


Abstract
The aims of this study were (a) to compare absolute myocardial blood flow (MBF) during adenosine triphosphate (ATP) infusion with that after dipyridamole administration without caffeine intake and (b) to evaluate the effect of caffeine intake on the hyperemic flow induced by these coronary vasodilator agents. Methods: MBF was quantified with 15O-labeled water and PET at rest, during ATP infusion (0.16 mg/kg/min for 9 min), and after dipyridamole administration (0.56 mg/kg over 4 min) after a 24-h abstinence from caffeine (baseline evaluation) in 10 healthy volunteers. Within 2 wk, the same PET studies were repeated after caffeine intake to evaluate the effect of caffeine on the hyperemic flow induced by these pharmacologic agents (caffeine study). Myocardial flow reserve (MFR), defined as the ratio of hyperemic to resting blood flow, was also evaluated. Results: Resting MBF in baseline and caffeine studies did not differ significantly (0.79 ± 0.29 vs. 0.75 ± 0.31 mL/min/g, P = 0.88). Without caffeine intake, MBF during ATP infusion was significantly higher than that after dipyridamole administration (3.70 ± 0.67 vs. 3.00 ± 0.79 mL/min/g, P = 0.003), whereas there was no significant difference in MFR between ATP and dipyridamole stress (5.15 ± 1.64 vs. 4.11 ± 1.44, P = 0.07). After caffeine intake, the hyperemic flows induced by ATP and dipyridamole were not significantly different (1.68 ± 0.37 vs. 1.52 ± 0.40 mL/min/g, P = 0.50). MFR estimated by ATP and dipyridamole also did not differ significantly in the caffeine studies (2.44 ± 0.88 vs. 2.25 ± 0.94, P = 0.73). MBF during ATP infusion and after dipyridamole administration were significantly lower in the caffeine studies than that in the baseline evaluation (1.68 ± 0.37 vs. 3.70 ± 0.67 mL/min/g, P < 0.0001, and 1.52 ± 0.40 vs. 3.00 ± 0.79 mL/min/g, P < 0.0001, respectively). Conclusion: This study demonstrates that ATP has the potential to induce greater hyperemia than dipyridamole, whereas hyperemic responses to ATP and dipyridamole are similarly attenuated after caffeine intake. These findings suggest that abstinence from caffeine before ATP stress testing may be needed.
Dipyridamole has been successfully used for coronary flow reserve (CFR) measurements (1,2) and for noninvasive diagnosis of coronary artery disease (CAD) (3,4). Recently, adenosine triphosphate (ATP) has been increasingly used as an alternative agent for pharmacologic stress imaging. It has been reported that ATP has a diagnostic value similar to that of dipyridamole for myocardial perfusion scintigraphy in patients with CAD (5,6). However, few data are available on the magnitude of the hyperemia produced by intravenous infusion of ATP in comparison with dipyridamole in humans (6). In this regard, PET has important advantages over SPECT, because it can objectively evaluate hyperemia induced by ATP compared with that induced by dipyridamole in the absolute term. In addition, 15O-labeled water (H215O) has a short half-life (2 min) that can be used for serial measurements of these pharmacologic stresses.
It is known that the coronary vasodilator effect of adenosine or dipyridamole is inhibited by methylxanthine compounds such as theophylline (7) or caffeine (7–9). It is common practice to request caffeine abstinence for 12–24 h before the performance of dipyridamole myocardial perfusion scintigraphy. ATP is a precursor of adenosine and, therefore, its hyperemic effect is thought to be dependent on its degradation product, adenosine. In addition, it has also been suggested that ATP has a coronary vasodilator effect independent of adenosine through different mechanisms (10–12). However, to our knowledge, the hyperemic effect of ATP under the influence of caffeine has not been investigated yet.
Therefore, the aims of this study were (a) to compare absolute myocardial blood flow (MBF) during ATP infusion with that after dipyridamole administration without caffeine intake and (b) to evaluate the effect of caffeine intake on the hyperemic flow induced by these coronary vasodilator agents.
MATERIALS AND METHODS
Subjects
Ten healthy male volunteers (age range, 20–39 y; mean age, 31 ± 6 y), without a history of cardiac disease, hypertension, diabetes, hypercholesterolemia, and habitual smoking, were studied. All had a normal electrocardiogram (ECG) at rest and during the ATP and dipyridamole studies. None of the volunteers was on any medication before or at the time of the myocardial flow measurements. All volunteers were asked to abstain from caffeine-containing products for a minimum of 24 h before the testing. Each subject gave written informed consent as approved by the Kyoto University Ethics Committee.
Study Protocol
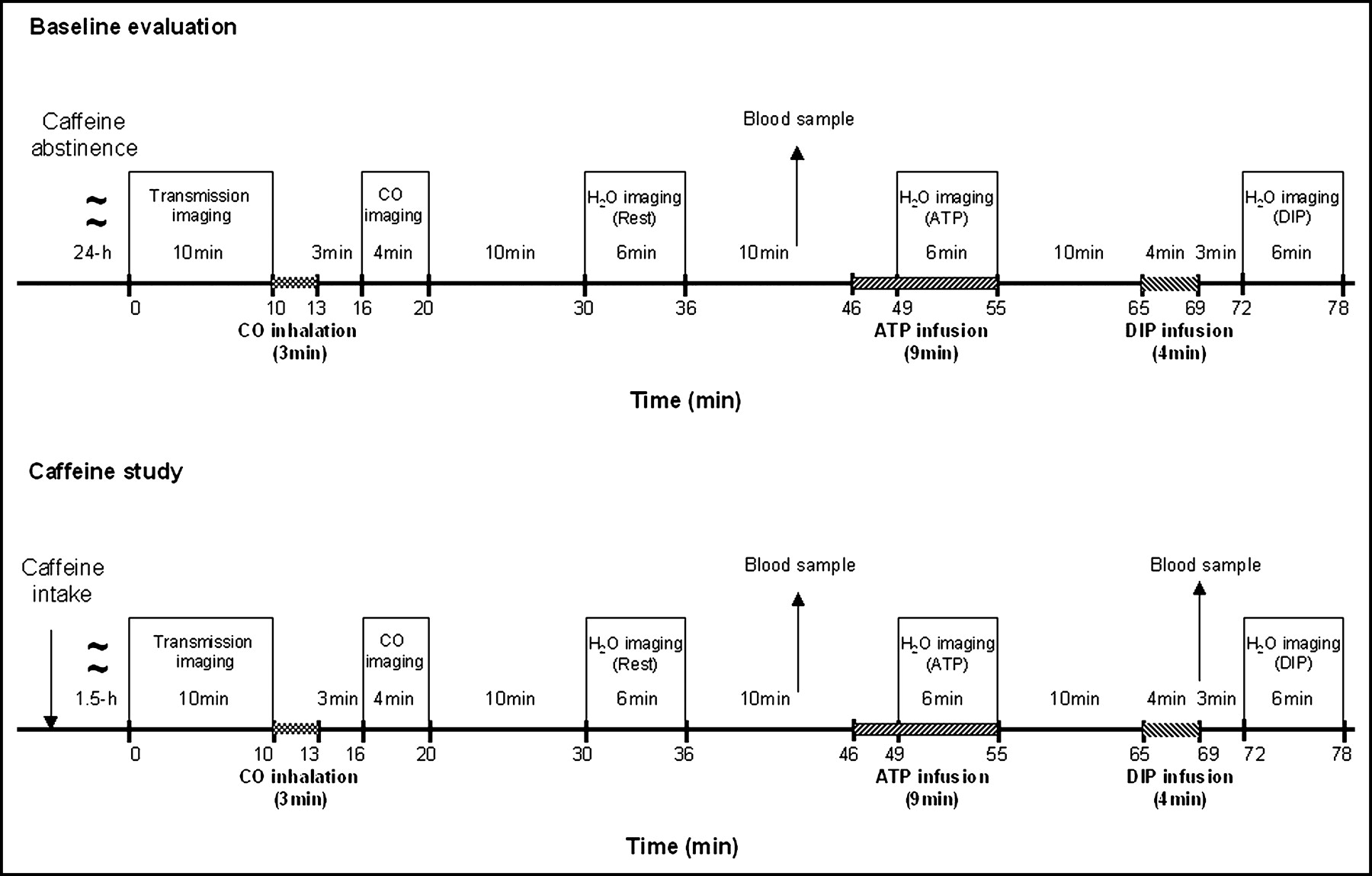
The 10 healthy volunteers were studied by dynamic PET and intravenous infusion of H215O at rest, during intravenous ATP infusion, and after dipyridamole administration after a 24-h abstinence from caffeine (baseline evaluation) (Fig. 1A). Within 2 wk, the same studies were repeated after caffeine intake (caffeine study) (Fig. 1B). The caffeine study was performed 1.5 h after oral intake of 3 mg/kg of caffeine (Cafferop; Daiichi Pharma Corp.), which is comparable to the quantity in 2–3 cups of coffee (13,14).
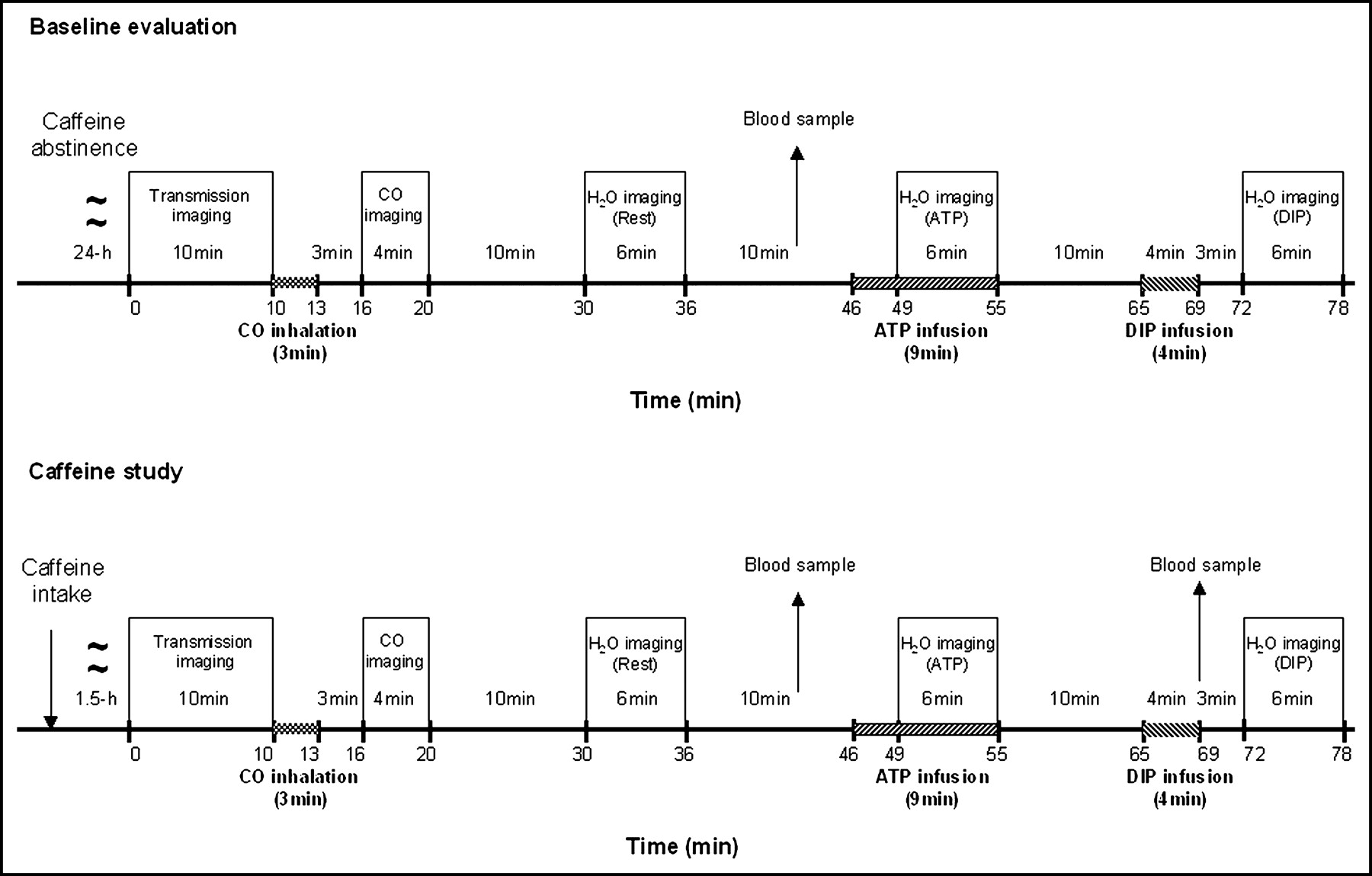
Study protocol. DIP = dipyridamole.
Image Acquisition
Two catheters were inserted: one in the antecubital vein of the right hand for injection of H215O and one in the antecubital vein of the left hand for injection of ATP and dipyridamole and to draw a blood sample. Each subject was positioned in the gantry of the PET camera (Advance; General Electric Medical Systems) with the aid of ultrasound. The spatial resolution of the reconstructed clinical PET images was ∼8-mm full width at half maximum at the center of the field of view, and the axial resolution was ∼4 mm (15). The subjects lay supine in the PET scanner with their arms out of the field of view. A 10-min transmission scan using 2 rotating 68Ge pin sources was obtained for the attenuation correction. After a transmission, subjects were asked to inhale 15O-labeled carbon monoxide (C15O) for 2 min. After inhalation, C15O was allowed to combine with hemoglobin in the red blood cells for 3 min before a 4-min static scan was started. During the scan period, 3 blood samples were drawn at 2-min intervals and the radioactivity was measured. In the resting condition, ∼740 MBq H215O were injected intravenously over 2 min, and a 20-frame dynamic PET scan was performed for 6 min. Ten minutes later, after physical decay of the 15O activity to nearly undetectable levels, ATP was infused intravenously for 9 min at a constant rate of 0.16 mg/kg/min (5,6). Three minutes after the start of the ATP infusion, H215O was administered again and a second set of dynamic PET images was acquired. Ten minutes after the end of the ATP administration, dipyridamole was infused intravenously at a rate of 0.56 mg/kg over 4 min. Three minutes after the end of the dipyridamole infusion, a third dose of H215O was administered with acquisition of dynamic PET images. Heart rate, blood pressure, and ECGs were monitored continuously during the PET studies. Each subject was carefully monitored and questioned during and after termination of infusion of the pharmacologic agent to determine any occurrence of adverse events. Aminophylline was available during the study.
Image Processing
The acquisition sequences of the H215O dynamic images were 6 frames of 5 s each, followed by 6 frames of 15 s each and 8 frames of 30 s. All data were corrected for dead time, decay, and photon attenuation. The PET images, including transmission images, C15O images, and H215O dynamic images, were reoriented into short-axis planes. Myocardial regions of interest (ROIs) were drawn on the 3 or 4 short-axis slices covering the whole wall of the left ventricle. To enhance the accuracy and statistical significance of the flow measurements, the average blood flow of the global myocardium was calculated and used for further analysis. The arterial input function was obtained from the left ventricular time–activity curve using a validated method in which corrections were made for the limited recovery of the left ventricular ROI and the spillover from the myocardial activities (16).
MBF, Myocardial Flow Reserve (MFR), and Coronary Vascular Resistance (CVR)
Values of MBF (mL/min/g) were calculated according to a previously published method using the single-compartment model, which is theoretically free from partial-volume effects or wall motion (16–18). The investigator was unaware of which of the 2 PET studies was being interpreted (ATP or dipyridamole, caffeine or no caffeine). MFR was calculated as the ratio of stimulated flow to resting flow. To account for interindividual differences in the flow response to caffeine, resting MBF was normalized to the rate–pressure product as an index of cardiac workload. Normalized MBF was derived from the ratio of blood flow (mL/min/g) to the rate–pressure product (mm Hg × beats/min) × 10,000 (19). The subject variability measurement of MBF, which was determined by the SD divided by the MBF (mL/min/g), was compared between ATP and dipyridamole stress MBF in the baseline evaluation. An index of CVR was derived from the ratio of mean arterial blood pressure (mm Hg) to MBF (mL/min/g).
Analysis of Plasma Caffeine Concentrations
Venous blood samples were drawn at the beginning of the ATP H215O dynamic study in the baseline evaluation (Fig. 1) and at the beginning of each pharmacologic H215O dynamic study in the caffeine studies (Fig. 1). Plasma caffeine concentrations were determined using a standard high-performance liquid chromatography method (20).
Statistical Analysis
Statistical analysis was performed with a commercially available personal computer software program (StatView-J 5.0; SAS Institute Inc.). Values are expressed as the mean ± SD. Statistical analysis of the hyperemic response, hemodynamic data, and the plasma caffeine concentrations was performed by 1-way repeated-measures ANOVA followed by the Bonferroni test. The Fisher exact probability test was used to compare the frequency of adverse events during ATP or dipyridamole stress testing. Correlations were sought using least-squares analysis. Probability values < 0.05 were considered statistically significant.
RESULTS
Hemodynamic Findings
The hemodynamic findings at rest, during ATP infusion, and after dipyridamole administration are shown in Table 1. At rest, there were no significant differences in any of the hemodynamic data between baseline and caffeine studies (Table 1). In the baseline evaluation, the heart rate significantly increased during ATP infusion (P < 0.001) and after dipyridamole administration (P < 0.001) (Table 1) and was significantly higher after dipyridamole administration than during ATP infusion (99 ± 12 vs. 88 ± 12 beats/min, P = 0.02). However, the increase in heart rate during ATP infusion and after dipyridamole administration was blunted after caffeine intake.
Comparison of Hemodynamic Variables at Rest and During Pharmacologic Vasodilation in Baseline Evaluation and Caffeine Studies
In the baseline evaluation, the rate–pressure product significantly increased during ATP infusion (P < 0.001) and after dipyridamole administration (P < 0.0001) (Table 1) and was significantly higher after dipyridamole administration than during ATP infusion (10,119 ± 1,776 vs. 8,763 ± 1,732 mm Hg × beats/min, P = 0.04). In the caffeine studies, the rate–pressure product significantly increased during ATP infusion (P = 0.01) and after dipyridamole administration (P = 0.001) (Table 1), whereas there was no significant difference between during ATP infusion and after dipyridamole administration (8,266 ± 1,420 vs. 8,795 ± 1,074 mm Hg × beats/min, P = 0.41).
MBF and MFR
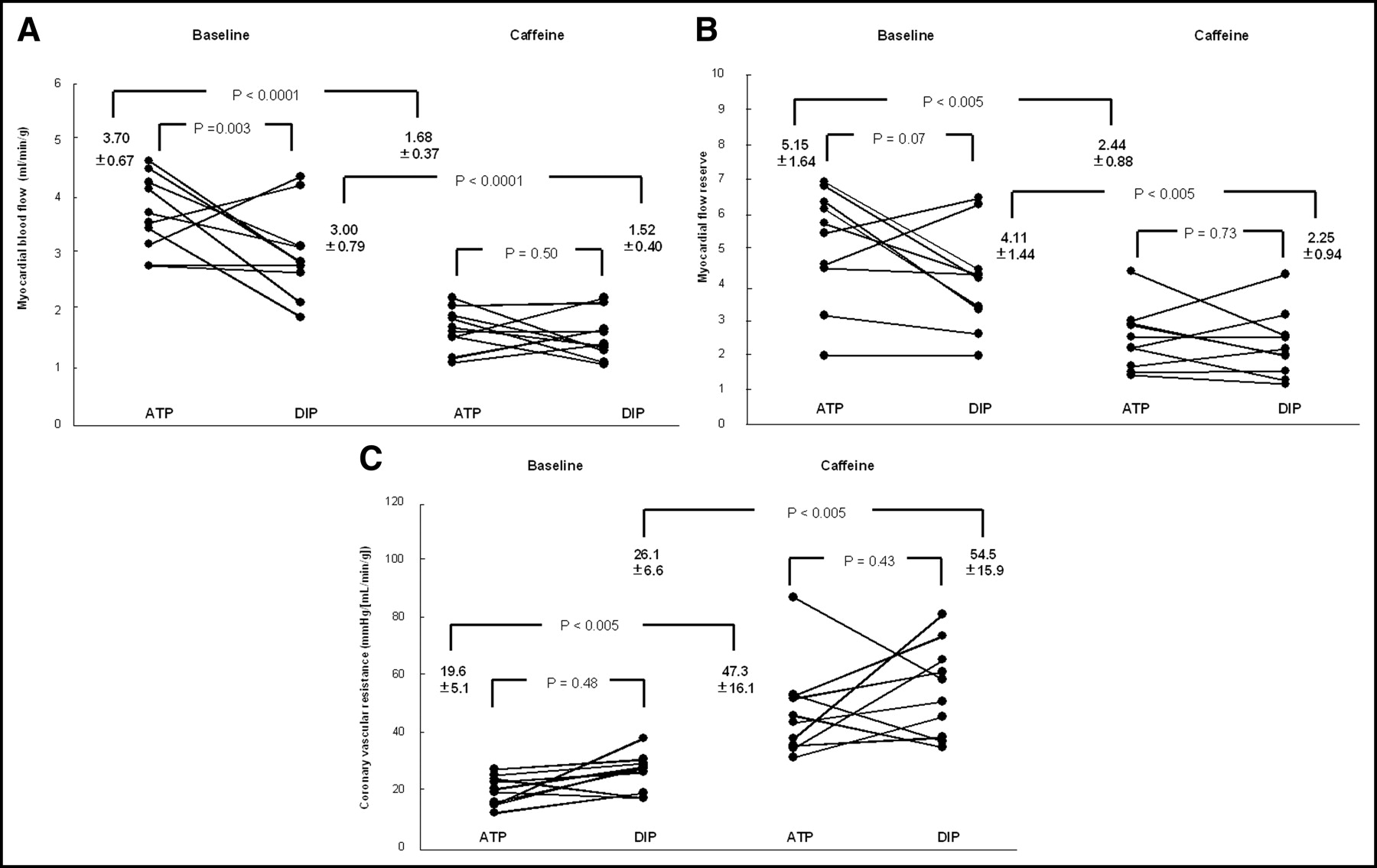
The individual measurements of blood flow and flow reserve are listed in Table 2. At rest, there was no significant difference in MBF between the baseline and caffeine studies (0.79 ± 0.29 vs. 0.75 ± 0.31 mL/min/g, P = 0.88). Normalized MBF was also similar in the baseline and caffeine studies (1.23 ± 0.39 vs. 1.18 ± 0.53 mL/min/g/[mm Hg × beats/min], P = 0.56). In the baseline evaluation, MBF significantly increased during ATP infusion (P < 0.0001) and after dipyridamole administration (P < 0.0001) (Table 2) and was significantly higher during ATP infusion than that after dipyridamole administration (3.70 ± 0.67 vs. 3.00 ± 0.79 mL/min/g, P = 0.003, Fig. 2A). However, there was no significant difference in MFR between ATP and dipyridamole (5.15 ± 1.64 vs. 4.11 ± 1.44, P = 0.07, Fig. 2B). After caffeine intake, MBF induced by ATP and dipyridamole was not significantly different (1.68 ± 0.37 vs. 1.52 ± 0.40 mL/min/g, P = 0.50, Fig. 2A). MFR estimated by ATP and dipyridamole was also similar (2.44 ± 0.88 vs. 2.25 ± 0.94, P = 0.73, Fig. 2B). MBF during ATP infusion and after dipyridamole administration was significantly lower in the caffeine studies than that in the baseline evaluation (1.68 ± 0.37 vs. 3.70 ± 0.67 mL/min/g, P < 0.0001, and 1.52 ± 0.40 vs. 3.00 ± 0.79 mL/min/g, P < 0.0001, Fig. 2A). Furthermore, MFR estimated by ATP and dipyridamole was significantly lower in the caffeine studies than that in the baseline evaluation (2.44 ± 0.88 vs. 5.15 ± 1.64, P < 0.005, and 2.25 ± 0.94 vs. 4.11 ± 1.44, P < 0.005, respectively, Fig. 2B).
Comparison of MBF, MFR, and CVR at Rest and During Pharmacologic Vasodilation in Baseline Evaluation and Caffeine Studies

(A) MBF during ATP infusion and after dipyridamole administration in baseline evaluation (left) and in caffeine studies (right). (B) MFR estimated by ATP and dipyridamole in baseline evaluation (left) and in caffeine studies (right). (C) CVR during ATP infusion and after dipyridamole administration in baseline evaluation (left) and in caffeine studies (right). DIP = dipyridamole.
The subject variability measurement was lower during ATP infusion than that after dipyridamole administration in the baseline evaluation (0.18 vs. 0.26).
CVR Index
The individual measurements of CVR are listed in Table 2. At rest, this index did not differ between baseline evaluation and caffeine studies (100.3 ± 25.7 vs. 110.9 ± 35.5 mm Hg/[mL/min/g], P = 0.25). In the baseline evaluation, there was no significant difference in CVR between ATP and dipyridamole (19.6 ± 5.1 vs. 26.1 ± 6.6, P = 0.48, Fig. 2C). The CVR during ATP infusion and after dipyridamole administration were significantly higher in the caffeine studies than that in the baseline evaluation (47.3 ± 16.1 vs. 19.6 ± 5.1 mm Hg/[mL/min/g], P < 0.005, and 54.5 ± 15.9 vs. 26.1 ± 6.6 mm Hg/[mL/min/g], P < 0.005, respectively, Fig. 2C).
Relation Between Plasma Caffeine Concentrations and Hyperemic Blood Flows
MBF induced by ATP and dipyridamole was inversely correlated with plasma caffeine concentrations (y = −0.46x + 3.44, r = 0.73, P = 0.0002, Fig. 3A, and y = −0.36x + 2.89, r = 0.68, P = 0.001, Fig. 3B, respectively)
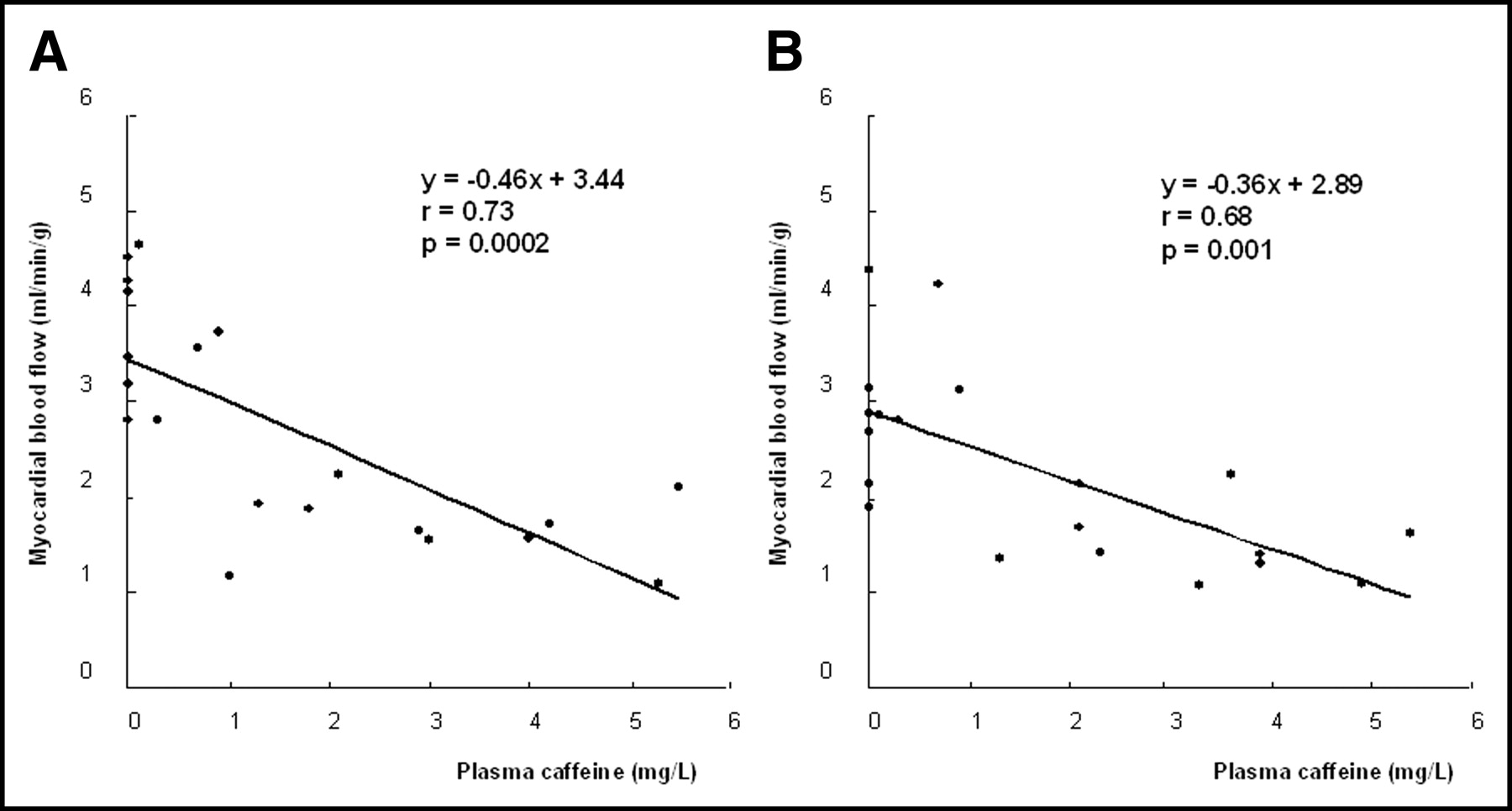
MBF during ATP infusion (A) and after dipyridamole administration (B) was inversely correlated with plasma caffeine concentrations.
Furthermore, MFR estimated by ATP and dipyridamole was also inversely correlated with plasma caffeine concentrations (y = −0.71x + 4.37, r = 0.72, P = 0.003, Fig. 4A, and y = −0.67x + 3.88, r = 0.56, P = 0.010, Fig. 4B, respectively).

MFR estimated by ATP (A) and dipyridamole (B) was inversely correlated with plasma caffeine concentrations.
Adverse Events
None of the subjects reported any major adverse reactions (chest pain, heart block, or acute asthmatic attack). In the baseline evaluation, 6 subjects had minor adverse events during ATP infusion, including dyspnea (n = 4), epigastrial discomfort (n = 1), flushing (n = 6), and stomachache (n = 2). After dipyridamole administration, 5 subjects had minor adverse events, including dyspnea (n = 2), flushing (n = 1), headache (n = 1), palpitation (n = 3), and stomachache (n = 2) (P = 0.65). After caffeine intake, the incidences were observed only in 2 subjects during ATP infusion and in 1 subject after dipyridamole infusion (P = 0.53).
Plasma Caffeine Concentrations
The plasma caffeine concentrations for each subject are listed in Table 3. In the baseline evaluation, detectable plasma caffeine concentrations were found in 4 subjects and ranged from 0.1 to 0.9 mg/L. In the remaining 6 subjects whose levels were below the level of detection (<0.1 mg/L), the plasma caffeine concentrations were dealt with the same as those of 0 mg/L. The mean plasma caffeine concentration in the baseline evaluation was significantly lower than that in the caffeine studies (0.2 ± 0.3 mg/L, P < 0.0001, vs. the ATP and dipyridamole studies after caffeine intake). For the caffeine studies, the plasma caffeine concentrations ranged from 1.0 to 5.5 mg/L, and there was no significant difference between the ATP and dipyridamole studies (3.1 ± 1.6 vs. 3.3 ± 1.3 mg/L, P = 0.76).
Plasma Caffeine Concentrations (mg/L)
DISCUSSION
To our knowledge, this is the first study to evaluate the absolute MBF with ATP compared with dipyridamole in the same subject. At the standard doses, ATP seems to be more potent than dipyridamole in producing hyperemia. However, both ATP- and dipyridamole-induced hyperemic effects were similarly blunted by caffeine intake. These findings suggest that abstinence from caffeine before ATP stress testing may be needed.
Effect of ATP Versus Dipyridamole on MBF
One possible explanation for the higher MBF during ATP infusion than that after dipyridamole administration may be the different vasodilator action induced by adenosine for the increase in adenosine concentration in the myocardium or arterial wall. Dipyridamole increases the level of circulating adenosine by inhibiting phosphodiesterase, activating adenylate cyclase, and preventing its cellular reuptake (8,21). Therefore, dipyridamole induces the vasodilator effect indirectly. It is known that the degree of dipyridamole-induced vasodilation at a standard dose is sometimes submaximal (21) and varies among subjects (5). In contrast, the hyperemic effect of ATP depends on adenosine, which induces the vasodilator effect directly (5,6,22,23). Chan et al. (22) documented that dipyridamole and adenosine produce similar levels of hyperemia, despite adenosine having a direct-acting coronary vasodilator effect. Wilson et al. (24) demonstrated that a fraction of intravenous infusion of adenosine is metabolized during its transit from the peripheral venous infusion site to the myocardium, because of its very short half-life (<2 s). ATP has a longer half-life (<20 s) than that of adenosine, because it is metabolized into adenosine diphosphate, adenosine monophosphate, and, eventually, adenosine (5,21). In addition, all components from ATP to adenosine are metabolically active (23). Jeremias et al. (23) suggested that intravenous infusion of ATP can produce a higher concentration of adenosine in the coronary circulation than intravenous infusion of adenosine itself. A Doppler guide wire measurement showed that the CFR with ATP tended to be higher than that with dipyridamole (6) or with adenosine (21), which is in good agreement with our results. However, they only provided the values of the average peak velocity in coronary arteries. We believe that this study is the first to compare absolute MBF during ATP infusion and after dipyridamole administration in healthy subjects.
In addition, in this study, the subject variability measurement was lower during ATP infusion than that after dipyridamole administration without caffeine intake (0.18 vs. 0.26), which indicates that ATP produces more stable hyperemia than dipyridamole.
The dose of ATP was determined on the basis of previous reports (5,6) and the dose of dipyridamole was also chosen according to other reports (4,25,26). These doses are widely used in clinical settings. It has been reported that the magnitude of hyperemia is not significantly changed from standard doses to high doses of ATP (6) and of dipyridamole (26). Therefore, despite the fact that only a single dose of ATP and of dipyridamole was given in this study, we believe that the current results are not significantly related to the dose of ATP or of dipyridamole.
Mechanism of Dipyridamole- and ATP-Induced Vasodilation and Caffeine Effect on Pharmacologic Stress-Induced Hyperemia
The dipyridamole-induced hyperemic response is mediated via accumulation of adenosine and stimulation of purine receptors (A2 membrane adenosine receptors). Theophylline and caffeine are competitive adenosine antagonists (7,8,20,27). Bottcher et al. demonstrated that caffeine reduces dipyridamole-induced hyperemia in a dose-dependent fashion (8), which is consistent with our results. In canine and human studies, it has been reported that ATP itself and its degradation product, adenosine diphosphate, contribute to coronary vasodilation mediated by other purine receptors (P2Y receptors) (10–12,27,28). Thus, ATP has a theoretically independent coronary vasodilator effect of adenosine through different mechanisms. In our study, however, ATP-induced hyperemia was inversely correlated with plasma caffeine levels. This finding indicates that adenosine may play an important role in producing hyperemia during ATP infusion.
The average caffeine consumption by adult humans varies among different cultures and nations from 80 to 400 mg per person per day (29). Accordingly, we selected the average amount of caffeine—a dose of 3 mg/kg caffeine—that is reportedly comparable to the quantity in 2–3 cups of coffee (13,14).
The plasma caffeine half-life for healthy subjects is reportedly 4.9–5.7 h (30), and most subjects had caffeine levels of <1 mg/L after a 24-h abstinence from caffeine (9), which is consistent with our results. In the current study, a significantly higher MBF was observed in the baseline evaluation compared with that in the caffeine study. Therefore, abstinence from caffeine-containing products 24 h before diagnostic dipyridamole- or ATP-induced stress testing may be recommended.
Clinical Implications
Although absolute MBF during ATP infusion was significantly higher than that after dipyridamole administration, our results do not necessarily indicate the diagnostic superiority of ATP for SPECT studies because radionuclide myocardial perfusion tracer extraction reaches a plateau at submaximal flow rates. Thus, the achievement of maximal increases in MBF may not be important in the SPECT studies.
In this study, we did not compare MBF between ATP and adenosine because adenosine is not approved for clinical usage in Japan. However, the fact that adenosine produces more consistent and potent coronary dilatation at clinically used doses in comparison with dipyridamole has been appreciated for many years (31). The rapid onset of action and elimination of adenosine compared with dipyridamole reduces the time needed to perform studies. Despite its higher frequency of side effects (32), patients preferred adenosine stress testing compared with dipyridamole stress testing, mainly because of the short duration of side effects (22).
ATP is less expensive and has a lower rate of side effects, including the incidence of atrioventricular block, than adenosine (5). With these advantages over adenosine, ATP may be comparable to adenosine as a routine clinical agent.
Limitations of Study
Our study had some limitations. First, the order of drug administration was not varied in a random way. However, the order, in which the dipyridamole scans were performed before ATP scans, was actually impractical. Because dipyridamole has a much longer half-life than that of ATP, it would interfere with the action of ATP for a few hours. In addition, because plasma caffeine is metabolized over time, it would be difficult to maintain constant plasma caffeine concentrations between ATP and dipyridamole PET scans in the caffeine studies.
Second, only healthy volunteers were enrolled in this study. Thus, whether the same results can be extrapolated to patients with CAD remains to be shown.
Third, because a small number of subjects was enrolled in this study, the results should be confirmed in a larger population. In addition, the repeatability of ATP-induced hyperemic myocardial flows as assessed by PET imaging was not determined. Variability of hyperemic MBF in the individual is also suggested. Therefore, further studies are required for confirmation of this study.
CONCLUSION
The current results suggest that ATP has a potential of producing greater hyperemia than does dipyridamole. After caffeine intake, the hyperemia induced by these 2 agents was similarly blunted. These findings suggest that abstinence from caffeine before ATP stress testing may be needed.
Footnotes
Received Oct. 8, 2003; revision accepted Dec. 4, 2003.
For correspondence or reprints contact: Shigeto Kubo, MD, PhD, Department of Nuclear Medicine and Diagnostic Imaging, Kyoto University Graduate School of Medicine, 54 Shogoin Kawahara, Sakyo-ku, Kyoto, 606-8507, Japan.
E-mail: kub{at}kuhp.kyoto-u.ac.jp
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Sex Differences and Caffeine Impact in Adenosine-Induced Hyperemia
- Dose-Dependent Effect of Caffeine on Adenosine-Induced Myocardial Stress Perfusion in Rubidium-82 Positron-Emission Tomography/Computed Tomography
- Clinical Quantification of Myocardial Blood Flow Using PET: Joint Position Paper of the SNMMI Cardiovascular Council and the ASNC
- Effect of Caffeine on Ischemia Detection by Adenosine Single-Photon Emission Computed Tomography Perfusion Imaging