segments infiltrated by tumor cells.
Statistics and Mathematic Modeling
For PSA stratification, we systematically calculated tracer sensitivity within multiple small PSA ranges. Each PSA interval was characterized in terms of its center and width. On the basis of the detection rate within each interval, we compiled a PSA-stratified tracer sensitivity curve without any a priori assumption of PSA thresholds. Analogously, we derived curves displaying the PSA-stratified rate of diagnosis at limited stage based on multiple small PSA intervals. From these curves, we derived a diagnostic window as follows: the lower threshold was determined as the PSA level, where sensitivity exceeded 50%. The upper threshold was taken as the PSA level, where the fraction of limited relapses detected decreased 50%.
To correct our sensitivity comparison between 18F- and 68Ga-labeled tracers for Gleason scores, we randomly selected matched subcohorts of 30 18F and 30 68Ga tracer patients with pairwise equal Gleason scores (1,000 iterations). We then determined the log-transformed ratio between PSA-stratified sensitivity in the 18F subcohort and sensitivity in the 68Ga subcohort for each iteration. We thus obtained log-transformed ratios ri, with ri > 0, if 18F sensitivity was superior. Finally, we compared ri against the null hypothesis by a paired t test.
RESULTS
PSA Levels Predict Sensitivity of PSMA Imaging After Prostatectomy
We first subdivided the 191 consecutive PET scans into the following groups: PSMA-negative scans (n = 43), PSMA-positive scans displaying limited relapse (n = 85), and PSMA-positive scans displaying advanced relapse (n = 63).
In prostatectomy patients, PSA levels significantly differed between these 3 groups (Supplemental Fig. 1A; supplemental materials are available at http://jnm.snmjournals.org): PSA levels were significantly lower in PET-negative patients than in PET-positive patients displaying limited (P = 4.3 × 10−3) or advanced relapse (P = 4.9 × 10−7). Furthermore, PSA levels differed significantly between limited and advanced-staged relapses (P = 7.6 × 10−3). Interestingly, PSA values did not differ significantly after radiotherapy (Supplemental Fig. 1B). Intriguingly, PSMA accumulated exclusively in locoregional nodes for 75% of prostatectomy patients with limited relapse, which was rarely observed after radiotherapy (17%, P < 1 × 10−4). Most radiotherapy patients with limited relapse displayed tracer accumulation exclusively in the local tumor bed (68%), which was only occasionally detected after prostatectomy (21%, P < 1 × 10−4).
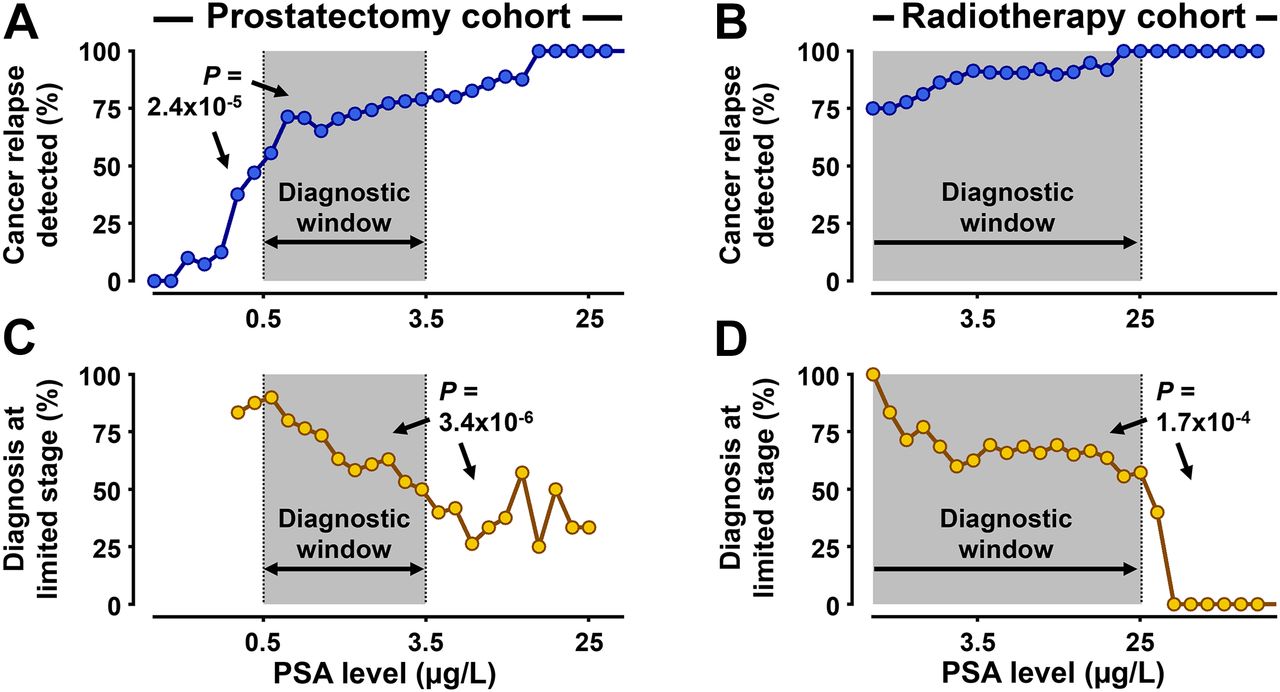
We next plotted PSA levels against the rate of PET-positive patients after prostatectomy. Furthermore, we plotted PSA against the fraction of scans, displaying a relapse at limited stage. Detection rates increased abruptly and significantly (P = 2.4 × 10−5), when PSA concentrations exceeded 0.5 μg/L and remained largely unchanged above this threshold (Fig. 1A). PSA levels tightly anticorrelated with the probability of detecting cancer relapse at limited stage (Fig. 1C): although most relapsed tumors were diagnosed at limited stage for a PSA of less than 3.5 μg/L, this pattern significantly (P = 3.4 × 10−6) reversed when PSA levels exceeded 3.5 μg/L. Interestingly, these rates were largely PSA-independent for PSA levels up to 25 μg/L in the radiotherapy cohort (Figs. 1B and 1D). Although sensitivity was high across all PSA concentrations examined (median, 91.5%), the fraction of limited-stage diagnoses varied stably around a median of 67.5% for PSA up to 25 μg/L.

PSA-based stratification reveals optimized PSA range for PET imaging. Patients were sorted by log-transformed PSA levels (x-axis) in ascending order. Fraction of PSMA-positive scans (blue) is plotted against PSA levels in prostatectomy (A) and radiotherapy (B) patients (PSA sensitivity curve). Similarly, fraction of scans, displaying recurrent tumors at limited stage (gold), is plotted against PSA levels in prostatectomy (C) and radiotherapy (D) patients. On the basis of these curves, diagnostic window (gray) for PSMA PET imaging was derived.
As an external validation of our imaging results, biopsy and corresponding PET scan were concordant in 86.6% (13/15) of our patients (fully concordant, 73.3%; partially concordant, 13.3%; Supplemental Fig. 2).
18F-DCFPyL Displays Improved Sensitivity in Localization of Relapsed Tumors After Prostatectomy
We plotted PSA-stratified sensitivity curves separately for 18F-DCFPyL and 68Ga-PSMA-HBED-CC and noted that the sensitivity curve of 18F-DCFPyL was discretely, but robustly, shifted toward lower PSA concentrations. For PSA levels around 0.45 μg/L, local sensitivity of 18F-DCFPyL reached 62%, whereas 68Ga-PSMA-HBED-CC detected tumor relapses in 33% of the cases (Supplemental Fig. 3, arrows). The PSA-stratified sensitivity curve of 18F-DCFPyL exceeded the 68Ga-PSMA-HBED-CC curve significantly (P = 3.4 × 10−3) and substantially (average sensitivity, 80% vs. 68%) for a PSA of 0.5–3.5 μg/L.
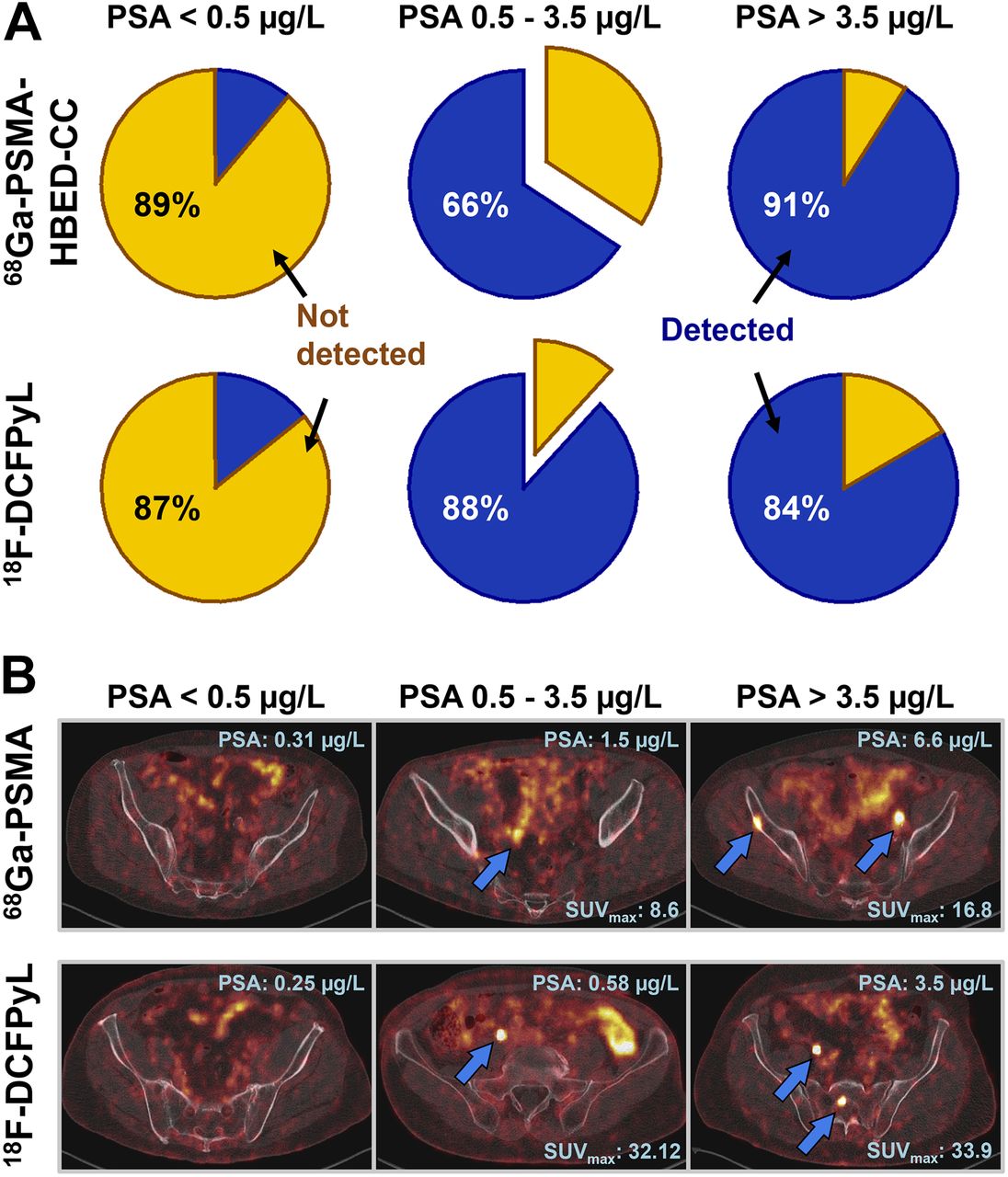
As an orthogonal approach, we counted the absolute number of PET-positive patients, as detected with either 18F-DCFPyL or 68Ga-PSMA-HBED-CC (Supplemental Table 1). For a PSA of 0.5–3.5 μg/L, we observed significantly (P = 0.042, 1-tailed χ2 test without Yates correction) and substantially (88.2% vs. 65.7%) more relapsed patients with 18F-DCFPyL (15/17) than with 68Ga-PSMA-HBED-CC (23/35). Outside this PSA range, 18F-DCFPyL and 68Ga-PSMA-HBED-CC displayed similar sensitivity (Fig. 2).
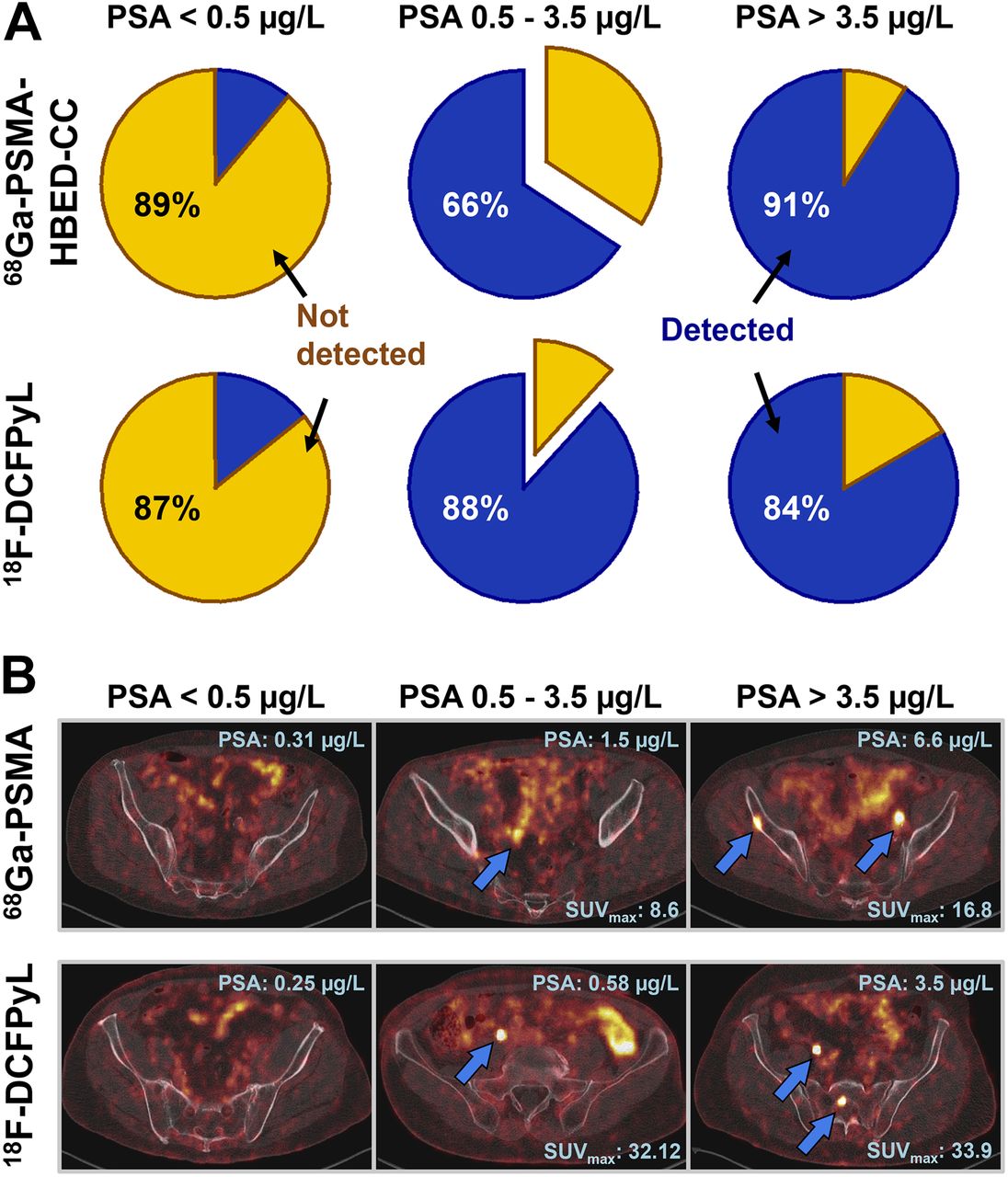
18F-DCFPyL displays enhanced sensitivity for localization of relapsed tumors after prostatectomy at limited stage. (A) Prostatectomy patients with BCR were examined with 68Ga-PSMA-HBED-CC (top) or 18F-DCFPyL (bottom). Pie charts display fractions of PET-positive (blue) and PET-negative (gold) patients with PSA < 0.5 μg/L (left), > 3.5 μg/L (right), or 0.5–3.5 μg/L (middle). (B) Representative PSMA PET/CT images (fusion ratio, 1:1), acquired with 68Ga-PSMA-HBED-CC (top) or 18F-DCFPyL (bottom). PSA level and SUVmax over PSMA-positive lesion (blue arrows) are annotated for each scan.
We next aimed to formally exclude the possibility that the substantial sensitivity differences between the 2 tracers might derive from differences in Gleason scores. We performed a mathematic confounder correction and randomly selected 30 Gleason-matched pairs from the 18F and 68Ga tracer cohorts of prostatectomy patients (1,000 iterations) (Supplemental Fig. 4). We then compared PSA-stratified sensitivity of the 18F- and 68Ga-labeled tracers for each iteration. The superiority of 18F-DCFPyL was preserved in 92.1% (all PSA levels, P = 5.3 × 10−234, paired t test against null hypothesis) and 100% (PSA < 1 μg/L, P = 2.5 × 10−294) of the iterations, respectively (Supplemental Figs. 5A and 5B). As a negative control, we randomly swapped tracer labels between matched pairs and found that random relabeling entirely abrogated the significant sensitivity difference between the 2 tracers (Supplemental Figs. 5C and 5D). This suggests that slight differences in Gleason scores cannot sufficiently account for the sensitivity differences between 18F-DCFPyL and 68Ga-PSMA-HBED-CC.
Direct Comparison of Tracer Distribution Patterns in Validation Cohort
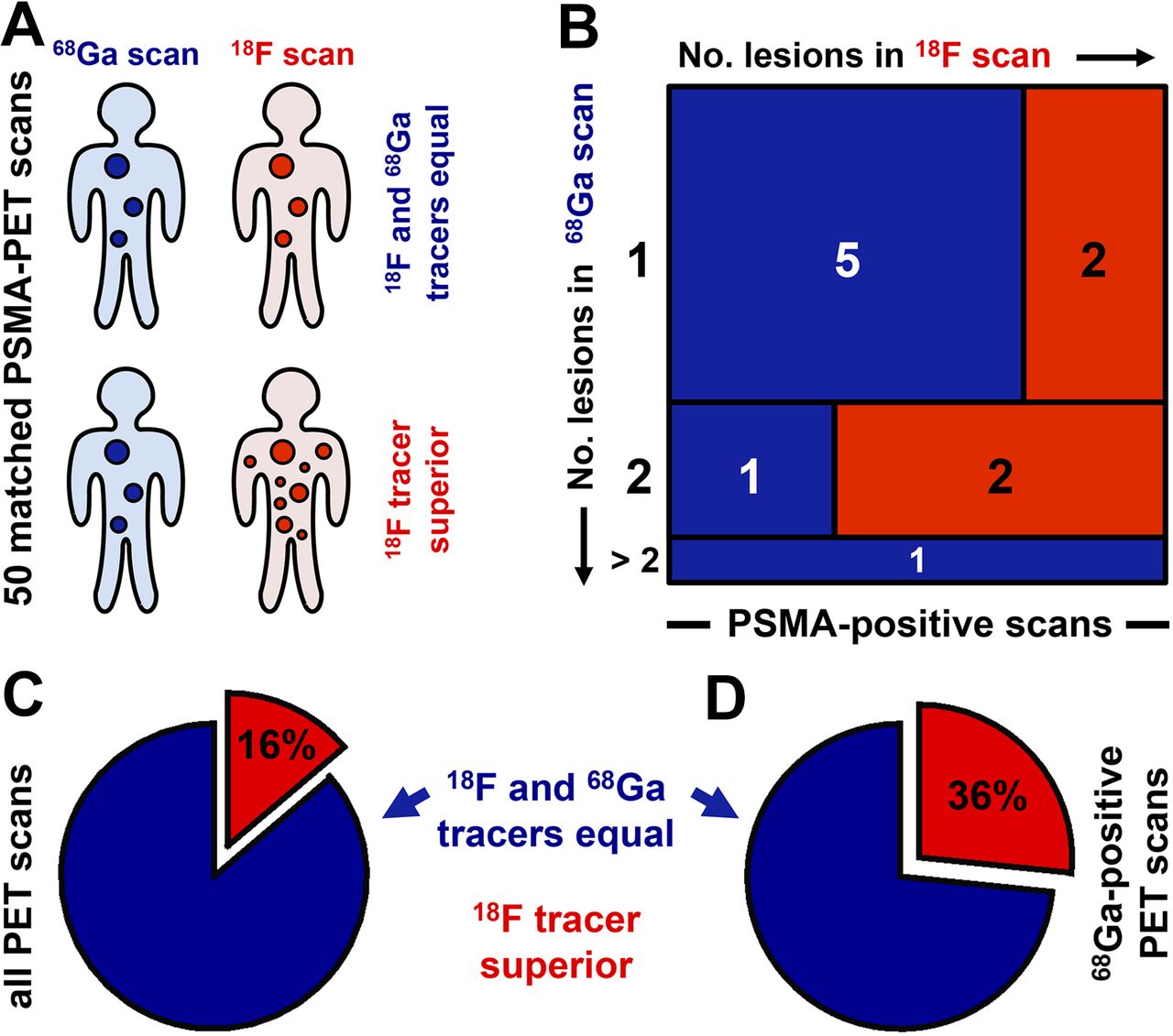
We continued our efforts of a recent pilot study (12) and sequentially examined patients with 68Ga-PSMA-HBED-CC and 18F-DCFPyL. This gave us a cohort of 25 patients, who had been scanned with both tracers (Fig. 3A). Pairwise comparison of matched PET scans revealed that tracer distribution patterns were highly concordant (P = 2.71 × 10−8), substantiating the validity of 18F-DCFPyL. In particular, all 23 PET-positive lesions on 68Ga scans could be confirmed on the corresponding 18F scan (Fig. 3B).
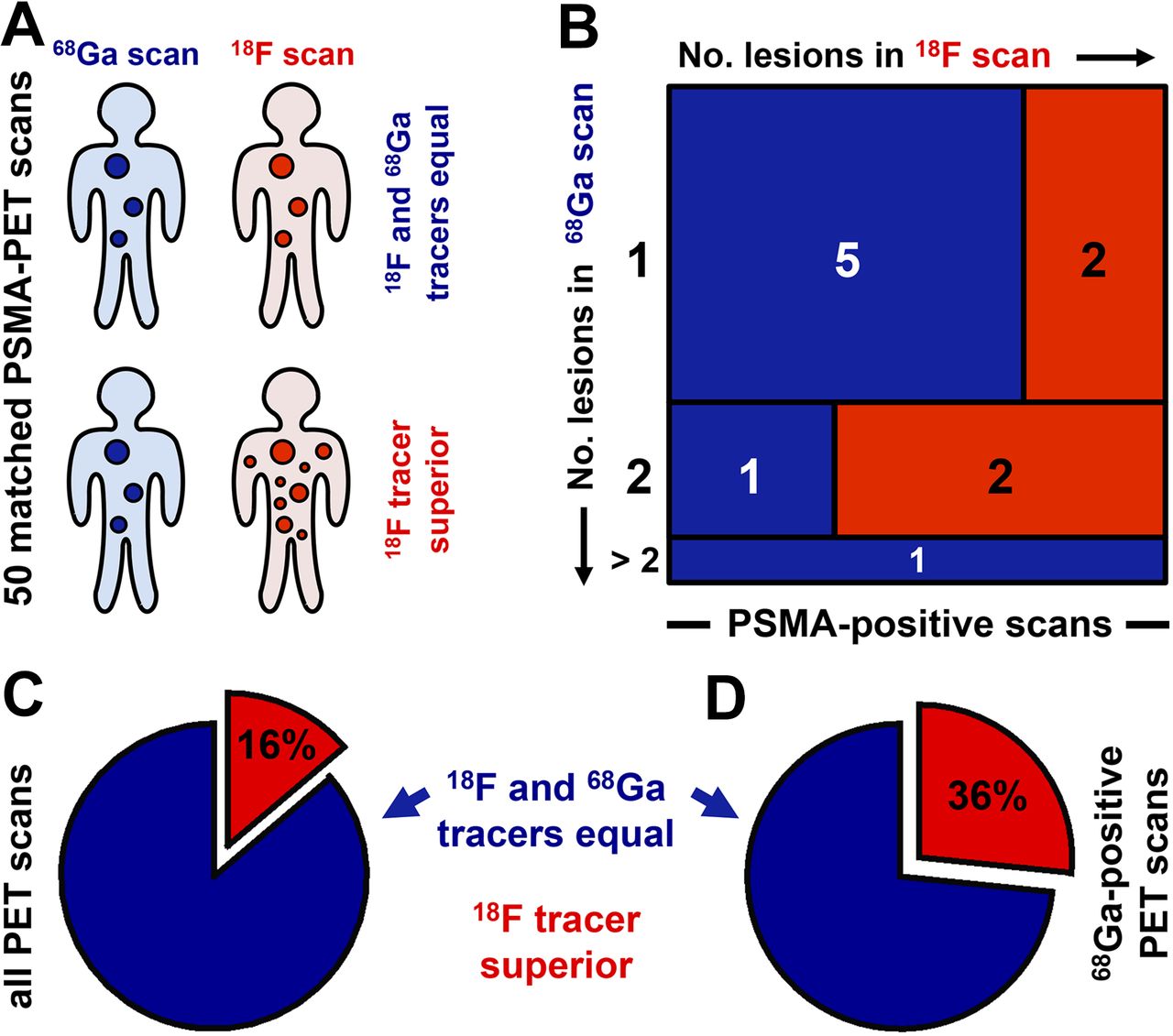
Direct comparison of distribution patterns of 18F-DCFPyL and 68Ga-PSMA-HBED-CC. (A) For 25 patients, sequentially examined with 18F-DCFPyL and 68Ga-PSMA-HBED-CC, we determined whether the 2 tracers displayed equal number of lesions. PSMA negativity was consistent for 18F-DCFPyL and 68Ga-PSMA-HBED-CC in all 14 PSMA-negative cases. (B) Mosaic plot compares PET positivity scores between the 2 tracers in all 11 PSMA-positive cases (rows: PET positivity of the 68Ga scan; columns: PET positivity of corresponding 18F scan). Each group is represented by rectangle (red: more 18F-DCFPyL–positive lesions; blue: equal PET positivity scores). Rectangle areas reflect group sizes. (C and D) Pie charts display fraction of patients with superior PET positivity of 18F-DCFPyL scan (red) (all PET scans, 25 patients, C). Alternatively, only patients with positive 68Ga scans were included (68Ga-positive PET scans, 11 patients, D).
Intriguingly, for 36% of the 68Ga-PSMA-HBED-CC–positive scans (4/11) we detected additional PET-positive lesions on the 18F-DCFPyL scan (Figs. 3C and 3D). In particular, PET positivity scores were significantly higher for the 18F-DCFPyL scans than for their corresponding 68Ga-PSMA-HBED-CC scans (P = 4.2 × 10−2) (Figs. 3B and 3C). Significance increased when only the matched PET scans of the 11 68Ga-positive patients were included in the analysis (P = 3.7 × 10−2) (Figs. 3B and 3D).
We next asked whether we could identify any obvious reasons for the increased sensitivity of 18F-DCFPyL. As exemplarily shown in Figure 4, we observed a substantial extinction of tracer signal between the kidneys in 68Ga-PSMA-HBED-CC scans, most likely due to the higher activity of 68Ga-PSMA-HBED-CC in the kidneys, compared with 18F-DCFPyL (12). This might explain why this artifact was only marginally present in the corresponding 18F-DCFPyL scan (patient 1). PET-positive lesions could therefore not be reliably excluded between the kidneys on some 68Ga-PSMA-HBED-CC scans. For instance, patient 2 revealed an 18F-DCFPyL–positive metastasis in LVB2, which was largely annihilated in the 68Ga-PSMA-HBED-CC scan (Fig. 4). Additionally, for some patients the visibility of PET-positive lesions was substantially lower with 68Ga-PSMA-HBED-CC than 18F-DCFPyL (patient 3).
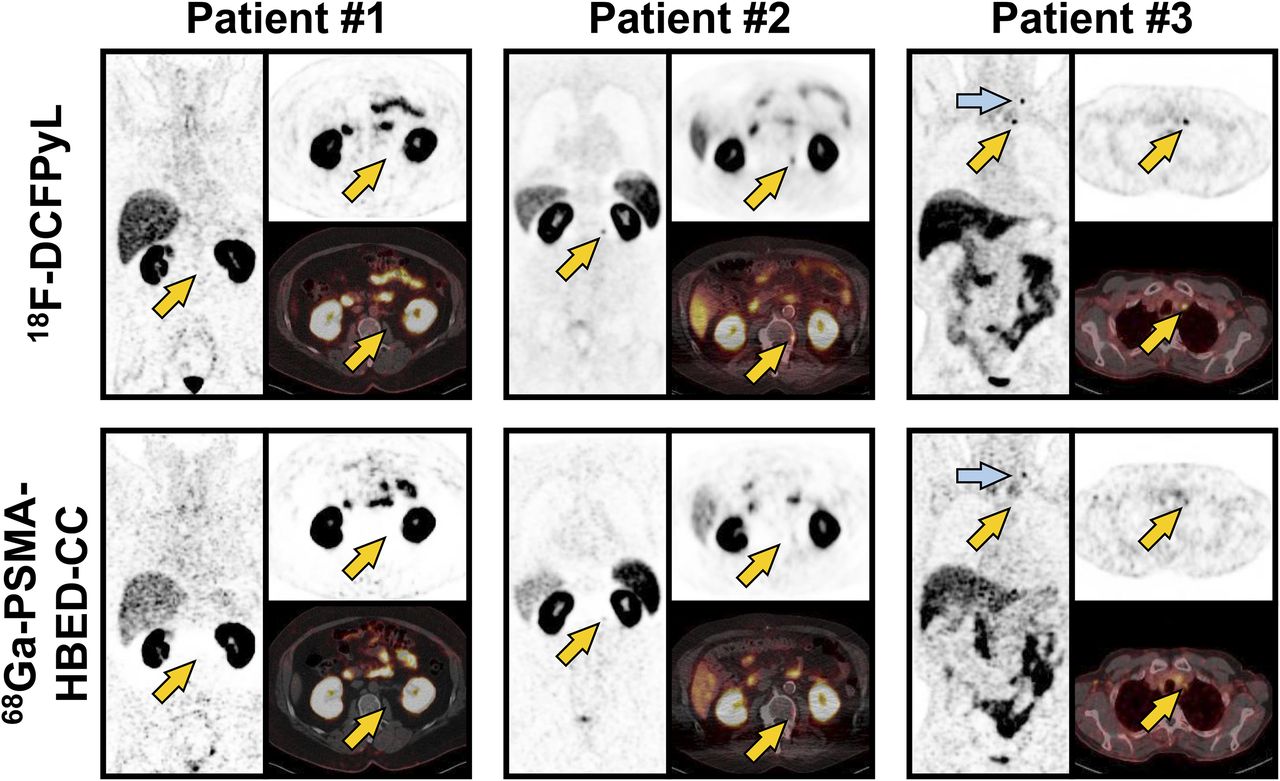
Representative matched PET scans. Images are shown for 3 PSMA-positive patients who were examined with 18F-DCFPyL (top) and 68Ga-PSMA-HBED-CC (bottom). Although patients 1 and 2 displayed clear 68Ga signal extinction artifact—that is, low activity counts between kidneys—patient 3 displayed diminished tracer contrast on 68Ga scan. Coronary (left) and transversal (top right) slices are shown for each PET scan. Additionally, PET/CT fusion image is displayed (bottom right). Arrows highlight differences between 18F and 68Ga scans. Same technical parameters (SUV windows, brightness, contrast) were used for each corresponding image pair.
DISCUSSION
PSA Levels Pinpoint Optimized Timing of PSMA PET
Accurate timing of PSMA PET substantially affects its diagnostic value in BCR patients. When PET scans are acquired too early, tumor detection rates are typically low. When PSMA PET scans are acquired too late, the number of patients identified at limited-stage disease is low, thus limiting its value for the individual patient. Our retrospective analyses suggest that the diagnostic value of PET depends on the absolute PSA level of BCR after prostatectomy, in marked contrast to the situation after radiotherapy. We established that a narrow PSA range of 0.5–3.5 μg/L allows optimal detection of cancer relapse after surgery. Thus, narrow monitoring of PSA values could well be useful for accurate timing of PET imaging.
A recent study reported a sensitivity rate of 85% for 68Ga-PSMA-HBED-CC in prostatectomy patients with BCR (7), which is fully concordant with our own observations. However, as that study did not subdivide the patient group with a PSA of less than 1 μg/L, lower detection thresholds cannot be derived. Another study reported a detection rate of 58% for patients with a PSA of less than 0.5 μg/L (5). A third retrospective study on 68Ga-PSMA-HBED-CC stratified patients using fixed PSA thresholds (6); sensitivity was 65% (0.2–0.29 μg/L), 44% (0.3–0.49 μg/L), and 71% (0.5–0.99 μg/L). This wide variability of tracer sensitivity suggests that results may be dependent on the patient cohorts examined, on the PSA thresholds selected, and on interpreter-dependent differences. We therefore compared 18F- and 68Ga-labeled PSMA tracer cohorts that had been simultaneously examined by the same interpreters at the same institution and within the same time period. Furthermore, in contrast to previous studies, we used a mathematic model, which determined tracer sensitivity for variable PSA thresholds. This enabled us to derive a PSA range, optimized for PSMA PET imaging, without a priori definition of PSA thresholds.
Sensitivity of PSMA PET Parallels PSMA Expression
Mannweiler et al. profiled PSMA expression in 51 metastasized prostate cancer patients (2). They found that 96% of primary tumors and 84% of the corresponding metastases displayed detectable PSMA levels. We therefore speculated that PSMA PET sensitivity might generally be limited to approximately 84%, due to heterogeneous PSMA expression in prostate cancer (2). Concordantly, PET imaging reached a sensitivity rate of 89% in our prostatectomy patients with a PSA of greater than 3.5 μg/L. Furthermore, we found surprisingly high PSA levels of more than 2.5 μg/L in 21% of the PSMA-negative patients, which can most likely be attributed to PSMA-negative metastases. 18F-DCFPyL reached a sensitivity of 88% in prostatectomy patients even for PSA levels of 0.5–3.5 μg/L. We thus speculate that 18F-DCFPyL exploits the full potential of PSMA tracers for a PSA of 0.5 μg/L or more.
18F-DCFPyL Allows Early Localization of Cancer Relapse
On the basis of 62 18F-DCFPyL scans, this study confirmed previous pilot studies (11,12), which reported that 18F-DCFPyL sensitivity is at least noninferior to the 68Ga-PSMA-HBED-CC standard. Intriguingly, in this larger study, 18F-DCFPyL displayed even improved detection rates in prostatectomy patients with PSA levels of 0.5–3.5 μg/L. We used matched-pair analyses to exclude the possibility that Gleason scores might affect differences in tracer sensitivity. Furthermore, we performed cross-sectional imaging of 25 patients with both tracers and found that 18F-DCFPyL detected significantly more PET-positive lesions. As this improved sensitivity of 18F-DCFPyL was thus consistent across 3 independent approaches, our results suggest that it would be well worth validating 18F-labeled PSMA tracers in future prospective trials.
Nevertheless, we note that our study had the following limitations. We derived the lower PSA threshold (0.5 μg/L) retrospectively from our PET imaging results. Below this threshold, our tracer sensitivity rates were substantially lower than the results of previous studies on 68Ga-PSMA-HBED-CC for PSA levels of 0.2–0.5 μg/L (5,6). One explanation for this incongruence might lie in our scoring system, whereby a PET-positive lymph node required a morphologic correlate in the corresponding low-dose CT scan. Thus, we cannot formally exclude the possibility that PET-positive lymph nodes without a clear CT-morphologic correlate were misinterpreted as physiologic tracer accumulation in the ureter or intestine. Hence, interobserver variability may affect the lower PSA threshold. Similarly, we defined the upper PSA threshold (3.5 μg/L) based on our PET imaging results. Although none of our PET-negative patients displayed suggestive lesions on the corresponding CT scan, we cannot rule out the possibility that some patients diagnosed as limited stage carried additional PET-negative lesions at distant sites.
The standard tracer acquisition protocols (3,5,7,12) used in this study included different tracer uptake time periods for 18F-DCFPyL (120 min) and 68Ga-PSMA-HBED-CC (60 min) before image acquisition, because of the shorter half-life of the 68Ga label. This time difference of 60 min may contribute to the increased sensitivity of 18F-DCFPyL, as a recent pilot study observed that delayed image acquisition improved the quality of 68Ga-PSMA-HBED-CC scans for 4 patients (8). Furthermore, standard acquisition protocols (3,5,7,12) recommend different activity dosages for 18F-DCFPyL (250 MBq) and 68Ga-PSMA-HBED-CC (150 MBq), because of the small yields of local gallium generators in routine diagnostic procedures. Perhaps not surprisingly, a recent pilot study (12) thus reported significantly higher SUVmax in tumor lesions for 18F-DCFPyL than 68Ga-PSMA-HBED-CC, which enhances the tumor-to-background ratio of 18F-DCFPyL scans and might thus facilitate their interpretation. Although challenging in routine diagnostics, a potential improvement of the acquisition protocol for 68Ga-PSMA-HBED-CC might thus be prolongation of the acquisition time for PET scans. Our uptake time periods and tracer dosages are in full concordance with standard acquisition protocols of previous studies (3,5,7,12). Furthermore, a large prospective trial obtained PET scans with 68Ga-PSMA-HBED-CC after an even shorter time period of 45 min but still observed high sensitivity (6). Hence, optimized acquisition protocols for PSMA tracers remain a current matter of debate.
An additional factor, contributing to the increased sensitivity of 18F-DCFPyL, was the reduced tracer signal extinction between the kidneys, which we observed for 18F-DCFPyL. A recent study reported that the quality of 68Ga-PSMA-HBED-CC scans could be improved by delayed imaging after forced diuresis (9). In this study, we did not use forced diuresis, although this might well provide a means of improving the performance of both tracers.
Histologic validation was available only for a relatively small subcohort of patients. Hence, tracers could not be compared on the basis of histopathologic results and we cannot formally exclude the possibility that additional 18F-DCFPyL–positive lesions represent false-positive results. Furthermore, we obtained local biopsies exclusively from the prostate fossa of PET-positive patients with limited relapse. Consequently, PET-negative and advanced-staged patients did not undergo biopsy, so that our histopathologic validation was not independent of PET results. However, given the high coincidence between the distribution patterns of 68Ga-PSMA-HBED-CC and 18F-DCFPyL (including subthreshold correlates of 18F-DCFPyL–positive lesions in the corresponding 68Ga-PSMA-HBED-CC scan) as well as the morphologic correlates of PET-positive lesions in the corresponding CT scan, there is accumulating evidence for the validity of 18F-DCFPyL. Four recent studies reported that PSMA-positive lesions could be histologically confirmed in 82%, 94%, 99%, and 100% of cases, respectively (13–16).
Despite its limitations, the major strengths of this study are that we provide the largest cohort of BCR patients examined with 18F-DCFPyL to date and that both tracers were used simultaneously at the same institution and analyzed by the same interpreters. Furthermore, we used a wide spectrum of mathematic models, including iterative Gleason-matched-pair analyses, to separately analyze prostatectomy and radiotherapy cohorts. Additionally, we applied variable PSA thresholds without making any a priori assumptions. Finally, we cross-validated our results using a separate cohort of 25 patients who were sequentially examined with both tracers, thus allowing a direct comparison of the distribution patterns of 18F- and 68Ga-labeled PSMA tracers.
CONCLUSION
Our data suggest that 18F-DCFPyL is noninferior to 68Ga-PSMA-HBED-CC while offering all the advantages of 18F labeling. Imaging with 18F-DCFPyL may even exhibit improved sensitivity, when PSA levels are moderately increased to between 0.5 and 3.5 μg/L after prostatectomy. This is of high clinical relevance because within this PSA range PSMA PET imaging detected most relapses at a limited stage. Hence, our findings provide a promising basis for validation of 18F-DCFPyL in future prospective trials.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
↵* Contributed equally to this work.
Published online Dec. 1, 2016.
- © 2017 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication October 13, 2016.
- Accepted for publication November 25, 2016.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- An 89Zr-Labeled PSMA Tracer for PET/CT Imaging of Prostate Cancer Patients
- Diagnostic Performance and Clinical Impact of 68Ga-PSMA-11 PET/CT Imaging in Early Relapsed Prostate Cancer After Radical Therapy: A Prospective Multicenter Study (IAEA-PSMA Study)
- Appropriate Use Criteria for Prostate-Specific Membrane Antigen PET Imaging
- Protocol for 18F-PSMA PET imaging in staging and management of prostate cancer - a retrospective cohort study
- Comparison of Dual-Tracer PET and CT Features to Conventional Risk Categories in Assessing Response to 177Lu-PSMA-617 Therapy for Metastatic Prostate Adenocarcinoma with Urinary Bladder Involvement
- Intraindividual Comparison of 18F-PSMA-1007 with Renally Excreted PSMA Ligands for PSMA PET Imaging in Patients with Relapsed Prostate Cancer
- Prospective Evaluation of 18F-DCFPyL PET/CT in Biochemically Recurrent Prostate Cancer in an Academic Center: A Focus on Disease Localization and Changes in Management
- An 18F-Labeled PSMA Ligand for PET/CT of Prostate Cancer: First-in-Humans Observational Study and Clinical Experience with 18F-JK-PSMA-7 During the First Year of Application
- Lesion Detection and Interobserver Agreement with Advanced Image Reconstruction for 18F-DCFPyL PET/CT in Patients with Biochemically Recurrent Prostate Cancer
- Matched-Pair Comparison of 68Ga-PSMA-11 PET/CT and 18F-PSMA-1007 PET/CT: Frequency of Pitfalls and Detection Efficacy in Biochemical Recurrence After Radical Prostatectomy
- Simplified Methods for Quantification of 18F-DCFPyL Uptake in Patients with Prostate Cancer
- A Prospective Study on 18F-DCFPyL PSMA PET/CT Imaging in Biochemical Recurrence of Prostate Cancer
- Bridging the Imaging Gap: PSMA PET/CT Has a High Impact on Treatment Planning in Prostate Cancer Patients with Biochemical Recurrence--A Narrative Review of the Literature
- Preclinical Evaluation and Pilot Clinical Study of Al18F-PSMA-BCH for Prostate Cancer PET Imaging
- Discovery of 18F-JK-PSMA-7, a PET Probe for the Detection of Small PSMA-Positive Lesions
- Interobserver Agreement for the Standardized Reporting System PSMA-RADS 1.0 on 18F-DCFPyL PET/CT Imaging
- Intraindividual Comparison of 18F-PSMA-1007 and 18F-DCFPyL PET/CT in the Prospective Evaluation of Patients with Newly Diagnosed Prostate Carcinoma: A Pilot Study
- Comparison of 68Ga-PSMA-11 and 18F-Fluciclovine PET/CT in a Case Series of 10 Patients with Prostate Cancer Recurrence
- Biochemical Recurrence of Prostate Cancer: Initial Results with [18F]PSMA-1007 PET/CT
- PSMA Ligands for Imaging Prostate Cancer: Alternative Labeling by Complex Formation with Al18F2+
- Seduction by Sensitivity: Reality, Illusion, or Delusion? The Challenge of Assessing Outcomes after PSMA Imaging Selection of Patients for Treatment
- Initial Experience with Volumetric 68Ga-PSMA I&T PET/CT for Assessment of Whole-Body Tumor Burden as a Quantitative Imaging Biomarker in Patients with Prostate Cancer
- PSMA Ligands for PET Imaging of Prostate Cancer