


Abstract
This study was designed to assess the prognostic value of stress myocardial perfusion SPECT with electrocardiographic (ECG) gating in patients undergoing noncardiac surgical treatment. Methods: The study included 481 consecutive patients who underwent noncardiac surgery and had been referred for preoperative myocardial perfusion scintigraphy. Myocardial scintigraphy used 99mTc-labeled perfusion agents and dipyridamole stress with ECG gating, permitting qualitative and quantitative analyses of both myocardial perfusion and cardiac function. Reconstructed perfusion images were analyzed qualitatively and semiquantitatively. The Quantitative Gated SPECT (QGS) program was used for gated SPECT analysis to calculate global left ventricular ejection fraction and estimate regional wall motion. We assessed the relationships between perioperative cardiac events and various predictors, including clinical risk factors, radionuclide perfusion, and functional variables. Results: Univariate analysis indicated that age (P < 0.001), diabetes mellitus (P < 0.01), history of heart failure (P < 0.05) or perfusion imaging (P < 0.0001), and QGS analysis (P < 0.0001) yielded significant risk stratification. According to multivariate analysis, age, diabetes mellitus, perfusion imaging, and QGS analysis were independent predictors of perioperative cardiac events. The event rate was correlated with quantitative scintigraphic indices of perfusion images (rest perfusion and ischemic scores) and QGS analysis (global ejection fraction and the number of hypokinetic segments). Although QGS functional data offered no significant incremental prognostic value in patients with abnormal perfusion, it classified patients with normal perfusion into 2 risk groups (P < 0.0001). A combination of clinical risk factors, scintigraphic perfusion results, and functional data allowed further detailed risk stratification. Conclusion: Stress myocardial perfusion SPECT with ECG gating has an incremental prognostic value over conventional nongated stress perfusion imaging in predicting perioperative cardiac events.
- stress myocardial perfusion SPECT
- quantitative gated SPECT
- preoperative risk stratification
- prognosis
- cardiac events
It is important to stratify cardiac risks in individual patients who plan to undergo surgical treatment. Radionuclide angiocardiography and stress myocardial perfusion scintigraphy have been used to evaluate perioperative or long-term morbidity and mortality in such patients (1–19). However, fewer reports have addressed a comparison of cardiac function and myocardial perfusion in assessing cardiac risks, mainly because of difficulty in performing 2 different examinations during the limited preoperative period (20–25). Moreover, only 1 article in our search elucidated the prognostic value of combined radionuclide angiography and myocardial perfusion imaging in predicting perioperative cardiac events (25). On the other hand, recent advances in computer technology and the development of algorithms for data analyses have permitted simultaneous assessment of myocardial perfusion and cardiac function in routine clinical examinations by using 99mTc-labeled myocardial perfusion agents and electrocardiographic (ECG)-gated SPECT (26). Some investigators used gated perfusion SPECT to estimate the prognoses of patients with known or suspected coronary artery disease (27–31). Nevertheless, no reports as yet have applied this technique to perioperative cardiac risk assessment.
The aim of this study was to evaluate the incremental prognostic value of ECG-gated myocardial perfusion SPECT for preoperative risk stratification. We performed dipyridamole stress perfusion SPECT with ECG gating on patients undergoing intermediate- or high-risk surgical procedures.
MATERIALS AND METHODS
Patients
This study included 550 consecutive patients who were scheduled to undergo noncardiac surgery and were referred for dipyridamole stress myocardial perfusion scintigraphy (September 1997–November 2000). Written, informed consent was obtained from all patients after they received a detailed explanation of the protocol. The form to obtain consent was approved by the institutional committee of Keio University Hospital (Tokyo, Japan). Surgery was canceled or deferred after the scintigraphic study in 69 patients, and 481 patients underwent surgical treatment. All of the surgical procedures were classified as high- or intermediate-risk procedures (high risk: 274 patients; intermediate risk: 207 patients) according to American College of Cardiology/American Heart Association guidelines (32). Among the high-risk surgeries, 234 were vascular procedures (aortic aneurysm: 184; peripheral vascular: 50); 38 were prolonged procedures with large fluid shift; and 2 were emergent major operations in the elderly. Intermediate-risk operations included 156 intraperitoneal and intrathoracic surgeries, 6 prostatectomies, 2 carotid endarterectomies, 12 head and neck operations, and 31 orthopedic surgeries. Clinical characteristics of the patients are indicated in Table 1.
Clinical Characteristics of 481 Patients
Protocol
99mTc-tetrofosmin or -sestamibi was used as the imaging agent in a 1-d rest/stress protocol. In the rest study, all patients were injected with 300 MBq of the tracer, and SPECT acquisition was performed 30 min after injection. In the stress study, patients were continuously injected with 0.56 mg/kg dipyridamole for 4 min. Three minutes after the completion of the dipyridamole infusion, 850 MBq of the perfusion tracer were administered. Stress SPECT images were obtained 30–60 min after administration.
Instrumentation
A 3-head rotating gamma camera (GCA-9300A/DI; Toshiba Corp., Tokyo, Japan) was used for data acquisition, and a medical image processor (GMS-5500U/DI; Toshiba Corp.) was used for image processing. The gamma camera rotated continuously for 15 min in each acquisition. SPECT images were reconstructed into a 64 × 64 matrix with a ramp filter after processing 90 projections over 360° using a Butterworth filter (order, 8; cutoff, 0.30 cycles per pixel). ECG gating was performed by dividing the cardiac cycle into 10 periods.
Image Analysis
After visual interpretation of the rest and stress SPECT images, perfusion images were also semiquantitatively assessed using 4-point scoring (0–3 for normal perfusion to defect) in the following 9 myocardial segments: 4 segments in a basal short-axis image, 4 segments in a mid short-axis image, and 1 apical segment in a long-axis image. Ischemic score was defined as stress total perfusion score − rest total perfusion score, which reflects the severity of myocardial ischemia.
The Quantitative Gated SPECT (QGS) program (Cedars-Sinai Medical Center, Los Angeles, CA) was used for gated SPECT analysis (26). Calculation of left ventricular ejection fraction (LVEF) values and wall motion analysis were performed by means of automatic determination of endocardial and epicardial surfaces for all gating intervals in the cardiac cycle. We used rest EF for data analysis. Regional wall motion was visually estimated using the cine-mode display of the data. In this estimation, we judged whether wall motion was or was not normal, with a normal finding defined as the absence of wall motion abnormality in any LV segments. In addition, we calculated the total number of hypokinetic segments in each patient by dividing the LV wall into 7 segments: anterobasal, anterior, apex, inferior, posterior, septum, and lateral.
Medical Record Review
We assessed clinical risk factors and the occurrence of cardiac events by reviewing the medical record. Clinical variables considered were age (≥75 y), hypertension, diabetes mellitus, hypercholesterolemia (serum cholesterol > 240 mg/dL), chest pain, preoperative arrhythmias, history of myocardial infarction, history of congestive heart failure, history of coronary revascularization, ECG analysis including necrotic Q waves, and ischemic ST change at rest.
Perioperative cardiac events were defined as those that occurred during operation and either before hospital discharge or up to 1 mo after surgery in patients with longer hospital stays. Cardiac events included cardiac death, nonfatal myocardial infarction, unstable angina, congestive heart failure, and performance of revascularization (15,17). Cardiac death was defined as death resulting from myocardial infarction, heart failure, or arrhythmias. The diagnostic criteria for myocardial infarction were based on ECG changes and serum creatine kinase (CK) value (new ECG Q wave ≥ 1 mm or CK-MB ≥ 5% or both). Unstable angina was defined by ECG ST changes (ST-segment depression or elevation ≥ 1 mm on the 12-lead ECG) with cardiac symptoms. Congestive heart failure was defined as radiographic evidence of pulmonary edema and cardiac enlargement requiring inotropic support. Nonfatal arrhythmias were excluded from cardiac events. Hard events included cardiac death and myocardial infarction.
Statistical Analysis
In univariate analysis, we used the Fisher exact test to compare frequency of cardiac events between patients with positive and negative test results. Stepwise logistic regression models were used to identify independent predictors of cardiac events (Stat View, version 4.5; Abacus Concepts, Inc., Berkeley, CA). P < 0.05 and an F value > 4.0 were considered statistically significant in univariate and multivariate analyses, respectively.
RESULTS
Of the total 481 patients, cardiac events were observed in 39 patients (8.1%). Hard events were documented in 8 of these 39 patients. Among the 69 patients who did not proceed to surgery, 33 (47.8%) manifested positive perfusion images; this proportion is significantly higher than the rate of positive perfusion images in patients who had surgery (47.8% vs. 25.8%; P = 0.0003).
Table 1 shows the results of univariate and multivariate analyses of the predictability of cardiac events with clinical and scintigraphic data. Univariate analysis indicates that age, diabetes mellitus, history of heart failure, perfusion imaging, and QGS analysis yielded significant risk stratification. Age (F = 23.3), diabetes mellitus (F = 5.9), perfusion imaging (F = 4.5), and QGS analysis (F = 45.2) are independent predictors according to the result of stepwise logistic regression analysis.
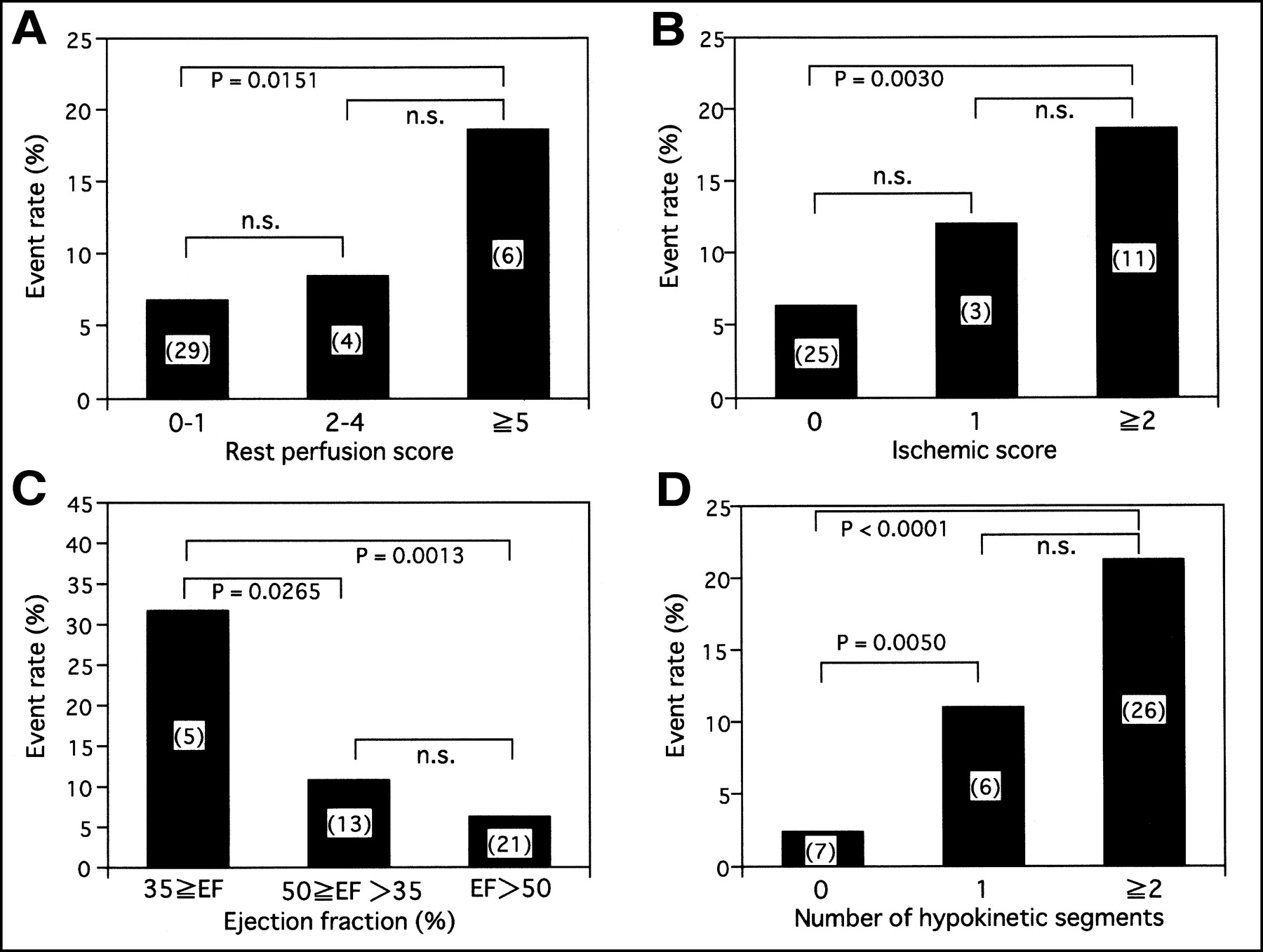
The relationships between scintigraphic quantitative variables and cardiac events are shown in Figure 1. The event rate increased with decreasing values of EF and with increasing values of rest perfusion and ischemic scores and numbers of hypokinetic segments.

Scintigraphic variables and event rates. (A) Rest perfusion score and event rate. (B) Ischemic score and event rate. (C) Ejection fraction and event rate. (D) Number of hypokinetic segments and event rate. Numbers of patients with cardiac events are indicated in parentheses. n.s. = not statistically significant.
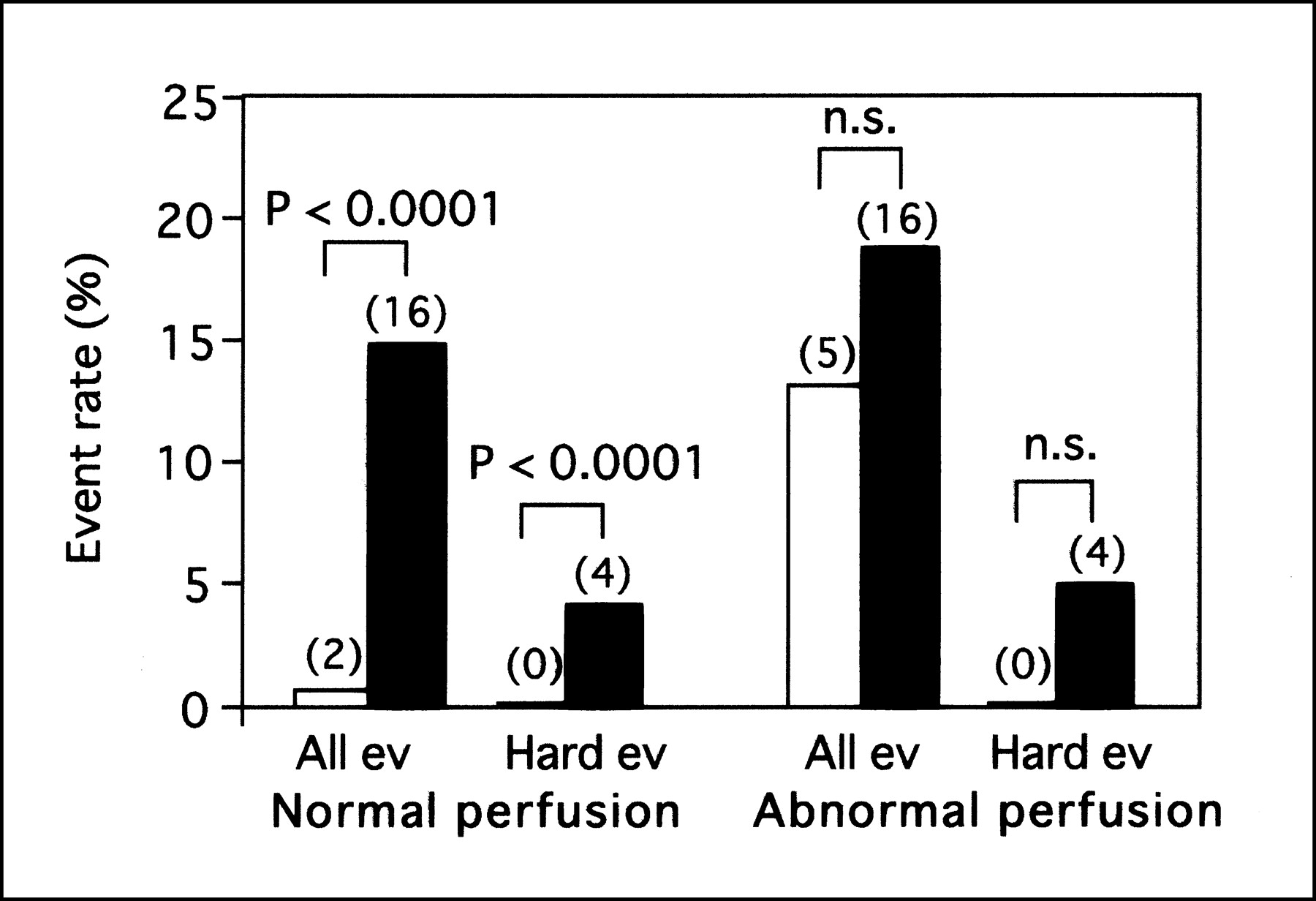
Figure 2 shows the incremental prognostic value of wall motion data obtained with QGS. Although the functional data offered no significant additive prognostic value in patients with abnormal perfusion images, it classified patients with normal perfusion into 2 risk groups.
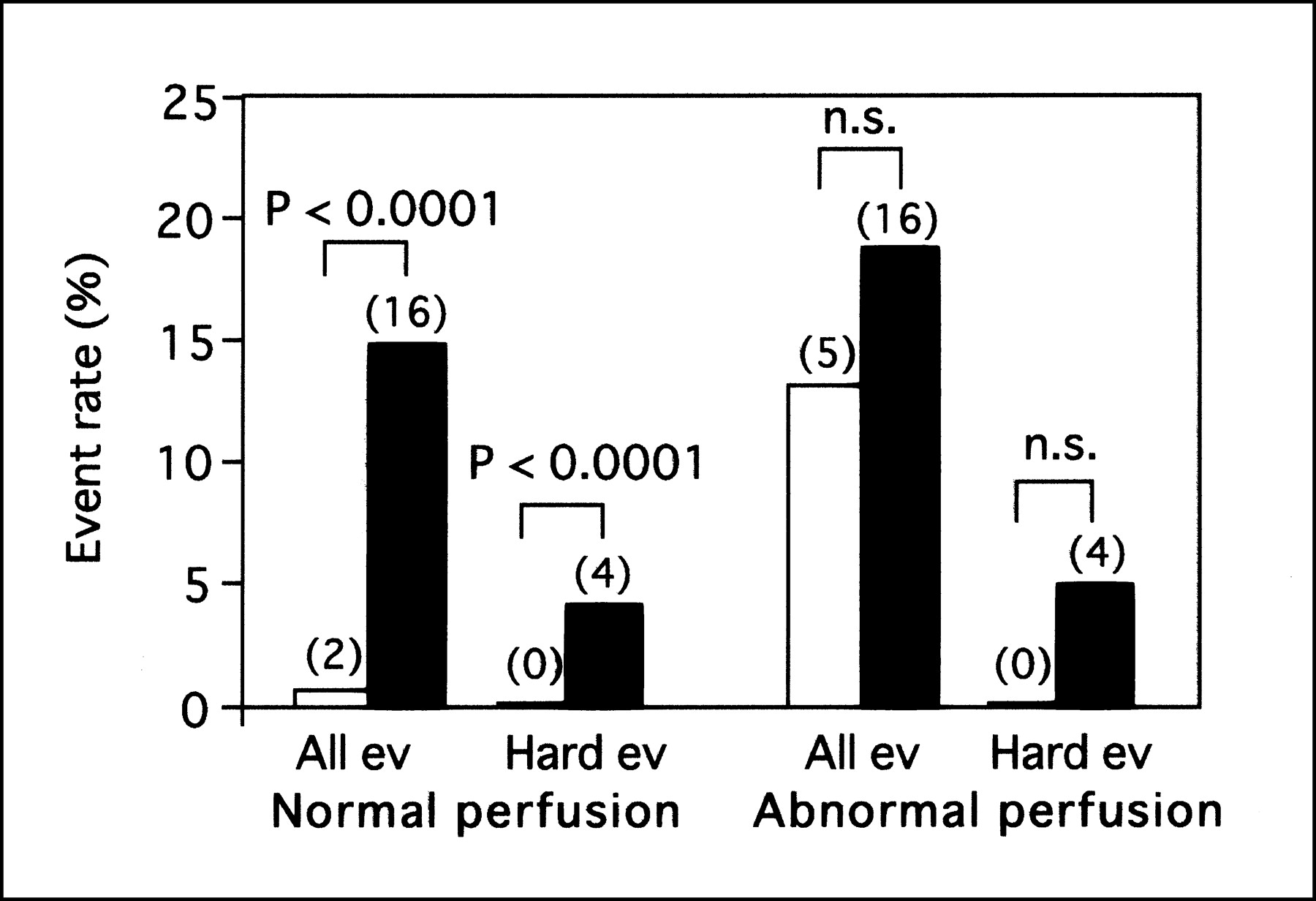
Incremental prognostic value of wall motion data. Numbers of patients with cardiac events are indicated in parentheses. Open bar = without wall motion abnormality; closed bar = with wall motion abnormality; All ev = all cardiac events; Hard ev = hard events only; n.s. = not statistically significant.
Risk assessment with combined clinical and scintigraphic data is illustrated in Figure 3. Patients were divided into 4 groups on the basis of the number of clinical risk factors (≤2 and >2) and findings of perfusion images (normal vs. abnormal). Each of these groups was divided into 2 subgroups on the basis of QGS analysis (normal and abnormal). The statistical analysis showed significant discrimination with QGS findings in 2 groups of patients with normal perfusion. Of the 8 patients with hard events, 4 manifested both perfusion and wall motion abnormality and the other 4 showed only wall motion abnormality.

Risk assessment with combined clinical and scintigraphic data. White column = normal wall motion; hatched column = abnormal wall motion. *Not statistically significant; **P = 0.0172; +P = 0.0005 (with vs. without wall motion abnormality).
DISCUSSION
Many investigators have identified preoperative clinical markers related to postoperative cardiac events; the most frequently reported markers are advanced age (1,10,22, 33), hypertension (22,33), diabetes (6,9, 12,14,17, 29,33), angina pectoris (17), cardiac arrhythmias (10,22), history of myocardial infarction (10,15, 25,29), congestive heart failure (14,17, 25,33), prior coronary artery bypass graft surgery (17), and abnormal baseline ECG (10,33). Our study indicated that advanced age, diabetes, and heart failure are significant predictors of perioperative cardiac events (Table 1). However, some reports suggested the limited value of clinical markers compared with scintigraphic and echocardiographic variables (20, 22). These differences are probably caused by report-dependent variability in the number of patients studied, prevalence of risk factors, and types of operations performed.
In addition to clinical markers, preoperative cardiac risk stratification is often performed using radionuclide techniques, especially in patients undergoing vascular surgery. Until the early 1990s, radionuclide angiocardiography was performed mainly for risk assessment (1–9). This procedure was superseded by stress myocardial perfusion scintigraphy (10–19). Although combined myocardial perfusion imaging and radionuclide angiography offers an incremental prognostic value in predicting surgery-related cardiac events (25), its use is limited because of additional cost and time before surgical procedures. Although the combination of perfusion imaging and echocardiography, which is easier to perform, has also been reported to be useful in preoperative risk assessment (20), an accurate EF value is not easy to obtain in routine clinical examination. To overcome this problem, we have used ECG-gated myocardial perfusion SPECT, permitting simultaneous evaluation of myocardial perfusion and cardiac function without additional cost and time. Some authors have applied this technique to risk stratification in patients with various conditions (27–31). According to these reports, gated SPECT parameters, including rest EF (27,30) and poststress EF (28,29,31), have incremental prognostic value in patients with acute myocardial infarction (29, 30) and with known or suspected coronary artery disease (27, 28,31). The EF value was proved to be a significant predictor of cardiac death (31), heart failure (22,30), and hard events (29). However, to our knowledge, no articles have elucidated the significance of gated SPECT in predicting perioperative cardiac events. To assess its prognostic value, we performed univariate and multivariate analyses (Table 1) and illustrated risk stratification using QGS data after sorting patients with prescan and perfusion information (Figs. 2 and 3).
It has been reported that preoperative stress myocardial perfusion imaging provides excellent negative predictive values in forecasting perioperative and late cardiac events, which implies that a normal stress perfusion study has powerful prognostic utility (34). The results of the present study suggest that the addition of functional variables to perfusion data allows further refined selection of low-risk patients (Figs. 2 and 3). In other words, normal perfusion and wall motion ensure a very low likelihood of perioperative cardiac events. This refinement was achieved by excluding patients with normal perfusion and abnormal wall motion. These patients included mainly those with cardiac dysfunction resulting from cardiomyopathy, valvular diseases, and other noncoronary causes. The above excluded patients offered a relatively high event rate (14.5%), and all events were cardiac death or heart failure with no ischemic episodes. This means that the addition of ECG gating is useful not only in stratifying risks but also in obtaining event-specific information. The result is compatible with reports showing that perioperative heart failure is predicted by preoperative cardiac dysfunction measured with echocardiography or radionuclide angiography (20,22). It is also reported that exercise echocardiography and gated SPECT were predictive for heart failure or cardiac death and that exercise SPECT has predictive power with ischemic complication, although these events are not perioperative (30,31). In addition, accurate identification of low-risk patients facilitates reduction of cost and preoperative waiting time, because these low-risk individuals can be exempted from further cardiac testing, including catheterization, and proceed directly to surgical treatment (18). The ECG-gated perfusion study is thought to be clinically feasible in assessing perioperative cardiac risks because it provides incremental functional variables reflecting prognosis over conventional perfusion imaging without requiring additional time, cost, or radiation exposure.
SPECT images are susceptible to artifact as a result of photon attenuation or patient movement during data acquisition. This artifact often results in abnormal perfusion images with normal wall motion (35). Therefore, addition of QGS functional data is useful to separate such cases from patients with true-positive perfusion images (35,36), which may lead to improved accuracy in predicting perioperative cardiac events. Further studies are required to elucidate the effect of QGS on this aspect.
One of the most important characteristics of scintigraphic imaging is that it provides not only qualitative but also quantitative information about the activity of organs in vivo. In prognosis assessment, quantitative variables permit stratification into 3 or more different risk groups; in contrast, qualitative data provide only a dichotomy. Therefore, we evaluated the usefulness of quantitative parameters in assessing perioperative cardiac events, as indicated in Figure 1. Most reports using radionuclide angiocardiography concluded that the rate of perioperative cardiac events increases with decreasing LVEF values (1–7,9, 21–23,25), and it was indicated that the event rate is very high, especially in patients with LVEF ≤ 35% (1–4,7,23). Although the majority of these reports focused on hard events, the same tendency was observed in both hard and soft events in our study. Studies using gated SPECT (not preoperative estimation) also yielded similar results in terms of prognostic utility (27–31).
We obtained quantitative data also from perfusion images, including rest perfusion and ischemic scores. The former reflect the severity of myocardial infarction, and the latter are related to the severity of ischemia. Several investigators have clarified the significance of quantitative parameters based on perfusion images in predicting perioperative and late cardiac events (11,12,16). According to these reports, the number of reversible defects is correlated with the perioperative event rate, whereas the rest perfusion defect is the predictor of late cardiac events rather than perioperative events. Baron et al. (22), however, indicated the limited ability of reversible perfusion defect as a predictor of perioperative cardiac events. Our results showed that not only the number of reversible defects but also the rest perfusion score were predictors of perioperative events. In the present study, reversible defects were observed in 25.6% of patients with a rest perfusion score ≥ 5, whereas the ratio was 12.8% in those with the score ranging from 2 to 4. This interdependence of the rest perfusion score and the presence of ischemia in our study can account for these results.
Some limitations are inherent in the present study. The first is that surgeons and anesthesiologists were aware of the results of scintigraphic testing. This availability of results had an influence on decisions regarding performance of surgery and perioperative management of patients, which may contribute to lowering the cardiac event rate and the positive predictive value (37).
The second limitation results from the use of dipyridamole stress instead of exercise. Some authors have indicated that exercise capacity and poststress functional variables are excellent predictors of cardiac events, by using exercise testing incorporating radionuclide imaging (9,28, 29,31). We used dipyridamole stress because a certain number of patients in the present study were undergoing vascular surgery or were elderly and were not suitable for exercise testing.
Finally, we analyzed the mixture of patients undergoing high- and intermediate-risk operations. Event rates in patients undergoing high- and intermediate-risk surgery were 8.8% and 7.5% (not statistically significant), respectively. No statistical difference was noted in the event rate, and an additional study enrolling an increased number of patients is required to conduct subgroup analyses. In addition, the dependence of the perioperative event rate on patient characteristics and surgical procedures in each hospital should be considered when these results are applied to procedures performed in other hospitals. Patients in the present study include a large number of individuals undergoing high-risk procedures (57% of the patient population), including vascular surgery. Procedures were performed at a large teaching hospital with the necessary level of surgical expertise.
CONCLUSION
Stress myocardial perfusion SPECT with ECG gating has an incremental prognostic value over conventional nongated stress imaging in predicting perioperative cardiac events, especially in patients with normal perfusion. This procedure is clinically feasible because it provides additional functional variables without requiring additional time, cost, or radiation exposure.
Footnotes
Received Apr. 4, 2002; revision accepted Sep. 25, 2002.
For correspondence or reprints contact: Jun Hashimoto, MD, Department of Radiology, School of Medicine, Keio University, 35 Shinanomachi, Shinjuku-ku, Tokyo, 160-8582, Japan.
E-mail: junhashi{at}rad.med.keio.ac.jp
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Prognostic capabilities of coronary computed tomographic angiography before non-cardiac surgery: prospective cohort study
- Coronary Computed Tomography Angiography After Stress Testing: Results From a Multicenter, Statewide Registry, ACIC (Advanced Cardiovascular Imaging Consortium)
- Myocardial Perfusion Imaging for Preoperative Risk Stratification
- Gated Myocardial Perfusion SPECT: Basic Principles, Technical Aspects, and Clinical Applications
- The Diagnostic and Prognostic Value of ECG-Gated SPECT Myocardial Perfusion Imaging