


Abstract
Plasma brain natriuretic peptide (BNP) level and cardiac autonomic function are closely related to prognosis in patients with heart failure. However, their correlation and incremental prognostic values in human heart failure are unclear. We sought to evaluate the correlation between BNP level and cardiac sympathetic innervation assessed by 123I-metaiodobenzylguanidine (123I-MIBG) and the prognostic value of combined assessment of risk factors for mortality in patients with heart failure. Methods: After conventional examinations and measurements of plasma BNP level and heart-to-mediastinum ratio (HMR) of cardiac 123I-MIBG activity, 158 patients with heart failure were prospectively followed with an endpoint of cardiac death for 16 mo. Results: Fifteen deaths due to pump failure and 2 sudden cardiac deaths were documented. Plasma BNP level correlated with HMR significantly but not so tightly (r = 0.330, P < 0.0001). Univariate analysis identified plasma BNP level, HMR, chronic renal dysfunction, diabetes mellitus, age, and use of nitrates as significant predictors of fatal pump failure, and multivariate Cox analysis showed that plasma BNP level was the most powerful predictor of cardiac death. Patients with both plasma BNP level of ≥172 pg/mL and late HMR of ≤1.74 had a greater annual rate of fatal pump failure than did those without (17.5%/y vs. 0%–3.9%/y, respectively). The hazard ratio of plasma BNP level (7.2) or cardiac 123I-MIBG activity (10.1) increased to 34.4 when both variables were used, and prevalence of fatal pump failure significantly increased from 22% to 62.5% when diabetes mellitus and chronic renal dysfunction were present with a higher plasma BNP level and low cardiac 123I-MIBG activity. Conclusion: Plasma BNP level is a stronger predictor than other risk factors for mortality in heart failure patients and is statistically significantly, but roughly, related to cardiac sympathetic nerve innervation. Impaired cardiac sympathetic nerve innervation and the presence of diabetes mellitus and chronic renal dysfunction, however, improve risk stratification of patients with heart failure and increased plasma BNP concentration.
- heart failure
- natriuretic peptides
- sympathetic nervous system
- prognosis
- diabetes mellitus
- renal dysfunction
Although treatment with angiotensin-converting enzyme (ACE) inhibitors, angiotensin II receptor blockers (ARBs), or β-blockers has recently been established as a standard drug treatment for improving survival of patients with heart failure, the efficacy of this treatment appears to be limited, even in selected patients with heart failure: The overall reduction in mortality rate is estimated to be only 30%–40%. New approaches to further risk stratification of patients undergoing contemporary drug treatment who are at greater risk for cardiac death are, therefore, needed. Brain natriuretic peptide (BNP) is a powerful predictor of clinical outcomes and is a better marker of efficacy of drug treatment in patients with heart failure than are other neurohumoral factors and conventional clinical markers (1–4). Long-term prognosis of patients with heart failure is affected by various noncardiac background factors such as renal dysfunction (5), diabetes mellitus (6), and hypertension (7). On the other hand, it is well known that central and peripheral sympathetic nervous systems are augmented in patients with failing hearts, whereas myocardial content of norepinephrine is impaired. Cardiac sympathetic function per se has also been shown to have pathophysiologic and prognostic implications (6,8–13). We have characterized potent and incremental prognostic values of cardiac sympathetic function assessed by 123I-metaiodobenzylguanidine (123I-MIBG) in human heart failure (12,13). It is thought that sympathoinhibitory actions of natriuretic peptides directly or indirectly retrain sympathetic nervous system outflow in the myocardium as well as in peripheral tissues. Despite the clinical implications of BNP and cardiac sympathetic activity in patients with heart failure, their correlation has not been determined, and incremental prognostic values of BNP on top of other determinants of clinical outcome, including cardiac autonomic function and noncardiac diseases, have not been fully investigated.
This prospective study was designed to determine the correlation between plasma BNP concentration and cardiac sympathetic nerve function and the prognostic value of plasma BNP concentration in patients with heart failure under current medical treatment as well as to determine whether combined assessment of these indices and other diseased states, if identified, enables better risk stratification for identification of patients at greater risk for cardiac death.
MATERIALS AND METHODS
Patient Population and Study Protocol
One hundred fifty-eight consecutive patients with congestive heart failure of New York Heart Association (NYHA) functional classes II–IV at entry (between 1999 and 2001) were enrolled. The entry criteria for this study were as follows: (a) recent documentation of symptomatic heart failure, including easy fatigability, exertional dyspnea, palpitation and orthpnea, accompanying jugular vein dilatation, moist rales, S3 gallop, peripheral edema, and pulmonary congestion or cardiomegaly on a chest radiograph; (b) measurement of plasma BNP level and cardiac MIBG scintigraphy having been performed on the same day or within a few days’ interval, after congestive heart failure had been stabilized by appropriate medical therapy as recommended in recent guidelines (14); (c) standard cardiac function tests using 2-dimensional echocardiography and radionuclide techniques having been performed within 1 wk after 123I-MIBG imaging under stable general conditions before discharge; (d) no indication for an invasive therapeutic procedure, except for the use of an implantable cardioverter defibrillator (ICD) during the period of hospitalization; and (e) informed consent for participation in the study based on the guidelines of the ethics committee of our hospital having been obtained from the patient. The patients included 110 males and 48 females with a mean age of 64 ± 13 y. Nineteen (12%) of the 158 patients were at NYHA class I without any effort-induced symptom in response to medical therapy after admission. In the remaining 139 patients, symptomatic heart failure was stabilized but persisted (Table 1). The mean left ventricular ejection fraction (LVEF) was 41% ± 17%, and 54 (34%) of the patients had LVEF of <30% (Table 1). The etiology of left heart failure was identified as ischemic heart disease in 45 (28%) of the patients and as nonischemic cardiomyopathy in the remaining 113 (72%) patients. Atrial fibrillation and ventricular tachycardia were documented in 63 (40%) and 46 (29%) of the patients, respectively. Chronic renal dysfunction, hypertension, and diabetes mellitus were identified in 27 (17%), 14 (9%), and 45 (28%) of the patients, respectively. Chronic renal dysfunction was defined as a persistent elevation in serum creatinine concentration of ≥1.5 mg/mL (133 μmol/L) or as a creatinine clearance of <50 mL/min. Diabetes mellitus was defined as an increased fasting plasma glucose concentration of ≥126 mg/dL (18.5 mmol/L), glycosylated hemoglobin (HbA1c) of ≥6.4%, or when patients undergo treatment with insulin or hypoglycemic agents. No patients had valvular heart disease or congenital heart disease that required surgical repair. Patients received standard drug therapy that had been conventionally used at the entry but no antidepressants were used. Use of diuretics or digitalis was continued preferentially in patients who had symptomatic heart failure or needed heart rate control; loop-diuretics were used for 106 (67%), spironolactone for 61 (39%), and digitalis for 45 (28%) of the patients. Nitrates and β-blockers were used preferentially for patients with coronary heart disease; nitrates were used for 39 (25%), and β-blockers for 87 (55%) of the patients. ACE inhibitors were used for 59 (37%) of the patients, ACE inhibitors or ARBs were used for 101 (64%) of the patients, and ACE inhibitors, ARBs, or β-blockers were used for 133 (84%) of the patients. Amiodarone was used for 17 (11%) of the patients. ICDs had been used in 12 (7.6%) of the patients before this study started (Table 1).
Clinical Backgrounds of 158 Patients and Comparison Between Survivors and Nonsurvivors
Patient follow-up was started after completion of assessments of BNP level, cardiac function, and cardiac 123I-MIBG activity with a primary endpoint of definitive cardiac death due to pump failure, with a second endpoint of sudden death or ICD discharge due to sustained ventricular tachycardia or fibrillation as near-cardiac death, and with a third endpoint of noncardiac death. Patients were regularly monitored for at least 6 mo. Sudden cardiac death was defined as witnessed cardiac arrest or death within 1 h after the onset of acute symptoms or unexpected, unwitnessed death (i.e., during sleep) in a patient known to have been well within the previous 24 h. Deaths due to deterioration of congestive heart failure were classified as pump failure death.
Measurements of Blood Levels of Natriuretic Peptides
Samples for the assay of plasma BNP concentration were transferred to chilled disposable tubes containing aprotinin (500 kallikrein inactivator units/mL) and immediately placed on ice and centrifuged at 4°C. The plasma BNP concentration was measured by a specific immunoradiometric assay using a commercial kit (Shionogi) as reported previously (1). Briefly, this assay uses 2 monoclonal antibodies against human BNP by sandwiching it between the 2 antibodies without the need for plasma extraction.
Quantification of Cardiac 123I-MIBG Activity
Under resting and fasting conditions, planar images from an anterior view were obtained 30 min and 4 h after an intravenous injection of 123I-MIBG (111 MBq) (Daiichi Radioisotope Labs, Ltd.) using a γ-camera equipped with a low-energy, general-purpose collimator as reported previously (12,13). Cardiac 123I-MIBG activity was quantified as the heart-to-mediastinum ratio (HMR) using planar 30-min postinjection and 4-h delayed images by manual setting of the region of interest with an 11 × 11 pixel on cardiac and upper mediastinal areas by nuclear medicine technicians without knowledge of each patient’s data (Fig. 1). This method has been reported to be highly reproducible (r = 0.996, P < 0.0001) in our laboratory (12). Subsequently, tomographic data were acquired over a 180° arc to calculate the washout rate of cardiac 123I-MIBG activity (12,13). Administration of oral drugs that could affect 123I-MIBG data was withdrawn transiently or permanently if possible.
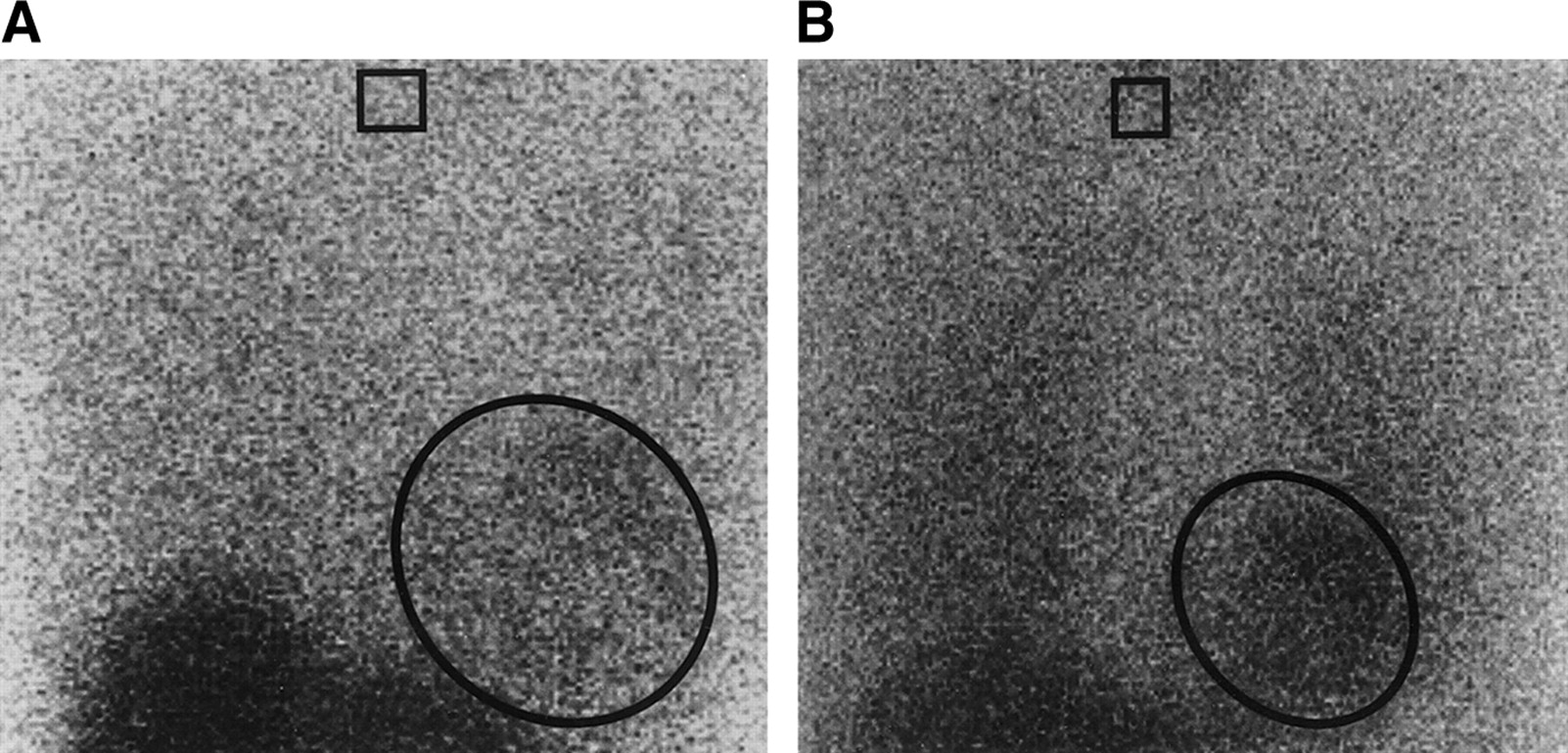
(A) A late cardiac planar 123I-MIBG image obtained from a 60-y-old female with congestive heart failure who had fatal pump failure. She had a persistently depressed LVEF (16%) and a highly increased plasma BNP level (1,070 pg/mL). Her late HMR (1.49) was markedly reduced. (B) A late cardiac planar 123I-MIBG image obtained from a 66-y-old male with congestive heart failure who survived. In response to drug therapy, he has an LVEF of 62%, a plasma BNP level of 76 pg/mL, and a normally preserved late HMR (2.14) at discharge. The box and oval indicate regions of interest on the upper mediastinal and cardiac areas, respectively, for calculation of the HMR of 123I-MIBG activity.
Statistical Analysis
Statistical values are shown as mean ± SD. The following variables were used for statistical analysis: age, sex, NYHA class, underlying disease responsible for heart failure (ischemic or nonischemic heart disease), complicating diseases (hypertension, diabetes mellitus, chronic renal dysfunction, tachyarrhythmias), LVEF, percentage of fractional shortening, left ventricular end-diastolic and end-systolic dimensions, plasma BNP level, medications used, early and late HMR, and its washout rate. Correlations between 2 continuous variables were analyzed by using linear regression analysis. Univariate and multivariate analyses with the Cox proportional hazards model were used to identify significant predictors of death. The Kaplan–Meier method was used to determine the time-dependent cumulative survival rate. Comparison of mean values between 2 groups was made using the unpaired Student t test, and prevalence was compared using the χ2 test. Survival curves were compared using the log rank test. Statistical potentials of selected independent predictors in univariate analysis were followed by multivariate analysis using the Wald χ2 and the Cox proportional hazards model. P < 0.05 was considered to be statistically significant. These analyses were performed using a computer software program, the SPSS statistical program package (SPSS version 11.0; SPSS Inc.).
RESULTS
Patient Characteristics and Outcomes
During 16 mo, 17 cardiac deaths and 3 noncardiac deaths were documented: 15 patients died from pump failure, 2 patients had sudden cardiac death, 1 patient died perioperatively when noncardiac surgery was performed, 1 died from acute pneumonia, and 1 died from a malignant tumor. Table 1 shows the clinical backgrounds of the patients who survived and those who died. The nonsurvivors had a significantly advanced age, greater NYHA functional class, greater plasma BNP concentration, and greater prevalence of chronic renal dysfunction and nitrate use compared with the survivors. There were, however, no significant differences in other variables, including cardiac function, scintigraphic data, underlying cardiac and noncardiac diseases, and other medications. ICD discharge was documented in 3 of the 12 patients in whom an ICD had been used.
Figure 1 shows typical late 123I-MIBG images. Despite aggressive medical treatment, a 60-y-old female with a persistently depressed LVEF (16%), a greatly increased plasma BNP level (1,070 pg/mL), and a markedly reduced 123I-MIBG HMR (1.49) at discharge had fatal pump failure. A 66-y-old male who had an LVEF of 62%, a plasma BNP level of 76 pg/mL, and a well-preserved 123I-MIBG ratio (2.14) showed a good response to drug treatment, resulting in good prognosis.
Correlations of Plasma BNP Level with Cardiac Sympathetic Innervation and LVEF
The plasma BNP level showed significant inverse correlations with the cardiac 123I-MIBG activity (late HMR) (r = 0.330, P < 0.0001) and with the LVEF (r = 0.192, P = 0.0150) (Fig. 2). Although the correlations were still statistically significant without use of a logarithm, the data were widely distributed and the inverse correlations are rough (r = 0.288, P = 0.0002 for late HMR and r = 0.190, P = 0.0168 for LVEF).
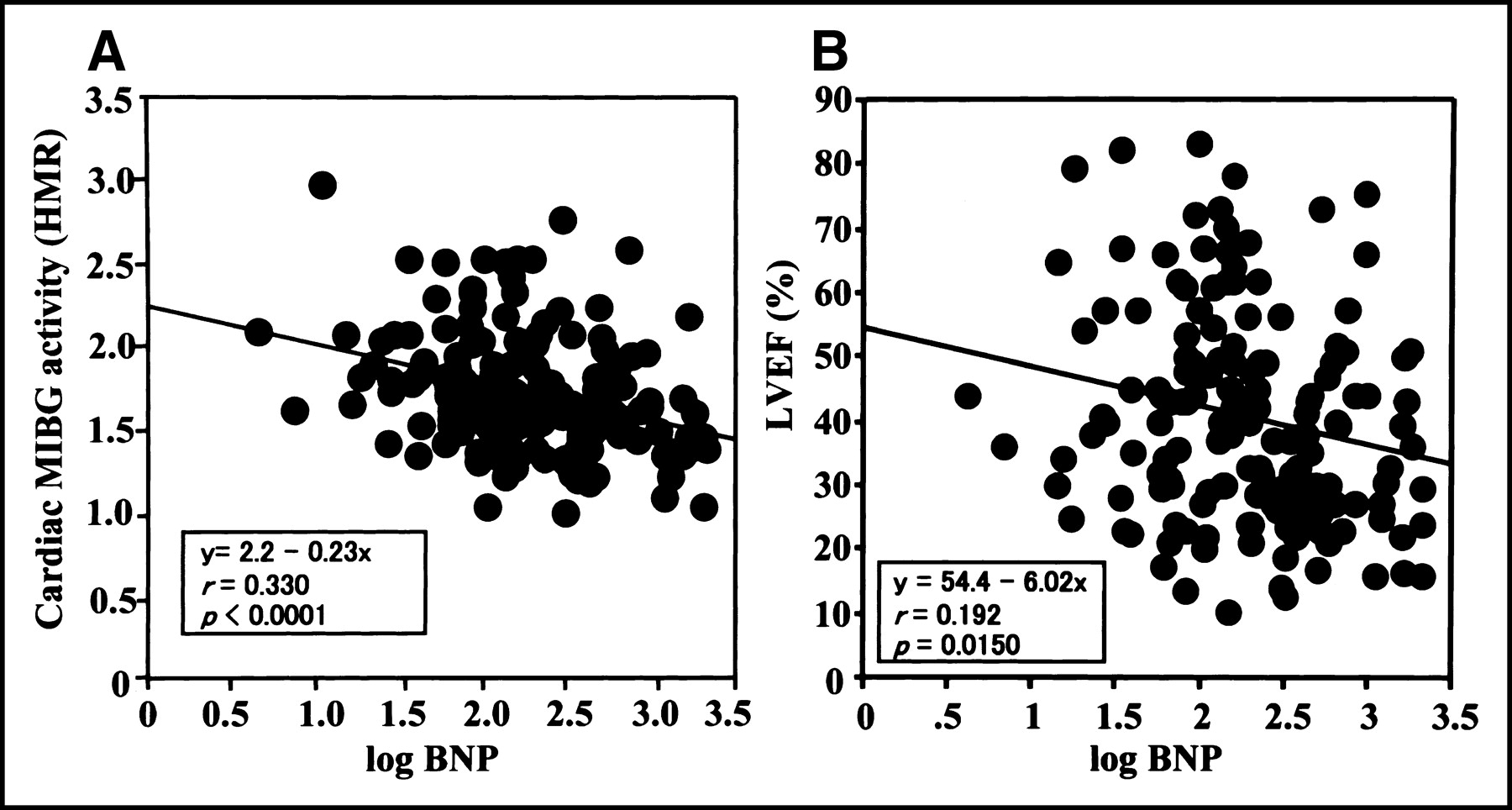
Correlations of the plasma BNP level with the cardiac 123I-MIBG activity quantified as late HMR (A) and LVEF (B). The inverse correlations between them are statistically significant but weak.
Determinants of Fatal Cardiac Events in Univariate and Multivariate Analyses
Univariate analysis identified the plasma BNP level, chronic renal dysfunction, age, cardiac 123I-MIBG activity (late HMR), use of nitrates, and diabetes mellitus as significant predictors of death due to pump failure (Table 2). Multivariate Cox proportional hazards regression analysis using these significant predictors showed that the plasma BNP level was an independent powerful determinant of fatal pump failure: Wald χ2 values and hazard ratios were 5.0916 and 1.0010, respectively (P = 0.02404) (Table 2).
Univariate and Multivariate Analyses for Predicting Cardiac Death Due to Pump Failure
Event Curve Analysis and Event Rates
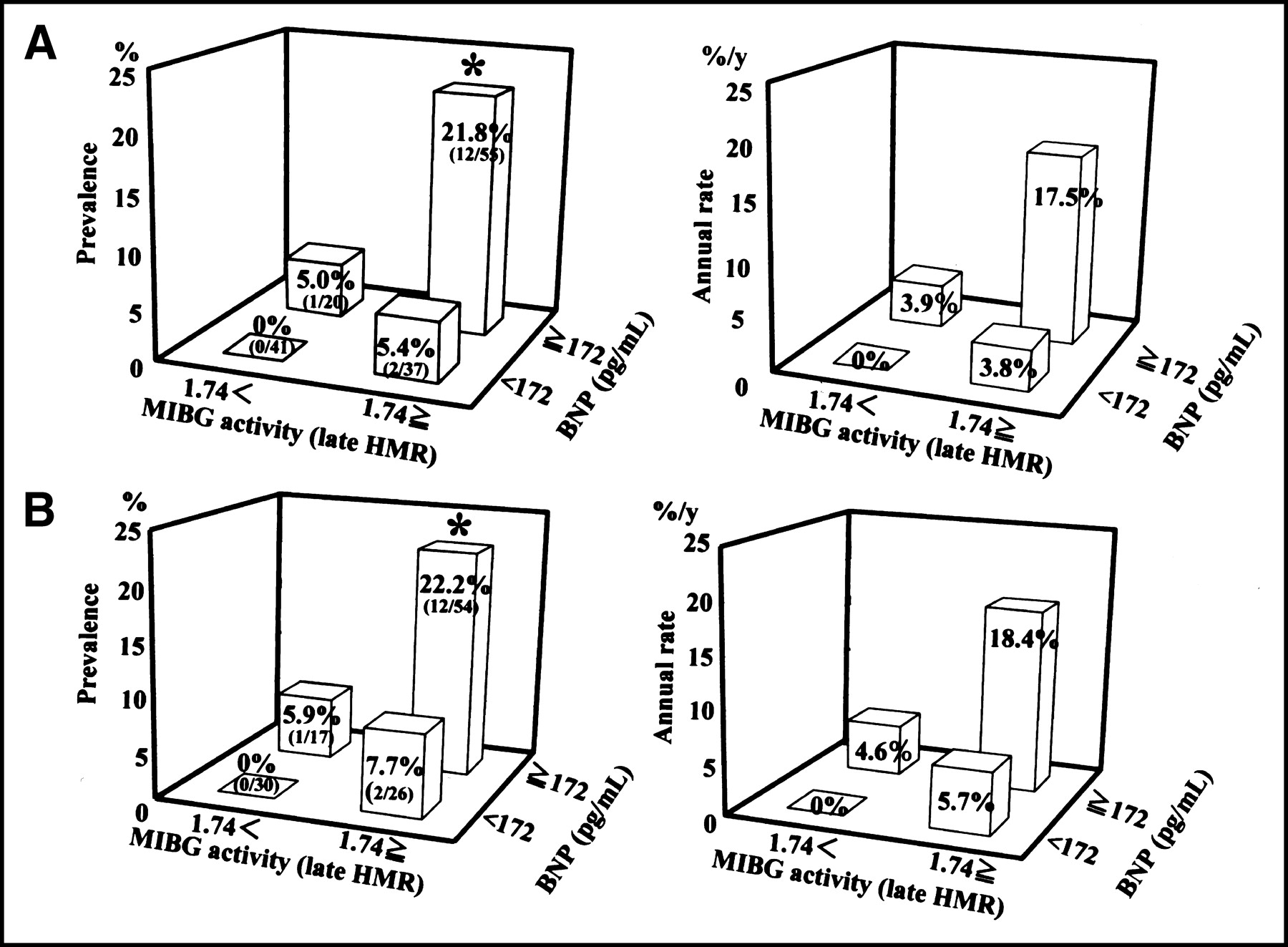
Patients were classified into 2 groups using 2 thresholds: a plasma BNP level of 172 pg/mL, which was the median value of plasma BNP levels in this study, and a cardiac 123I-MIBG activity (late HMR) of 1.74, which was the threshold identified in our previous study (12). The mortality rate due to pump failure was significantly higher in patients with a higher plasma BNP level (log rank = 9.50, P = 0.002, hazard ratio = 7.2, and 95% confidence interval = 1.6–32.1) or a lower cardiac 123I-MIBG activity (log rank = 7.70, P = 0.006, hazard ratio = 10.1, and 95% confidence interval = 1.3–77.0) than those of other patients (Fig. 3A). Likewise, when 127 patients with an LVEF of <50% were considered, patients with a higher plasma BNP level or a lower cardiac 123I-MIBG activity showed significantly greater survival rates than each counterpart (Fig. 3B). When patients were divided into 4 groups using both thresholds of the plasma BNP level and the cardiac 123I-MIBG activity, the group of patients with a plasma BNP level of ≥172 pg/mL and a late HMR of ≤1.74 had a significantly higher prevalence of fatal pump failure (21.8%; χ2 = 11.975, P < 0.001) than did the other groups (0%–5.4%) and an apparently greater annual rate of fatal pump failure (17.5%/y) than did the other groups (0%–3.9%/y) (Fig. 4A). When 127 patients with an LVEF of <50% were considered, the patient group with a higher plasma BNP level or a lower cardiac 123I-MIBG activity showed a significantly (P < 0.05) greater prevalence (22.2%) and an annual rate of fatal pump failure (18.4%/y) than did the other groups (Fig. 4B).
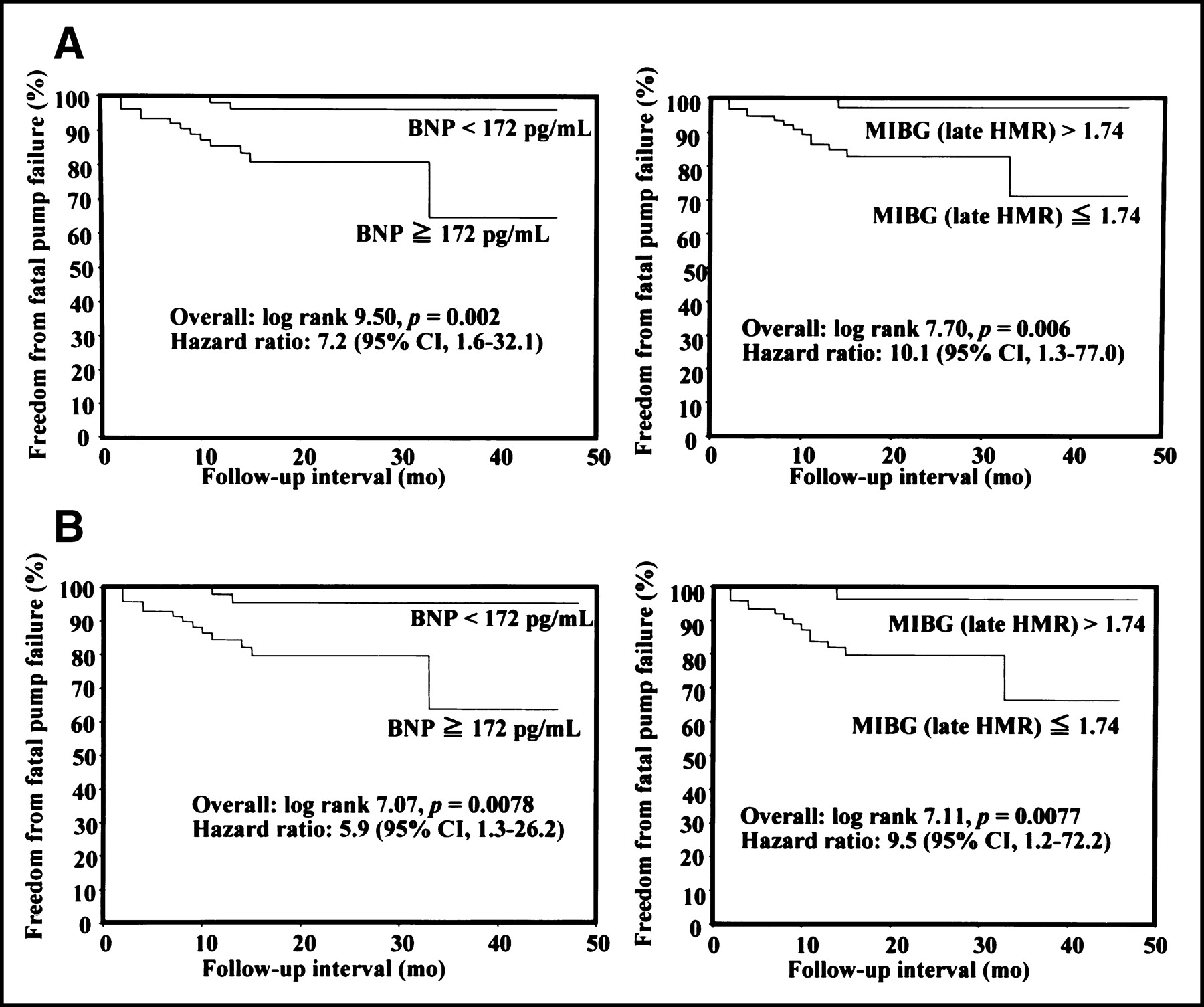
Kaplan–Meier event (fatal pump failure)-free curves when patients were stratified into 2 groups using the thresholds of a plasma BNP level of 172 pg/mL and an 123I-MIBG HMR of 1.74. The group of patients with plasma BNP levels of <172 pg/mL (left) or HMRs of >1.74 (right) had a significantly lower event rate than did each counterpart not only when all 158 patients were considered (A) but also when 127 patients who had an LVEF of <50% were considered for this analysis (B).

Comparison of prevalence (left) and annual rate of fatal pump failure (right) when patients were classified into 4 groups using the thresholds of a plasma BNP level of 172 pg/mL and an HMR of 1.74. The group of patients who had both a plasma BNP level of ≥172 pg/mL and an HMR of ≤1.74 had significantly greater event rates than those of the other 3 groups not only when all 158 patients were considered (A) but also when 127 patients who had an LVEF of <50% were considered for this analysis (B). *P < 0.05 vs. the other 3 groups.
Incremental Prognostic Values in Combination of BNP Level and Other Variables
Figure 5 shows incremental prognostic values of combined assessment of the plasma BNP level, cardiac 123I-MIBG activity, diabetes mellitus, or chronic renal dysfunction, all of which were identified as significant predictors of fatal pump failure in univariate analysis (Table 2). The hazard ratio of the plasma BNP level (7.2) or the cardiac 123I-MIBG activity (10.1) increased to 34.4 when both variables were used, but no further improvement was observed in other combinations. The rate of fatal pump failure increased significantly from 22% to 62.5% when high plasma BNP and low cardiac 123I-MIBG activity levels accompanied both diabetes mellitus and chronic renal dysfunction.
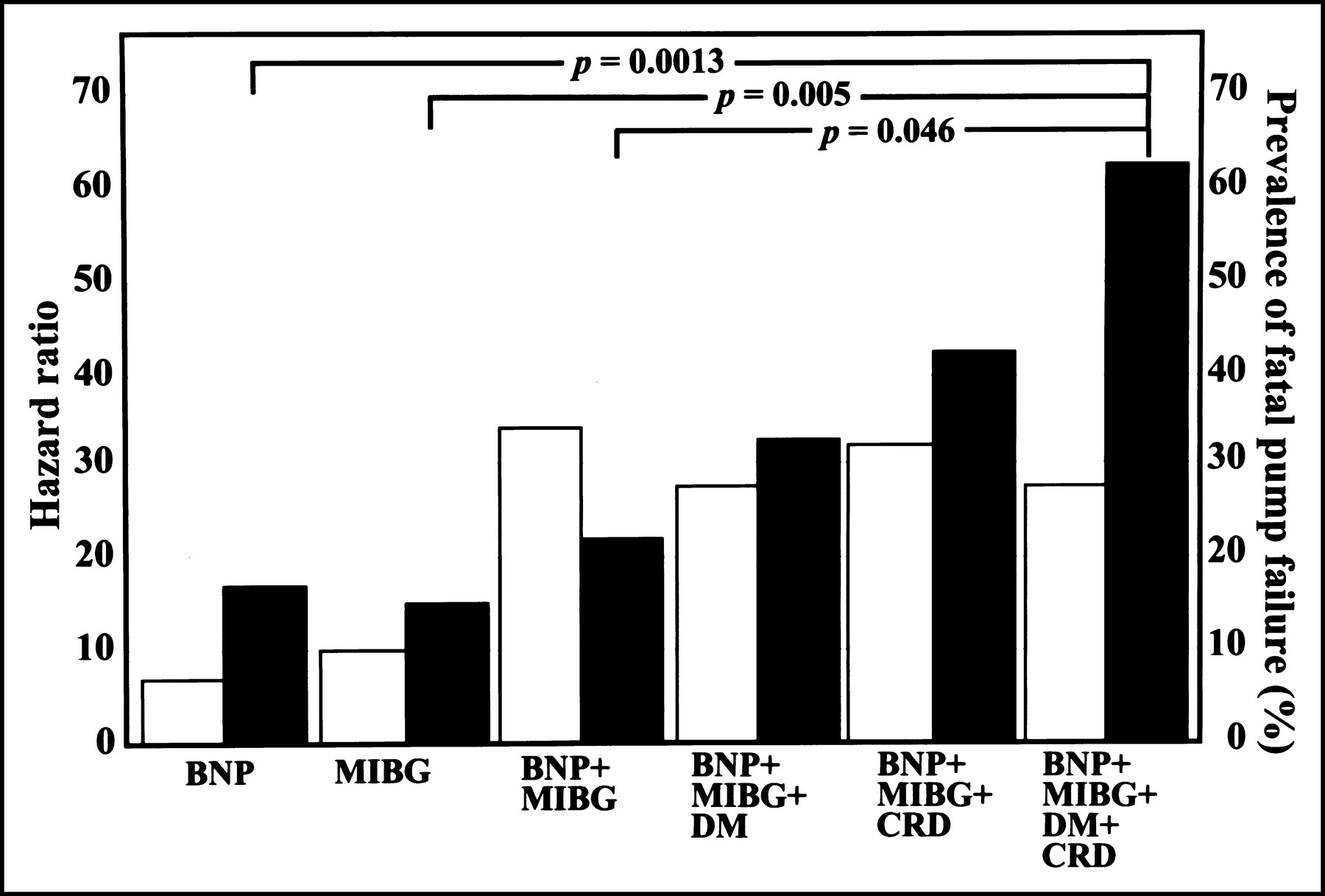
Incremental prognostic values of combined assessment of the plasma BNP level, the cardiac 123I-MIBG activity, diabetes mellitus (DM), or chronic renal dysfunction (CRD), all of which are significant predictors of fatal pump failure in univariate analysis (Table 2). Hazard ratios (□) for fatal pump failure increased to 34.413 when both the plasma BNP level and the cardiac 123I-MIBG activity were used, but no further improvement was achieved in any other combination. On the other hand, the greatest prevalence (62.5%) of fatal pump failure (▪) was observed when all of these variables were used.
DISCUSSION
The present results show that survival of patients with heart failure is related to depressed cardiac sympathetic activity and elevated BNP level and that combined assessment of these indices can improve risk stratification of patients at greater risk for pump failure death. Plasma BNP level increases in relation to interplay between hemodynamic alterations and cardiac function but is affected by age or right ventricular conditions. Augmented activities of central and peripheral sympathetic nervous systems (15) have potential deleterious effects on the cardiovascular system, whereas the myocardial content of norepinephrine is reduced in failing hearts (8). This finding is consistent with the observation of markedly depressed cardiac 123I-MIBG activity in failing hearts because the level of cardiac 123I-MIBG activity is related to the myocardial epinephrine content (16). The inverse correlation between the plasma BNP level and the cardiac sympathetic activity found in this study can be explained by their roles in heart failure. BNP is a slowly responding but powerful hormone in relation to the need for overload reduction in heart failure. Augmentation of central and peripheral functions of autonomic nervous systems, as an initial compensatory mechanism, makes sympathetic innervation in the myocardium exhausted and impaired during a long-term process, eventually leading to lethal outcome. This is probably because increases in circulating catecholamine levels and sympathetic outflow have deteriorating effects on the myocardium (17), because production of neurotransmitters at nerve terminals is reduced (18) and because depletion of high-energy phosphate at nerve endings impairs ion balance and autonomic functions (19). Recent investigations have shown that natriuretic peptides modulate systemic and cardiac autonomic nervous systems through a central neural action, by stimulating arterial and cardiac baroreceptor afferent nerve terminals or by inhibiting sympathetic ganglionic neurotransmission (20–22) even in a physiologic range (22). The correlation between the plasma BNP level and the cardiac sympathetic activity was statistically significant but not so strong in this study, suggesting differences in their roles in the heart failure process and the existence of confounding factors that modify hemodynamic conditions, stimulation of BNP synthesis, and cardiac sympathetic nerve functions. A significant but not strong correlation between the plasma BNP level and the LVEF is probably because LVEF is affected by hemodynamic conditions and sympathetic activity and because the natriuretic peptide level is related not only to systolic dysfunction but also to diastolic dysfunction (23). These findings support the rationale of combined use of these neuronal and humoral factors for risk stratification of patients with heart failure at high risk for lethal outcomes.
There are several known clinical backgrounds or noncardiac diseased states that affect long-term prognosis of patients with heart failure (5–7,24). The plasma BNP level was the most powerful prognostic marker among the variables examined in multivariate Cox analysis. It should, however, be noted that risk for fatal pump failure increases significantly when both diabetes mellitus and chronic renal dysfunction are present in patients with heart failure in whom the plasma BNP level is elevated and the cardiac 123I-MIBG activity is impaired, suggesting incremental prognostic implications of the diabetic state and chronically impaired kidney function in patients with heart failure. Earlier studies (5,6,25–29) also showed that diabetic mellitus and renal dysfunction are likely to be risk factors for mortality in patients with left ventricular dysfunction. Although the precise mechanisms of adverse effects of these conditions were not determined in this study, there are some possible explanations. Both diabetic mellitus and renal dysfunction at an advanced stage impair the function of the autonomic nervous system in the myocardium independent of complicated structural heart disease (30,31), resulting in impairment of cardiac functional reserve, regulation of vascular tone, and electrophysiological stability. In addition, a diabetic state impairs endothelial function in the coronary artery and augments epicardial coronary sclerosis, interstitial fibrosis, and intracellular metabolic alterations in failing hearts, all of which possibly lead to further impairment of cardiac diastolic and systolic performances and to lethal arrhythmias (25–27). Although reduced kidney function is a powerful independent predictor of mortality in patients with advanced heart failure, it remains controversial whether impaired renal function is associated with low cardiac output or with cardiac risk factors for mortality, such as low LVEF and high NYHA functional class (5,28,29). Renal dysfunction may be related to systemic risk factors for mortality, such as electrolyte (sodium and potassium) imbalance, hyperfibrinogenemia, increased C-reactive protein levels, overloaded conditions, and anemia (5,24).
In this study, patients underwent standard drug treatment for heart failure (14), including treatment with ACE inhibitors, ARBs, and β-blockers; 133 (84%) of the patients were treated with at least one of these drugs, but these drugs were not used for treatment of the remaining 25 (16%) patients because of adverse effects, depressed heart rate, or low systolic blood pressure. BNP and cardiac 123I-MIBG values were measured under conditions stabilized by the drug treatment because both of these values can alter during an early stage of heart failure and pharmacologic introduction and because this study aimed to evaluate long-term prognosis using data obtained at discharge. It is notable that combined assessment of the plasma BNP level and the cardiac sympathetic innervation enabled more accurate identification of patients at greater risk who were undergoing the standard drug treatment for heart failure. Because both BNP and 123I-MIBG data may have altered during a long-term period or due to progression of heart failure (32–36), it is necessary to determine the appropriate timing and appropriate interval for measurements of the plasma BNP level and the cardiac 123I-MIBG activity during the clinical course of heart failure for more accurate prediction of the long-term prognosis.
Another important clinical issue is whether the markers used here are reliable predictors of sudden death in patients with heart failure. There is no established method for predicting sudden lethal events, probably because of the many triggers involved (37). Berger et al. (33) recently showed the possibility of the plasma BNP level predicting sudden death in patients with an LVEF of ≤35%. Although the statistical powers of the plasma BNP level and the cardiac 123I-MIBG activity were maintained when 2 sudden cardiac deaths and 3 ICD discharges observed in this study were included in the analysis, the small number of episodes made it difficult to draw a definitive conclusion. Our recent study has demonstrated that combined data on cardiac 123I-MIBG activity and heart rate variability improves prediction of ICD shock due to lethal arrhythmias (38). This preliminary result suggests that depressed functions of central and cardiac autonomic nervous systems are responsible for sudden lethal events and that combined assessment of these indices is useful for the prediction of and management of heart failure patients at high risk for sudden cardiac death.
Cardiac 123I-MIBG imaging enables assessment of the presynaptic function of the cardiac sympathetic nervous system but not the postsynaptic function. In failing hearts, β-adrenoceptor function is downregulated, whereas supersensitivity of adrenoceptor function is observed when cardiac sympathetic presynaptic innervation is impaired (39). The interaction between pre- and postsynaptic functions in failing human hearts must be determined. The patients enrolled in this study had congestive heart failure, but 31 (20%) of the patients had an LVEF of ≥50% at convalescence. In particular, 16 (10%) patients with an LVEF of ≥65% had left ventricular hypertrophy and diastolic dysfunction on 2-dimensional echocardiography. Heart failure with preserved systolic function is observed in roughly one third of patients with heart failure, probably due to diastolic dysfunction (40). These findings suggest that assessment of the cardiac sympathetic innervation and the BNP level is useful for identifying heart failure patients who have preserved systolic function but impaired diastolic function and are at high risk for cardiac death. A recently reported rapid assay of the BNP level is a promising method for screening, early diagnosis, and monitoring of patients with suspected or known heart failure. Despite the limited availability of cardiac 123I-MIBG imaging, the noninvasive and quantitative features can contribute to further risk assessment of heart failure patients who are identified to be at high risk for cardiac death by the plasma BNP level and other variables. Finally, the present findings indicate the need for planning a larger prospective multicenter study to establish a new diagnostic strategy using the plasma BNP level, cardiac sympathetic nerve activity, and other clinical markers.
CONCLUSION
The plasma BNP level is inversely related to cardiac sympathetic nerve innervation and is a more powerful prognostic marker than other factors for mortality in patients with congestive heart failure who have undergone contemporary drug therapy. Impaired cardiac sympathetic nerve innervation and the presence of diabetes mellitus and chronic renal dysfunction, however, increase the risk for lethal cardiac events in patients with heart failure and increased plasma BNP concentration. Thus, combined assessment of the plasma BNP level, cardiac sympathetic innervation, and noncardiac diseases such as diabetic state and impaired kidney function enables better identification of patients at greater risk for cardiac death.
Acknowledgments
The authors thank the staffs of the Cardiology Department and Division of Nuclear Medicine, Sapporo Medical University School of Medicine, Sapporo; the Cardiovascular Clinic, Sapporo; and the Division of Cardiovascular Medicine, Hakodate Goryokaku Hospital, Hakodate, for their cooperation in clinical services.
Footnotes
Received Jun. 23, 2003; revision accepted Oct. 9, 2003.
For correspondence or reprints contact: Tomoaki Nakata, MD, PhD, Second Department of Internal Medicine (Cardiology), Sapporo Medical University School of Medicine, S-1, W-16, Chuo-ku, Sapporo 060-8543, Japan.
E-mail: tnakata{at}sapmed.ac.jp
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Cardiac 123I-MIBG Imaging for Clinical Decision Making: 22-Year Experience in Japan
- A Pooled Analysis of Multicenter Cohort Studies of 123I-mIBG Imaging of Sympathetic Innervation for Assessment of Long-Term Prognosis in Heart Failure
- Synergistic prognostic values of cardiac sympathetic innervation with left ventricular hypertrophy and left atrial size in heart failure patients without reduced left ventricular ejection fraction: a cohort study
- Influence of Ejection Fraction on the Prognostic Value of Sympathetic Innervation Imaging With Iodine-123 MIBG in Heart Failure
- Cardiac Mortality Assessment Improved by Evaluation of Cardiac Sympathetic Nerve Activity in Combination with Hemoglobin and Kidney Function in Chronic Heart Failure Patients
- Advances in SPECT and PET for the management of heart failure
- Iodine-123 Metaiodobenzylguanidine Imaging and Carbon-11 Hydroxyephedrine Positron Emission Tomography Compared in Patients With Left Ventricular Dysfunction
- Impaired Cardiac Sympathetic Innervation and Myocardial Perfusion Are Related to Lethal Arrhythmia: Quantification of Cardiac Tracers in Patients with ICDs
- Cardiac Sympathetic Imaging With mIBG in Heart Failure
- The Significance of Cardiac Sympathetic Nervous System Abnormality in the Long-Term Prognosis of Patients with a History of Ventricular Tachyarrhythmia
- Predicting the Need for an Implantable Cardioverter Defibrillator Using Cardiac Metaiodobenzylguanidine Activity Together with Plasma Natriuretic Peptide Concentration or Left Ventricular Function