


Abstract
Assessment of reversible perfusion defects in exercise 201Tl perfusion SPECT has low sensitivity and high specificity for detection of multivessel coronary artery disease (CAD). The goal of this study was to evaluate whether worsening of left ventricular regional wall motion assessed by an automated algorithm in exercise 201Tl electrocardiography-gated SPECT had incremental diagnostic value over perfusion data for detection of multivessel CAD. Methods: Two hundred one patients underwent exercise 201Tl gated SPECT. Software that automatically analyzes left ventricular function was used to assess exercise and rest regional wall motion. Regional wall motion on initial images was compared with that on rest images, that is, delayed images for patients without reinjection images and reinjection images for patients with reinjection images. The left ventricle was divided into 9 segments, with individual segments assigned to 3 coronary territories. Worsening of wall motion was defined as worsening in any segment on initial images compared with rest images. Results: Of 73 patients with multivessel CAD, 20 (27.4%) had reversible perfusion defects in multiple coronary territories, 26 (35.6%) exhibited worsening of regional wall motion in multiple territories, and 37 (50.7%) had reversible perfusion defects or worsening of regional wall motion in multiple territories. The sensitivity of the combination of reversible perfusion defect and worsening of regional wall motion was significantly higher than that of reversible perfusion defect alone for detection of multivessel CAD (50.7% vs. 27.4%, P < 0.05). The specificity of the combination of reversible perfusion defect and worsening of regional wall motion for detecting multivessel CAD did not differ from that of reversible perfusion defect alone and that of worsening of regional wall motion alone (94.5% vs. 99.2% and 97.7%, respectively, P = not statistically significant). Conclusion: Combined assessment of worsening of left ventricular regional wall motion by exercise and perfusion data in exercise 201Tl gated myocardial SPECT was more sensitive, with acceptable specificity, than was assessment with perfusion data alone for detection of multivessel CAD.
An important goal of noninvasive stress testing is the identification of patients with multivessel coronary artery disease (CAD). Such patients could benefit prognostically from revascularization (1). Exercise 201Tl myocardial perfusion imaging is a well-established method for diagnosis and risk stratification of patients with CAD (2–5). This method of diagnosis is based primarily on the detection of perfusion defects. However, a potential limitation of 201Tl scanning is that a measure of relative rather than absolute myocardial blood flow is obtained. In patients with multivessel CAD, the degree of ischemia may be underestimated because of relatively balanced global hypoperfusion of the left ventricle (LV) without absolute quantification of regional blood flow. Perfusion defects may be evident only in the most ischemic area, whereas the least ischemic area may appear normal. Because of this problem, some but not all patients with multivessel CAD have perfusion abnormalities in all of the expected coronary arterial territories on 201Tl imaging. Moreover, exercise endpoints, such as anginal pain, a positive electrocardiography (ECG) change, or arrhythmia, which are related to premature interruption of an exercise stress test, may be responsible for detection of the culprit lesion only, the threshold of ischemia for the other stenosis not being reached. The result is a decrease in the sensitivity of all scintigraphic parameters for the detection of multivessel CAD. Previous reports (6–8) estimated that as few as 13%–50% of patients with 3-vessel or left main CAD had perfusion abnormalities in multiple territories. To improve the performance of scintigraphic methods for detection of multivessel CAD, the use of indirect scintigraphic indices other than perfusion defects has been reported and validated, that is, increased lung (9,10) or right ventricle (11) uptake of 201Tl, transient ischemic LV dilatation (9,12), and myocardial 201Tl washout (13).
An automated algorithm (14,15) for direct evaluation of LV function based on the results of ECG-gated myocardial perfusion SPECT is now commercially available. The algorithm simultaneously yields information on myocardial perfusion and LV regional and global function. Although this automated algorithm was initially validated using 99mTc-labeled tracers (14,15), recent studies (16–18) have validated the accuracy of 201Tl gated SPECT for measurement of LV function and have shown its feasibility and reliability.
Myocardial stunning caused by exercise-induced ischemia has been reported to result in depression of systolic LV function in the ischemic zone (19–21). In patients with severe coronary artery stenoses or multivessel CAD, repeated episodes of ischemic stunning may lead to depression of LV function. Because of the possibility that LV regional and global function have not returned to baseline by the time of postexercise acquisition of 201Tl gated SPECT in some patients with exercise-induced ischemia, documentation of worsening of regional wall motion is thought to be clinically useful in the diagnosis of myocardial ischemia. A recent study (22) showed that in patients with normal resting perfusion, a postexercise regional wall motion abnormality detected by 99mTc-sestamibi gated SPECT is a sensitive marker of severe and multivessel CAD. This study was therefore designed to determine whether worsening of regional wall motion as assessed by an automated algorithm in exercise 201Tl ECG-gated SPECT had incremental diagnostic value over perfusion data for detection of multivessel CAD.
MATERIALS AND METHODS
Patient Population
We identified 201 consecutive patients with normal sinus rhythm and known or suspected CAD who underwent exercise 201Tl myocardial SPECT and coronary arteriography in Osaka City University Hospital between January 1999 and October 2000. Patients who had undergone coronary artery bypass grafting were excluded. Baseline characteristics of the 201 patients are shown in Table 1. Fifteen of the 201 patients had significant left main CAD that was considered equivalent to combined disease of the left anterior descending artery and the left circumflex artery.
Baseline Characteristics of 201 Patients
Exercise 201Tl Myocardial SPECT
Each patient performed symptom-limited exercise on a bicycle ergometer. The workload initially was 25 or 50 W and was increased 25 W every 2 min until an endpoint was reached. The endpoints included excessive fatigue, dyspnea, moderate to severe angina, hypotension, diagnostic ST depression (>1.5 mm horizontal or downsloping at the J point or >2.0 mm upsloping at 80 ms after the J point), or significant arrhythmia. At peak exercise, 201Tl (111 MBq for patients without previous myocardial infarction and 74 MBq for patients with previous myocardial infarction) was injected intravenously and the patient was encouraged to exercise for an additional minute. Initial images were obtained immediately after the termination of exercise, and delayed images were obtained 4 h later. In patients with previous myocardial infarction, an additional dose of 37 MBq 201Tl was injected at rest immediately after the acquisition of delayed images, and the reinjection images were obtained 20 min later.
SPECT was performed with a 2-detector gamma camera (Vertex; ADAC Laboratories, Milpitas, CA) equipped with low-energy, general-purpose collimators, with the detectors set to form a 90° angle. A total of 32 equidistant projections were acquired over 180 degrees in a 64 × 64 matrix from the 45° right anterior oblique projection to the 45° left posterior oblique projection with an energy window of 70 keV ± 10%. ECG-gated images were acquired with 40-s, 6° angular steps. At each projection, 8 frames per cardiac cycle were acquired, with an allowable change in R-R interval of the mean value ± 20%. Nongated images for assessment of 201Tl uptake were obtained by summing all gated images. Transaxial slices of 4.7-mm-pixel thickness were reconstructed using a Butterworth filter (order, 5.0; critical frequency, 0.35 cycle per pixel) and the filtered backprojection method (ramp filter) on a processing computer (Pegasys; ADAC Laboratories) with an automatic reorientation algorithm for SPECT (AutoSPECT; Cedars-Sinai Medical Center, Los Angeles, CA) (23). No attenuation correction was applied.
Scintigraphic Image Analysis
Perfusion Defects.
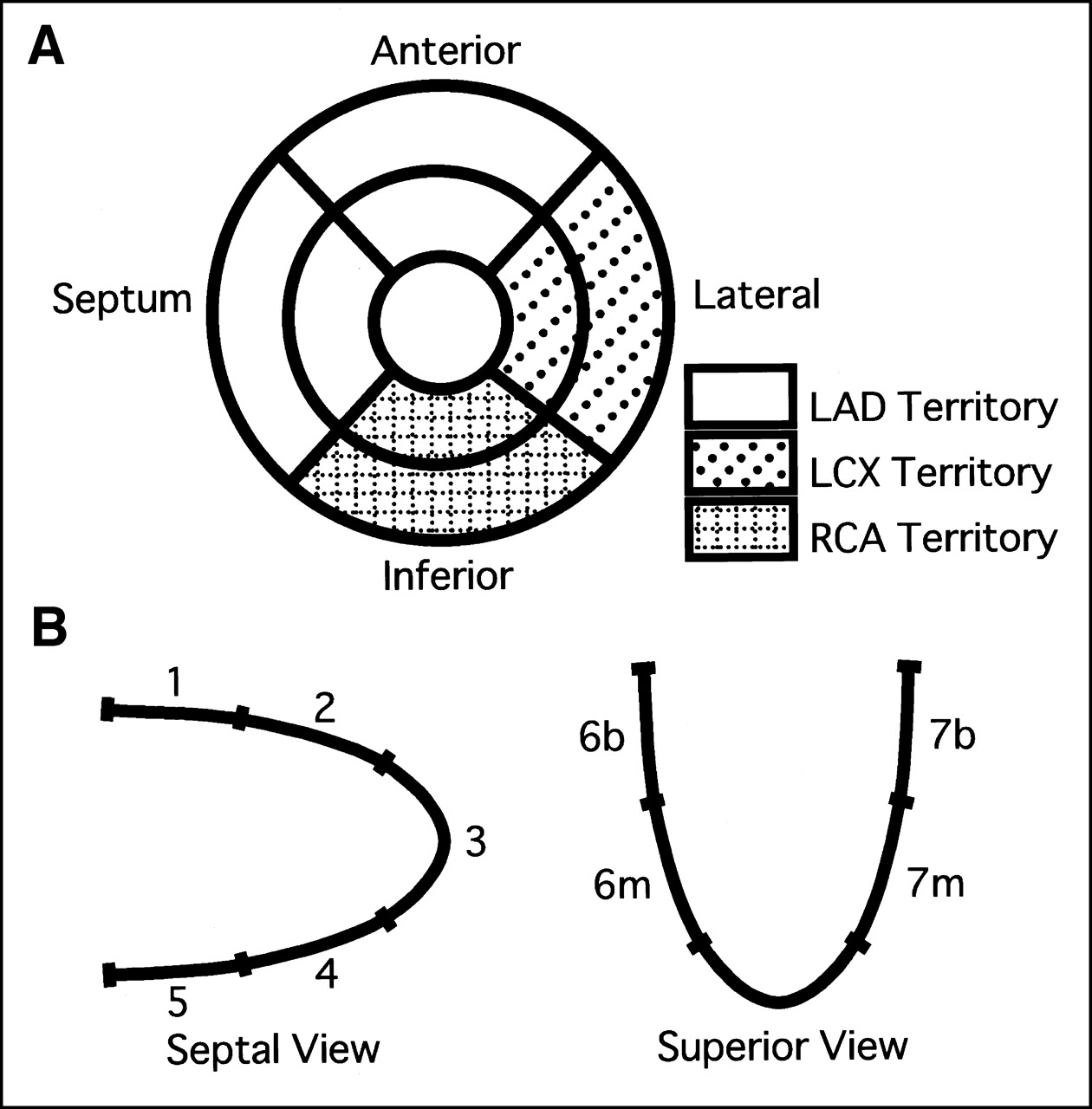
Two experienced observers interpreted the tomographic images visually by consensus without knowledge of patient clinical information or angiographic data. The LV was divided into 9 segments (Fig. 1A). The 201Tl uptake of each segment was assessed with a 4-point scoring system (3 = normal; 2 = mildly reduced; 1 = moderately reduced; 0 = severely reduced or absent). A reversible perfusion defect was defined as ≥1 grade improvement in any segment on the delayed images or reinjection images compared with the initial images. The 9 segments were assigned to 3 coronary territories as shown in Figure 1A. Reversible LV perfusion defects were classified according to the vascular territories of the 3 major coronary arteries; anterior, septal, and apical defects represented disease in the left anterior descending artery, inferior defects represented disease in the right coronary artery, and lateral defects represented disease in the left circumflex artery. Because of overlap between coronary territories, minimal (less than approximately 25%) extension of a perfusion defect into the adjacent territory was considered a perfusion defect of the predominant territory.

Relationship between short-axis tomographic segments and coronary arterial territories (A) and schema of 9 segments of left ventricle on 3-dimensional cine-mode display created with automatic left ventricular function analysis software program for ECG-gated myocardial perfusion SPECT (B). Reversible perfusion defects and worsening of wall motion in anterior, septal, and apical segments represented disease in left anterior descending artery (LAD), those in inferior segments represented disease in right coronary artery (RCA), and those in lateral segments represented disease in left circumflex artery (LCX). 1 = basal anterior; 2 = middle anterior; 3 = apex; 4 = middle inferior; 5 = basal inferior; 6b = basal septum; 6m = middle septum; 7b = basal lateral; 7m = middle lateral.
LV Ejection Fraction.
A completely automated software program that analyzes LV function (Quantitative Gated SPECT; Cedars-Sinai Medical Center) (14,15) was used to calculate global LV ejection fraction. Rest LV ejection fraction was derived from delayed images for patients without reinjection images and from reinjection images for patients with reinjection images.
LV Regional Wall Motion.
LV regional wall motion was analyzed visually on a 3-dimensional cine-mode endocardial display created with the automatic program that analyzes LV function (Quantitative Gated SPECT). Two experienced observers independently analyzed wall motion on initial images and on rest images, that is, delayed images for patients without reinjection images and reinjection images for patients with reinjection images, without knowledge of patient clinical information or angiographic data. Disagreements in interpretation were resolved by observer consensus. The LV was divided into 9 segments (Fig. 1B). Regional wall motion was graded using the following scores: 3 = normal or hyperkinetic, 2 = mildly hypokinetic, 1 = severely hypokinetic, and 0 = akinetic or dyskinetic. Regional wall motion on the initial images was compared with that on the rest images with side-by-side display of 3-dimensional cine-mode endocardial images. Worsening of wall motion was defined as ≥1 grade worsening in any segment on the initial images compared with rest images. The individual segments were assigned to 3 coronary territories as described for perfusion analysis.
Coronary Arteriography
All patients underwent coronary arteriography within 10 wk (6 ±12 d) of 201Tl SPECT. Coronary artery narrowing was visually assessed and reported as percentage luminal diameter stenosis. Significant coronary stenosis was defined as ≥70% narrowing of the internal diameter of the left anterior descending artery, the left circumflex artery, the right coronary artery, or their major branches and ≥50% narrowing of the left main coronary artery. Multivessel disease was defined by the presence of significant left main coronary artery disease or of 3- or 2-vessel disease on the coronary angiogram.
Statistics
Values are given as mean ± SD. κ statistics were used to evaluate the concordance of diagnosis of the number of diseased vessels with coronary arteriography and perfusion data in 201Tl SPECT. Incidences of phenomena were compared with the χ2 test. P < 0.05 was considered significant.
RESULTS
Scintigraphic Data and Number of Diseased Vessels
The relationship between scintigraphic data and number of diseased vessels is shown in Table 2. Only 20 (27.4%) of 73 patients with multivessel CAD had reversible perfusion defects in multiple territories.
Relationships Between Perfusion Data and Number of Diseased Vessels
Inter- and Intraobserver Agreement in Evaluating Worsening of Regional Wall Motion
The interobserver concordance rate in evaluating worsening of regional wall motion was 90.5% (κ = 0.70; P < 0.001). One of 2 observers reassessed worsening of regional wall motion 1 mo after the first evaluation. The intraobserver concordance rate was 92.0% (κ = 0.77; P < 0.001).
Reversible Perfusion Defect, Worsening of Regional Wall Motion, and Individual Coronary Stenosis
Comparisons of individual coronary stenosis with reversible perfusion defect, worsening of regional wall motion, and the combination of reversible perfusion defect and worsening of regional wall motion are shown in Tables 3–6.
Comparison of Scintigraphic and Coronary Angiographic Findings in LAD
Comparison of Scintigraphic and Coronary Angiographic Findings in RCA
Comparison of Scintigraphic and Coronary Angiographic Findings in LCX
Comparison of Scintigraphic and Coronary Angiographic Findings in Coronary Arteries Overall
The sensitivity of the combination of reversible perfusion defect and worsening of regional wall motion—that is, presence of reversible defects, worsening of regional wall motion, or both—did not differ from that of reversible perfusion defect alone for identification of left anterior descending artery lesions or left circumflex artery lesions but was significantly higher than that of reversible perfusion defect alone for identification of right coronary artery lesions (71.2% vs. 51.5%, P < 0.05). The specificity of the combination of reversible perfusion defect and worsening of regional wall motion for identification of individual stenosed coronary arteries was slightly but not significantly lower than that of reversible perfusion defect alone and that of worsening of regional wall motion alone but remained >90%.
The sensitivity of the combination of reversible perfusion defect and worsening of regional wall motion for identification of any stenosed vessel was significantly higher than that of reversible perfusion defect alone and that of worsening of regional wall motion alone (61.2% vs. 46.4%, P < 0.01, and 61.2% vs. 44.7%, P < 0.01, respectively). There was no significant difference in the specificity for identification of any stenosed vessel among reversible perfusion defect alone, worsening of regional wall motion alone, or the combination of reversible perfusion defect and worsening of regional wall motion (96.2%, 96.4%, and 93.4%, respectively).
Detection of Multivessel CAD
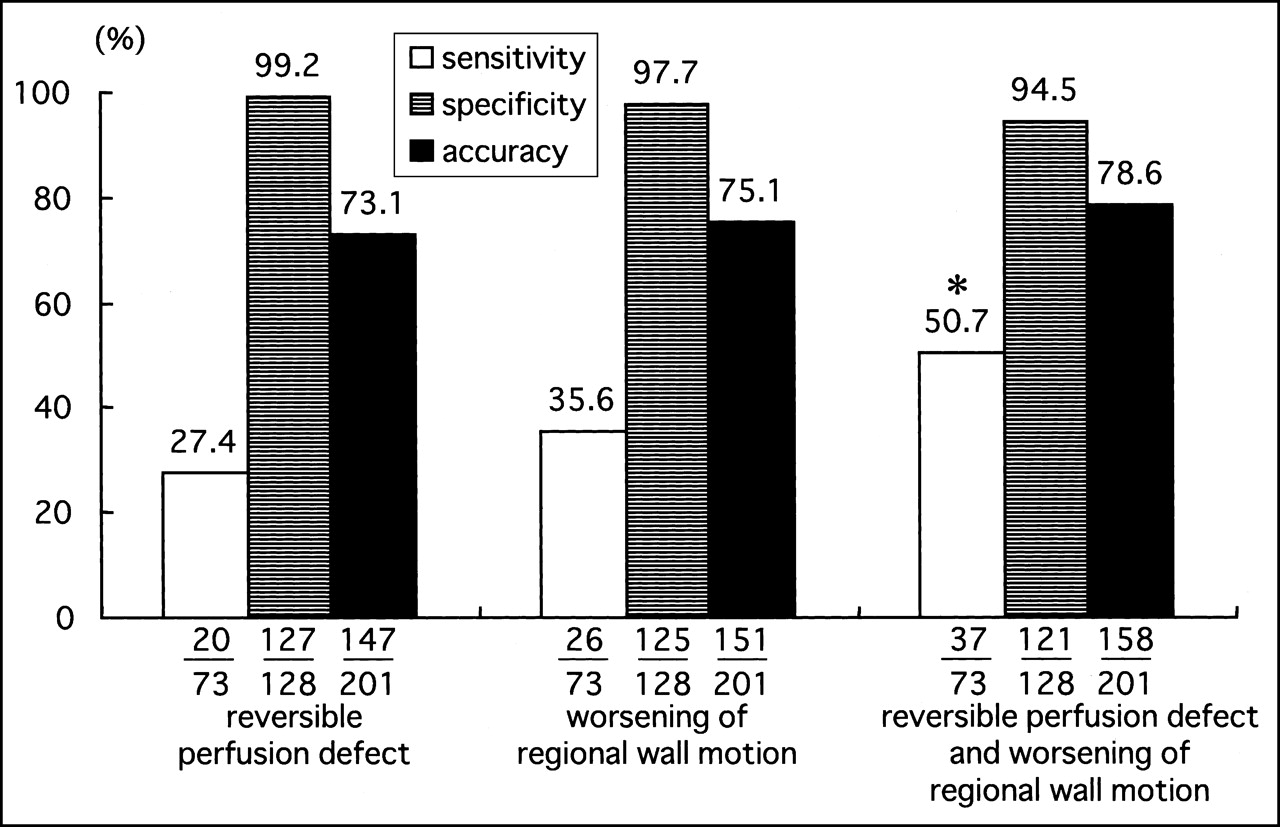
The patients were assigned to 2 groups by the presence or absence of multivessel CAD (Fig. 2). Thirty-seven (50.7%) of the 73 patients with multivessel CAD had reversible perfusion defects or worsening of regional wall motion in multiple coronary territories. The sensitivity of the combination of reversible perfusion defect and worsening of regional wall motion for identification of multivessel CAD was significantly higher than that of reversible perfusion defect alone (50.7% vs. 27.4%, P < 0.05). The specificity of the combination of reversible perfusion defect and worsening of regional wall motion for identification of multivessel CAD did not differ from that of reversible perfusion defect alone and that of worsening of regional wall motion alone (94.5% vs. 99.2% and 97.7%, respectively, P = not statistically significant).

Sensitivity, specificity, and accuracy in identification of multivessel CAD. *P < 0.05 compared with reversible perfusion defect alone.
Representative images from a patient with a previous inferior myocardial infarction treated with coronary stent placement are shown in Figures 3 and 4.

Representative images of tomograms from 57-y-old woman with 50% stenosis of left main coronary artery and no significant stenosis in right coronary artery. She had previous inferior myocardial infarction, which had been treated with placement of coronary stent in right coronary artery. Tomographic images revealed fixed defect in inferior wall.

Left ventricular functional images obtained by ECG-gated myocardial SPECT from same patient as in Figure 3. Outer cage and solid surface represent endocardial surfaces at end-diastole and end-systole, respectively. In initial images, anteroapical wall, septum, and lateral wall were hypokinetic and inferior wall was akinetic. In reinjection images, anteroapical wall, septum, and lateral wall were normokinetic and inferior wall was akinetic. Worsening of regional wall motion was observed in anteroapical wall, septum, and lateral wall. These findings suggested left anterior descending artery disease and left circumflex artery disease.
DISCUSSION
Our results showed that assessment of worsening of regional wall motion by exercise in 201Tl ECG-gated SPECT had incremental diagnostic value over perfusion data for detection of multivessel CAD. In particular, the combination of assessment of worsening of regional wall motion by exercise and perfusion data in exercise 201Tl myocardial SPECT was more sensitive, with acceptable specificity, than assessment of perfusion data alone for detection of multivessel CAD.
Myocardial stunning was initially reported in animal models of coronary occlusion and reperfusion (24) and was subsequently also shown to result from exercise-induced ischemia. The time course of resolution of ischemic LV dysfunction in patients has been reported to range from immediate to 2 h (19–21). An echocardiographic study (19) revealed persistence of regional wall motion abnormalities 30 min after completion of exercise in a high proportion of patients with multivessel CAD. Myocardial uptake of perfusion tracer at the time of acquisition represents the relative myocardial perfusion pattern at the time of tracer injection, whereas functional data derived from ECG gating represent LV function at the time of acquisition. Acquisition of the initial images in this study required approximately 15 min after completion of exercise. Accordingly, in some of the patients with exercise-induced ischemia, LV regional and global function might have already returned to baseline by the completion of postexercise acquisition. In patients with severe coronary artery stenosis, stunning does occur as a consequence of repeated episodes of ischemia during daily life, and repeated episodes of ischemic stunning lead to chronic depression of LV function (25). It is therefore possible that in some patients with severe coronary artery stenosis, LV regional and global function might be reduced even at rest and that exercise might not induce additional LV dysfunction. For these reasons, the worsening of LV regional wall motion by exercise might have relatively low sensitivity for detection of multivessel CAD.
Because the severity and duration of postischemic functional depression depend on the severity of ischemia (20,21), recent studies have shown a good relationship between the severity of perfusion abnormalities and exercise-induced LV dysfunction in exercise perfusion scanning (26,27). However, in patients with multivessel CAD, the degree of ischemia may be underestimated because of relatively balanced LV global hypoperfusion without absolute quantification of regional blood flow. In this study, perfusion data revealed reversible defects in multiple territories in only 20 (27.4%) of 73 patients with multivessel CAD, a finding comparable with those of previous studies (6–8), whereas among 53 patients with a reversible defect in less than 1 territory and multivessel CAD, the combination of reversible perfusion defect and worsening of regional wall motion detected 17 (32.1%) as having multivessel CAD.
Sharir et al. (22) showed that postexercise regional wall motion abnormality detected by 99mTc gated sestamibi SPECT had incremental diagnostic value over perfusion data in identification of severe (≥90% proximal stenosis or midstenosis) and extensive (>1 coronary artery with stenosis) CAD in patients with normal resting perfusion. The addition of regional wall motion variables to perfusion data resulted in a significant increase in the global χ2 for prediction of severe multivessel CAD. Overall sensitivity and specificity in identification of any severely stenosed vessel by severe perfusion defect or wall motion abnormality were 82% and 80%, respectively. The study of Sharir et al. was limited to patients with normal resting perfusion and excluded those who had pathologic Q waves on the ECG at rest and those who had undergone a revascularization procedure. We defined significant coronary stenosis as ≥70% lumen diameter narrowing of any of the major branches and ≥50% narrowing of the left main coronary artery, and our study group included patients who had previous myocardial infarction and had undergone percutaneous transluminal coronary angioplasty. We showed that worsening of wall motion by exercise had the potential to indicate moderate or severe multivessel CAD in a group of patients including those who had evidence of previous myocardial infarction.
Stress echocardiography performed with exercise or administration of a pharmacologic agent has become another well-established imaging modality for assessment of the presence, localization, and extent of CAD. This modality is based on the concept that new or worsening regional myocardial contractility induced by ischemia can reliably be detected by echocardiographic wall motion analysis. Several studies have shown its ability to detect multivessel disease. Roger et al. (28) showed that exercise echocardiography can detect multivessel CAD (left main coronary artery or 3- or 2-vessel disease with ≥50% stenosis) with a clinically useful degree of accuracy and that echocardiographic images add independent and incremental value to clinical and exercise variables alone. In their study, the overall sensitivity and specificity of exercise echocardiography for the identification of multivessel disease were 73% and 70%, respectively. The exclusion criterion in their study was a previous revascularization procedure. They defined a region as abnormal if the contractility of a corresponding segment was visualized as abnormal either at rest or on postexercise images. Therefore, the sensitivity and specificity of their results were directly affected by the percentage of patients who had abnormal regional wall motion at rest, that is, those with previous myocardial infarction. However, we showed that assessment of worsening of regional wall motion by exercise had incremental value for detection of multivessel disease in a population that included patients with previous myocardial infarction treated with coronary angioplasty.
Several limitations of this study should be considered. In our patients, the indication of coronary arteriography was determined by physicians on the basis of SPECT findings or other clinical variables, and patient selection was therefore biased.
It is possible that visual analysis of regional wall motion is more subjective than quantitative analysis. However, visual assessment could be the most common method of detecting multivessel CAD and is therefore important for generalization of our results to clinical practice.
We evaluated completely or partially reversible defects, but not fixed defects, as a perfusion variable to identify patients with CAD in this study. Many patients had previous myocardial infarction treated with coronary angioplasty. In other words, many patients had previous myocardial infarction but no significant stenosis in the infarct-related artery. Accordingly, fixed defects could probably detect the presence of previous myocardial infarction without a stenosed infarct-related artery. On the other hand, it was possible that an infarct territory with a fixed defect supplied by a stenosed infarct-related artery would be judged as a normal vascular territory. This possibility might result in the low sensitivity of perfusion data for detection of multivessel CAD.
In this study, we assessed coronary artery narrowing visually with coronary arteriography. In the 48% of our patients who had previous coronary angioplasty, visual estimation of coronary stenosis might have been less accurate than in patients with nondilated coronary arteries, thus rendering the assessment of coronary artery narrowing less reliable.
CONCLUSION
Combined assessment of worsening of LV regional wall motion by exercise and perfusion data in exercise 201Tl gated myocardial SPECT was more sensitive, with acceptable specificity, than was assessment of perfusion data alone for detection of multivessel CAD. Worsening of LV regional wall motion by exercise has the potential to indicate multivessel CAD in patients without multivessel patterns of reversible perfusion defects.
Footnotes
Received May 30, 2001; revision accepted Dec. 19, 2001.
For correspondence or reprints contact: Naoya Shirai, MD, Department of Internal Medicine and Cardiology, Osaka City University Graduate School of Medicine, 1-4-3 Asahi-Machi, Abeno-Ku, Osaka, 545-8585, Japan.
E-mail: shirain{at}msic.med.osaka-cu.ac.jp





{kind=link}
{kind=link}
{kind=link}
{kind=link}