


Abstract
The purpose of this study was to compare the results of isotope injection the morning of surgery (1-d protocol) with isotope injection the day before surgery (2-d protocol) in patients having sentinel lymph node (SLN) biopsy for breast cancer. Methods: The 1-d (protocol 1) and 2-d (protocol 2) protocols included 514 and 152 patients, respectively, treated contemporaneously by surgeons experienced with the SLN biopsy technique. All had preoperative lymphoscintigraphy (LSG) and SLN biopsy using both blue dye and 99mTc–sulfur colloid. All patients had a single-site intradermal injection of unfiltered 99mTc–sulfur colloid in 0.05 mL normal saline: 3.7 MBq (0.1 mCi) on the morning of surgery for protocol 1 and 18.5 MBq (0.5 mCi) on the afternoon before surgery for protocol 2. Results: The patients in protocols 1 and 2 were comparable in terms of age, tumor size, tumor location, histologic type, node positivity, and frequency of a previous surgical biopsy. Comparing protocols 1 and 2, early (30 min) LSG images found the SLN equally often (69% vs. 68%). Isotope identified the SLN equally often at surgery (93% vs. 97%) as did isotope plus dye (98% vs. 99%). A comparable number of SLNs was found (2.5 vs. 2.8 per axilla), and the concordance between isotope and dye in the SLN was also comparable (97% vs. 95%). Late LSG images (at 2 h, possible only for protocol 2) identified the SLN in significantly more patients compared with early images (86% vs. 68%). Conclusion: With unfiltered 99mTc–sulfur colloid injected intradermally, the results of SLN biopsy under the 1-d and 2-d protocols are virtually identical. A 2-d protocol allows increased efficiency in scheduling, both for nuclear medicine physicians and for the operating room, with no compromise in the effectiveness of SLN mapping.
The sentinel lymph node (SLN) concept, first proposed for the staging and treatment of penile cancer (1), has proven equally useful for patients with melanoma (2) and, most recently, for those with early-stage breast cancer (3–5). If the SLN, defined as the first regional node (or nodes) receiving lymphatic drainage from a cancer, is benign, then the patient may be spared the morbidity of a conventional lymph node dissection.
In breast cancer, the SLN have been identified using blue dye (4), radiocolloid (3), or a combination of both methods (5). An emerging international consensus, and our own experience (6,7), supports the use of the combined method. Radioisotope SLN mapping and the subsequent surgical excision, as done in the United States, usually involve one trip to the hospital, with the radiopharmaceutical given several hours before surgery. Although SLN localization under this protocol works well, operating room time is often wasted in waiting for patients to arrive from lymphoscintigraphy (LSG). The consequent frustration of the surgeon and time pressure on the nuclear medicine physician may result in the omission of additional images that might reveal unexpected pathways of lymphatic drainage. These delays could be eliminated by earlier isotope injection, and European centers (using 99mTc-albumin colloid, not available in the United States) have had excellent results with injection of the radiopharmaceutical on the day before surgery (8,9). The goal of this study, using the only radiotracer available in the United States (99mTc–sulfur colloid), was to compare the results of same-day and day-before isotope injection in breast cancer patients having SLN biopsy.
MATERIALS AND METHODS
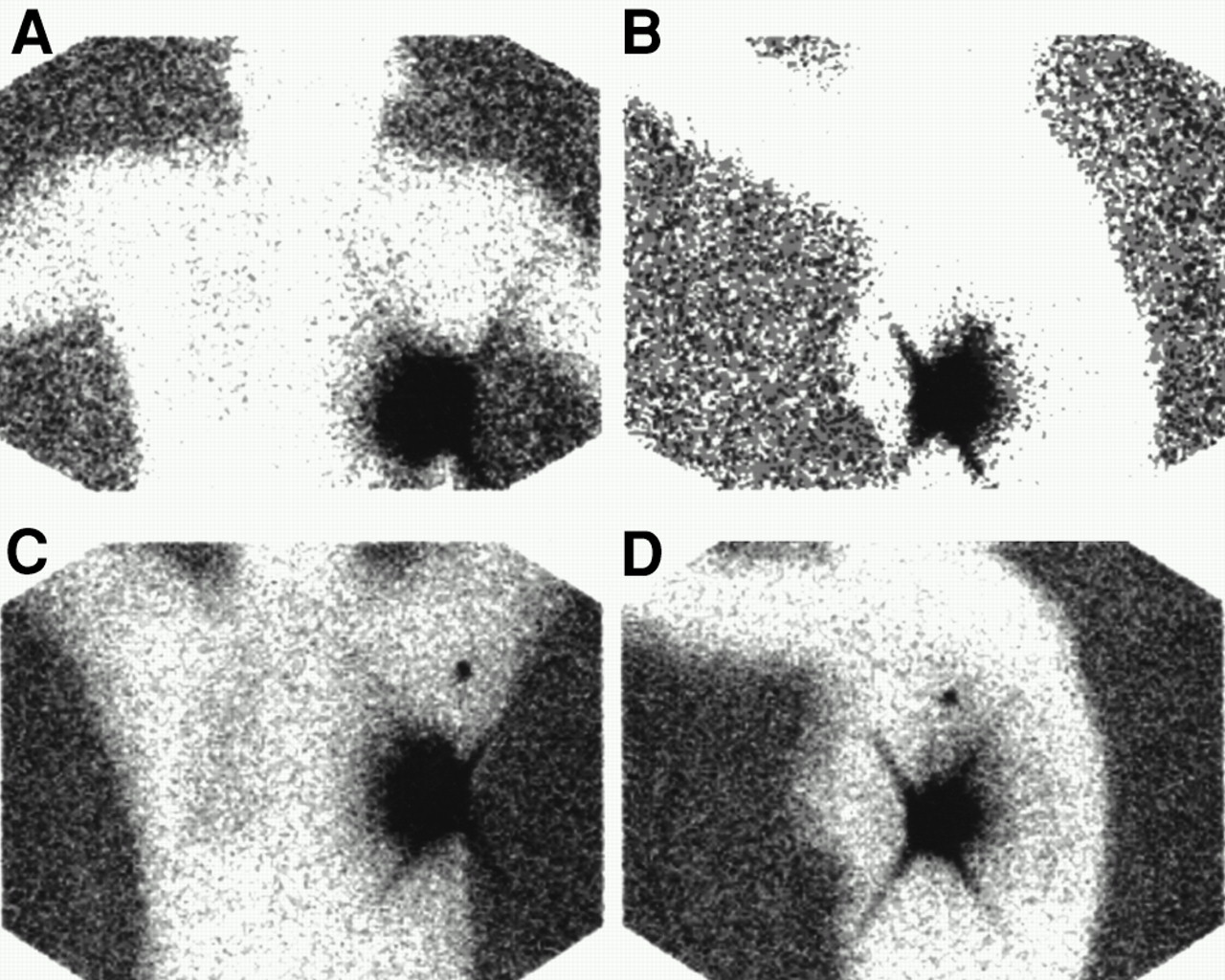
Between February and October 1999, 666 patients had SLN biopsy procedures at our center performed by surgeons who were experienced with the technique (earlier, we had performed 959 SLN biopsy procedures, starting in September 1996). Five hundred fourteen patients had isotope injection the day of surgery (protocol 1) and 152 patients were injected the day before surgery (protocol 2). All had a single-site intradermal injection of unfiltered 99mTc–sulfur colloid (CIS-US, Bedford, MA), given by one of two experienced nuclear medicine physicians, directly over the tumor or just cephalad to the scar of the previous surgical biopsy. The isotope was prepared in-house under strict guidelines to ensure quality control and consistent particle size (10). Patients received 3.7 MBq (0.1 mCi) under protocol 1 and 18.5 MBq (0.5 mCi) under protocol 2 (to allow for radioactive decay overnight). The volume injected was 0.05 mL for both protocols. LSG consisting of anterior and lateral images of the chest and axilla was obtained at 30 min, and protocol 2 patients also had a delayed image at 2 h. A cobalt flood source was used to silhouette the patient during image acquisition, allowing superb localization of the SLN (Fig. 1). Surgery was usually performed about 2 h after injection (protocol 1) or early the following morning (protocol 2).
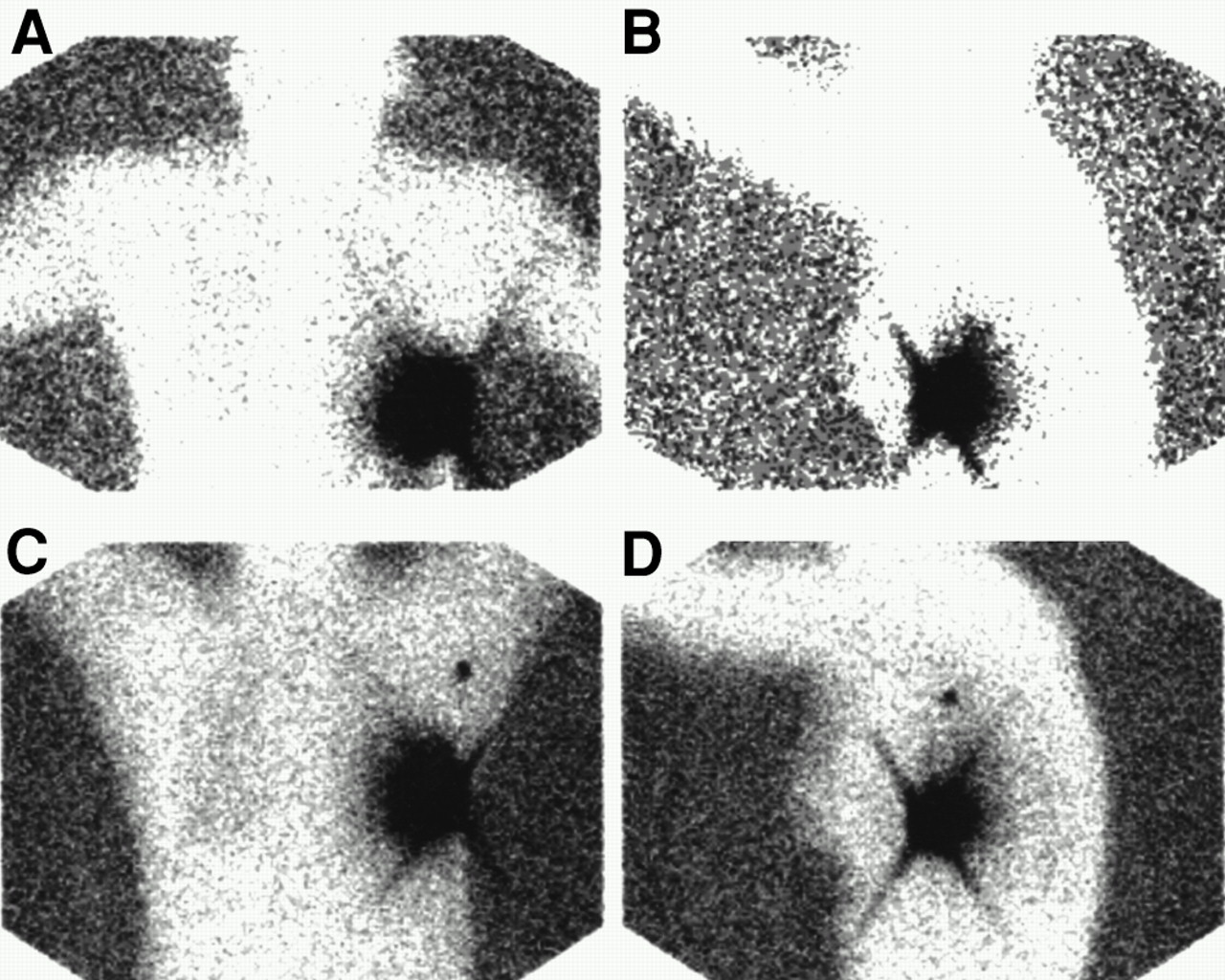
Anterior (A and C) and left lateral (B and D) transmission images show injection site in left breast and focal uptake in sentinel node in left axilla, seen only on 2-h delayed images. (A and B) Early images at 30 min. (C and D) Delayed images at 2 h.
Our operative protocol for SLN biopsy has been described in detail (6,7). Intraparenchymal injection of 4 mL blue dye (Lymphazurin; Zenith Parenterals, Rosemont, IL) was given 5–10 min before axillary dissection. Successful dye localization required finding a blue SLN or a blue lymphatic leading directly to a lymph node. Successful isotope localization required that the ex vivo counts of the SLN (using a handheld γ probe) exceed the postexcision axillary background by at least 4–5 times.
Patients were not randomly assigned to either protocol but were allocated on the basis of their own preference or the feasibility of scheduling the procedures (or both). The success rates of early and late LSG were compared using McNemar’s test. All cases were scored prospectively as dye, isotope, or combined (i.e., dye, isotope, or both) success. These success rates were compared using Fisher’s exact test, and a confidence interval for the ratio of two proportions was also computed. Zelen’s test for homogeneity of the odds ratio (11) examined the effect of surgeon on localization success rates. We used exact statistical analysis methods that do not require similar numbers in treatment groups.
RESULTS
Although patients were not randomized, the patients in protocol 1 and protocol 2 were quite comparable in terms of age, tumor size, histologic type, and tumor location (Table 1). A comparable proportion of patients had positive SLNs (30% vs. 37%; P = 0.13). Of the 205 patients with histologically positive SNLs, 7 (3.4%) were found only by blue dye and 21 (10%) were found only by isotope. One hundred eighty-three patients had conventional lymph node dissection. The other patients either refused further dissection or had positive nodes only by immunohistochemistry, the clinical significance of which is still not known.
Comparison of Patients in Two Protocols
The success of LSG in imaging the SLN on the early images was comparable between the two groups (Table 2). However, the success of LSG in protocol 2 patients increased significantly on the delayed images (from 68% to 86%; P < 0.0001). Figure 1 illustrates a case in which the sentinel node was seen only on the delayed images.
Successful Localization on Lymphoscintigram
Isotope localization of the SLN succeeded in a comparable fraction of protocol 1 and protocol 2 patients (93% vs. 97%; P = 0.21) as did the combined method (98% vs. 99%; Table 3). The ratio of the success rate in the 2-d protocol to the 1-d protocol is 1.019. An exact confidence interval for the ratio is (0.9761, 1.053). Because this is a narrow interval around 1, we conclude that the overall success rate of the 2-d protocol is comparable with that of the 1-d protocol.
Success Rate of Sentinel Node Localization
Comparable numbers of SLNs were obtained in protocol 1 and protocol 2 cases (2.5 vs. 2.8 per axilla). Although we do not have exact data on the dissection time between the two protocols, the consensus among our surgeons is that there is no appreciable time difference despite the slightly higher yield of SNLs in the 2-d protocol.
In those patients in whom both dye and isotope were found in the axilla, there was concordance (i.e., at least one sentinel node contained both dye and isotope) in 95% of the 2-d group and in 97% of the 1-d group (Table 4).
Number of Sentinel Nodes Found
To test for learning curve artifacts, we examined the distribution of SLN procedures by surgeon (Table 5). Most surgeons were highly experienced with SLN biopsy before starting this study. Of note, surgeon A performed the largest proportion of prior, protocol 1, and protocol 2 procedures (36%, 26%, and 47%, respectively). Despite this disproportion, a comparison of surgeon A with the combined results of surgeons B–I showed that the success rate of SLN localization did not differ significantly (P = 1.00; Zelen’s exact test for homogeneity of the odds ratios).
Distribution of Procedures Performed by Surgeons
DISCUSSION
SLN biopsy is rapidly emerging as a new standard of care for the patient with early-stage breast cancer, and radioisotope mapping of the SLN is a major component of the procedure. Using the combination of blue dye and isotope, about 10% of SLNs and 10% of positive SLNs are found by dye or isotope alone (7) and might be missed by reliance on a single method of localization.
Since we began to perform SLN biopsy for breast cancer in September 1996 (6), we have continued to refine our technique of isotope mapping. In a comparison of 220-nm filtered and unfiltered 99mTc–sulfur colloid (10), we found the SLN more often with the unfiltered preparation, we experienced more instances of failure associated with a diffusely hot axilla with the filtered isotope, and we found considerable heterogeneity of particle size in the standard unfiltered preparation. On the basis of these results, we began to do isotope preparation in-house to ensure consistent particle size and have adopted unfiltered isotope as our standard preparation.
Intrigued by reports of successful SLN localization with intradermal (12) and subdermal injection (8) (as opposed to the technique of intraparenchymal injection advocated by Krag (13,14)), we compared intradermal and intraparenchymal injection of isotope in 200 consecutive patients who underwent surgery by a single surgeon (15). All patients had intraparenchymal injection of blue dye. We discovered that the SLNs were found by isotope far more often with intradermal injection than with intraparenchymal injection (97% vs. 78%) and that for a similar proportion of each group (95% and 97%) the same SLN was both blue and hot (i.e., the dermal and parenchymal lymphatics of the breast drained to the same SLN). On the basis of these data, we have made intradermal isotope injection our standard method.
As our volume of SLN biopsy procedures (all with same-day isotope injection) grew, we became increasingly troubled with the difficulty of coordinating the schedules of the nuclear medicine department and the operating room. The nuclear medicine physicians felt increasingly pressured to complete the LSG quickly (omitting delayed films that might have proven useful), and the surgical teams were increasingly frustrated by delays waiting for patients to arrive in the operating room from nuclear medicine. This study, inspired by the success of other centers with LSG done the day before surgery (8,9), grew out of that frustration.
Here we show the striking similarity of results between same-day and day-before isotope injection in two comparable, contemporaneous cohorts of patients, all having SLN biopsy for breast cancer using a mature technique in the hands of experienced surgeons. The most significant difference between the two groups was that day-before isotope injection allowed the time for 2-h images, which substantially improved successful imaging of the SLN (from 68% to 86%). The higher success rate is unlikely to be associated with the higher radioactivity administered because the early image at 30 min carried a success rate that was almost identical with that of the 1-d protocol (68% vs. 69%). For LSG to be successful, delayed imaging of at least 2 h is highly recommended. Delayed imaging may also have the added advantage of revealing unexpected extraaxillary drainage.
We initially shared Morton and Bostick’s concern (16) that over time increasing numbers of axillary nodes, not all of them representing “the true sentinel node,” would take up isotope. This has not proven to be the case, either in our experience (2.5 vs. 2.8 nodes; Table 4) or in that of Winchester et al. (17), whose recent findings are quite comparable with our own. We believe that the 2-d protocol succeeds because beyond a few hours there is little or no significant further migration of colloid particles within the axilla. This is also supported by our data that the concordance between the blue dye and isotope is equally high in both protocols (Table 4) and practically identical to our previous experience (15).
CONCLUSION
SLN mapping using the technique of intradermal injection of unfiltered 99mTc–sulfur colloid yields comparable results whether injected on the same day or the day before surgery. SLNs were successfully identified in 98%–99% of patients with the combination of isotope and blue dye. Because of the delayed time of imaging, LSG revealed the SLN more successfully with the day-before injection. The scheduling of SLN biopsy procedures can be flexible and within a 24-h period need not take the time of isotope injection into account.
Footnotes
Received Apr. 6, 2000; revision accepted Nov. 7, 2000.
For correspondence or reprints contact: Henry W.D. Yeung, MD, Nuclear Medicine Service, Memorial Sloan-Kettering Cancer Center, 1275 York Ave., New York, NY 10021.
REFERENCES
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Organ and Fetal Absorbed Dose Estimates from 99mTc-Sulfur Colloid Lymphoscintigraphy and Sentinel Node Localization in Breast Cancer Patients
- Fusion of SPECT and Multidetector CT Images for Accurate Localization of Pelvic Sentinel Lymph Nodes in Prostate Cancer Patients
- Reverse echelon node and a lymphatic ectasia in the same patient during breast lymphoscintigraphy: the importance of injection and imaging technique
- Patient effective dose from sentinel lymph node lymphoscintigraphy in breast cancer: a study using a female humanoid phantom and thermoluminescent dosemeters
- Radioguided Sentinel Lymph Node Biopsy in Breast Cancer Surgery