


Abstract
Since the development of gated SPECT imaging approximately 10 y ago, this technique is now almost universally used as an adjunct for radionuclide perfusion imaging, enabling the assessment of perfusion along with determination of regional and global left ventricular function in the same examination. The gated SPECT determination of the left ventricular ejection fraction and volumes has been extensively validated. Additionally, this method allows for the improved identification of soft-tissue artifacts and enhances the detection of multivessel coronary artery disease. Furthermore, gated SPECT provides powerful information for the risk assessment of patients with known or suspected coronary artery disease and aids in the assessment of myocardial viability. Gated SPECT imaging has clearly become an integral part of radionuclide myocardial perfusion imaging.
Electrocardiographically (ECG)-gated myocardial perfusion SPECT was developed in the late 1980s and has rapidly evolved into a standard for myocardial perfusion imaging in the United States. The American Society of Nuclear Cardiology in its position paper from March 1999 recommended the routine incorporation of ECG gating during SPECT cardiac perfusion scintigraphy (1,2). Gated SPECT studies allow simultaneous assessment of perfusion and function in a single-injection, single-acquisition sequence.
The development of new radioisotopes and improvements in imaging hardware and computer technology have contributed significantly to the growth of gated SPECT. The 99mTc-based perfusion tracers, because of their higher count rates and stable myocardial distribution with time, permit evaluation of regional myocardial wall motion and wall thickening throughout the cardiac cycle. The development of automated algorithms to quantitatively measure left ventricular (LV) volume and ejection fraction (EF), and even regional myocardial wall motion and thickening from gated SPECT, rapidly and accurately, and with minimal operator interaction, has also contributed to its widespread use. These innovations have made SPECT imaging a premier method of noninvasive evaluation of myocardial blood flow and cardiac function in a variety of clinical situations (3).
GATED SPECT ACQUISITION AND PROCESSING
In a gated acquisition, a 3-lead ECG provides the R wave trigger to the acquisition computer, with 2 successive R wave peaks on the ECG defining a cardiac cycle. Counts from each phase of the cardiac cycle are associated with a temporal frame within the computer (4). Gating of myocardial perfusion is usually performed at 8 frames per R—R interval per projection, although most manufacturers have the capability to acquire 16 frames per R—R interval. The acquired data are then reconstructed and displayed in a cinematic or multiframe format, allowing the reader to assess wall motion in all areas of the myocardium, including the left and right ventricles (Fig. 1) (5).
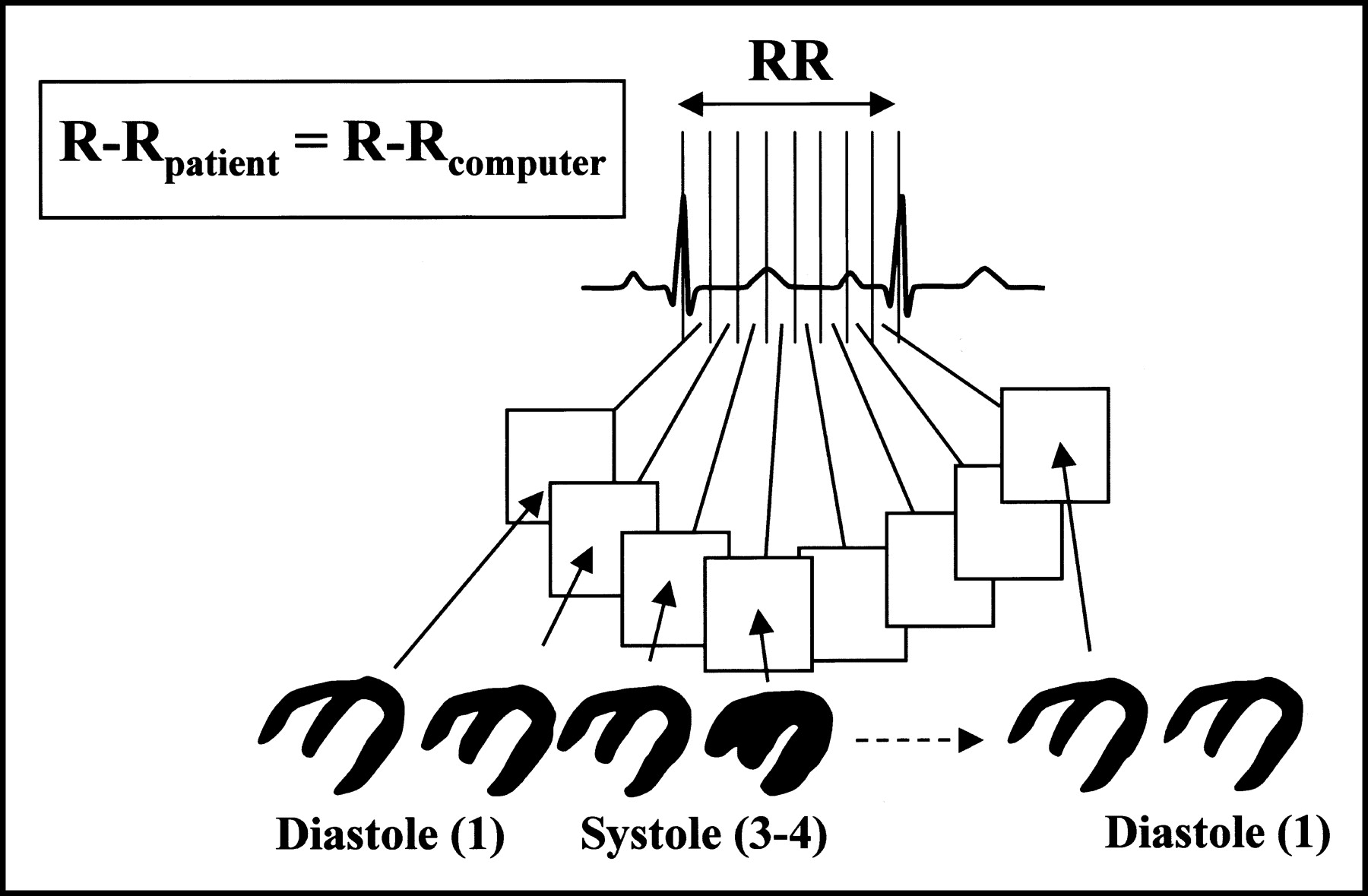
ECG-gated SPECT acquisition. Separate temporal frames corresponding to different phases of cardiac cycle are acquired for each angular projection. Perfusion images are obtained from summation of individual frames. (Reprinted with permission of (5).)
Changes in heart rate due to a variety of factors can result in temporal blurring—that is, mixing of counts from adjacent frames. To minimize temporal blurring, a beat rejection window is set by specifying the acceptable deviation of each R—R interval from the expected value. A 20% window has historically been applied, although in patients with highly variable heart rates, up to a 100% acceptance window can be set. In patients with arrhythmias, it is important to check for gating errors, as it has been demonstrated that EF fluctuations, perfusion differences, and, in particular, wall thickening discordance may occur with arrhythmias (6). Thus, in cases of extreme variation in heart rate or rhythm, an ungated SPECT study may be the most appropriate test.
There are a variety of single-day and 2-d protocols that may be used in conjunction with gated SPECT. Either 201Tl or 99mTc perfusion tracers may be used. Most commonly used is the high-dose technetium stress study because of its superior myocardial count density. 99mTc-Sestamibi provides more reproducible volume and LVEF measurements than 201Tl (7). In addition, when low- versus high-dose technetium was compared there was less variability of LVEF in the high-dosage cohort (8).
Either or both of the acquisitions composing the stress/rest or rest/stress sequence can be gated. Although the common practice is to gate only the poststress image, a small study by Johnson et al. reports that, in 36% of patients with reversible perfusion defects, the poststress LVEF was >5% lower than at rest (9). This implies that global and regional LV function obtained from poststress gated acquisitions are not representative of basal LV function in patients with stress-induced ischemia and that perhaps both rest and stress images should be gated routinely, as long as counts are sufficient.
Overall ventricular function and regional cardiac function (myocardial wall motion and thickening) are calculated separately using computer software requiring minimal operator input (Fig. 2). Most of these programs use an edge detection method using endocardial and epicardial surface points and make geometric assumptions (gaussian fit) to calculate LV end-systolic and end-diastolic volumes. Other methods seek definition of the same points using the percentage systolic count increases because of the partial-volume effect. Newer programs are usually a hybrid of edge detection and count-based methods and are 3-dimensional (10–12). Visually the ventricular wall thickening can be accentuated with thermal or hot body imaging options.

Quantification of EF, regional myocardial wall motion, and thickening from gated myocardial perfusion SPECT (QPS; Cedars-Sinai). (A) Myocardial contours displaying endocardial and epicardial surfaces overlying end-diastolic (ED) and end-systolic (ES) frames display 3 short-axis images, a midcavity horizontal image, and a midcavity vertical long-axis image. (B) Quantitative polar plots measuring regional myocardial wall perfusion (B1, B2), motion (B3), and wall thickening (B4) from gated SPECT. (C) Three-dimensional display of endocardial (solid) and epicardial (grid) LV surfaces calculated by automatic algorithm. (D) Endocardial time—volume curve and calculated LVEF from end-systolic and end diastolic volumes.
CLINICAL APPLICATIONS
Ventricular Function
The 3 most widely distributed software packages for LV function analysis from gated myocardial perfusion scans are QGS (Cedars-Sinai), 4D-MSPECT (University of Michigan), and the Emory Cardiac Toolbox or ECTb (Emory University). The QGS methodology uses gaussian fit to determine endocardial and epicardial offsets, whereas ECTb is a count-based method. Although both programs have, in general, compared favorably with other modalities for determining LVEF and volumes (Tables 1 and 2), it is important to keep in mind that the choice of gold standard, as well as degree of rigorousness in comparing the different methodologies in these validation studies, may vary. Some modalities used for comparison, including 2-dimensional echocardiography, radionuclide ventriculography, and first-pass radionuclide angiography have their own inherent inaccuracies. It is also important to note that not all reports provided the statistical analysis of the variability around the correlation line, such as the SE of estimates, which indicates the likelihood that the EF measured by the new technique will be within a certain range of the EF measured by the gold standard. If there is a large range, this usually indicates that a study is not as reliable. Perfusion defects, background activity, time after injection, and the injected dose may have a confounding effect on the quantitative determination of LVEF and LV volumes, as demonstrated by a small study done in canines by Vallejo et al., which showed that the automated QGS program consistently overestimated LVEF and LV volumes when compared with MRI (13). Furthermore, since this was a canine study, it is postulated that perhaps in smaller hearts, the limited spatial resolution of SPECT makes endocardial border recognition problematic and that perhaps a count-based method would be more appropriate. A larger human study by the same author, comparing gated SPECT with first-pass radionuclide angiography, showed a better correlation in studies with low extracardiac activity, higher counts, and larger hearts (14). This emphasizes the critical importance of quality control and optimizing image acquisition, as well as awareness on the part of the reader to recognize the presence of such variables. A study by Nakajima et al., specifically examining pediatric hearts (age, 2 mo to 19 y) with correspondingly small LV volumes (14–326 mL), also emphasized that in patients with small ventricular volumes gated SPECT is valid if appropriate image acquisition parameters are used (15).
Validation of Quantitative Measurements of LVEF by Different Software Programs for Gated Myocardial Perfusion SPECT
Assessment of LVEF by 5 Methods: Range and Lower Normal Limits
Several studies have directly compared the performance of gated SPECT software packages. A comparison between QGS and ECTb showed that QGS consistently provided significantly lower volumes and EFs compared with the ECTb algorithm for both coronary artery disease (CAD) and low-likelihood patients (Table 3) but that both methods showed close correlation with each other (r = 0.91–0.94) (16). Lum and Coel demonstrated a correlation coefficient of >0.9 in estimating EF and end-diastolic volume among QGS, ECTb, and 4D-MSPECT (17). Nakajima et al. compared QGS, ECTb, and 4D-MSPECT with gated blood pool and observed correlation coefficients of 0.89, 0.85, and 0.90, respectively (18). Although several studies have shown high correlation between various gated SPECT software programs in estimation of ventricular volume, since each program uses a different algorithm, their LV function data should be interchangeable only with caution. In the situation in which the same gated SPECT software application is used twice consecutively on the same patient, there is high correlation for both wall motion (r = 0.95) and systolic thickening (r = 0.88) (19).
Comparison of 2 Software Programs for Quantitation of LV Function and Volumes in Normal or Low-Risk Subjects
Artifact Identification
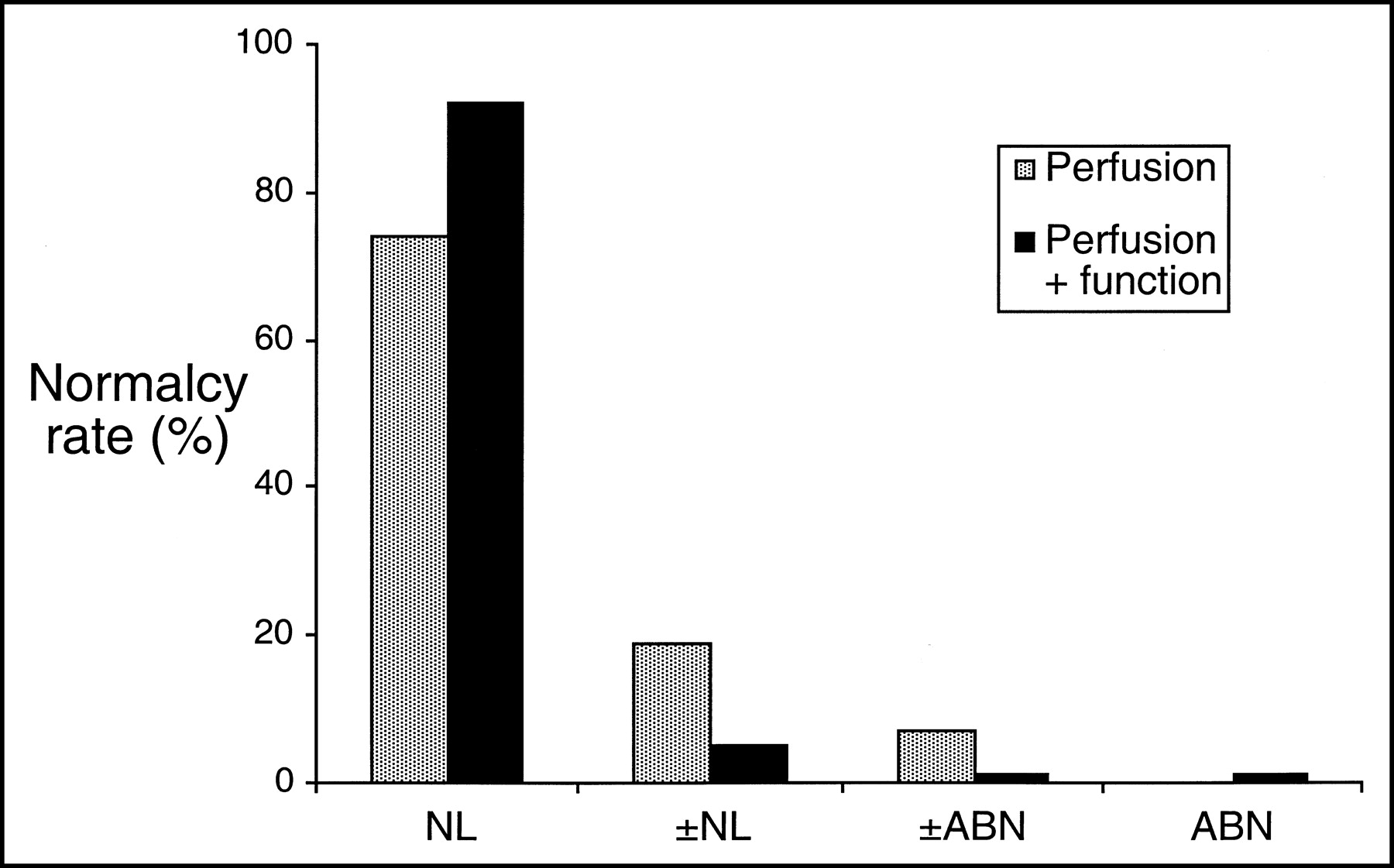
Initially, the clinical role of gated SPECT lay in its ability to enhance artifact identification. Soft-tissue attenuation artifacts often appear as fixed defects and are difficult to differentiate from infarct, thereby reducing the test specificity of SPECT myocardial perfusion imaging. Gated acquisitions may help differentiate scar from artifact as fixed defects with decreased function likely represent a myocardial infarction (MI), whereas attenuation artifacts will have a fixed defect with normal or relatively normal wall motion. DePuey and Rozanski demonstrated that false-positive perfusion studies could be reduced from 14% to 3% by incorporating regional wall motion data in the interpretation of perfusion imaging (20). In women, where the false-positive rate of stress ECGs is relatively high and breast soft-tissue attenuation artifact is common, ECG gating was shown to further enhance the diagnostic specificity of 99mTc perfusion imaging from 84% to 94% (21). Subsequently, Smanio et al. demonstrated that the addition of gated SPECT for the assessment of regional systolic function reduces the degree of uncertainty in the interpretation of 99mTc-sestamibi perfusion studies. The number of “borderline-normal” or “borderline-abnormal” interpretations was significantly reduced. In patients with a low likelihood of CAD, the normalcy rate increased from 74% to 93% (Fig. 3). In patients with a high likelihood of CAD, the trend was also toward a higher number of unequivocally abnormal interpretations (22).
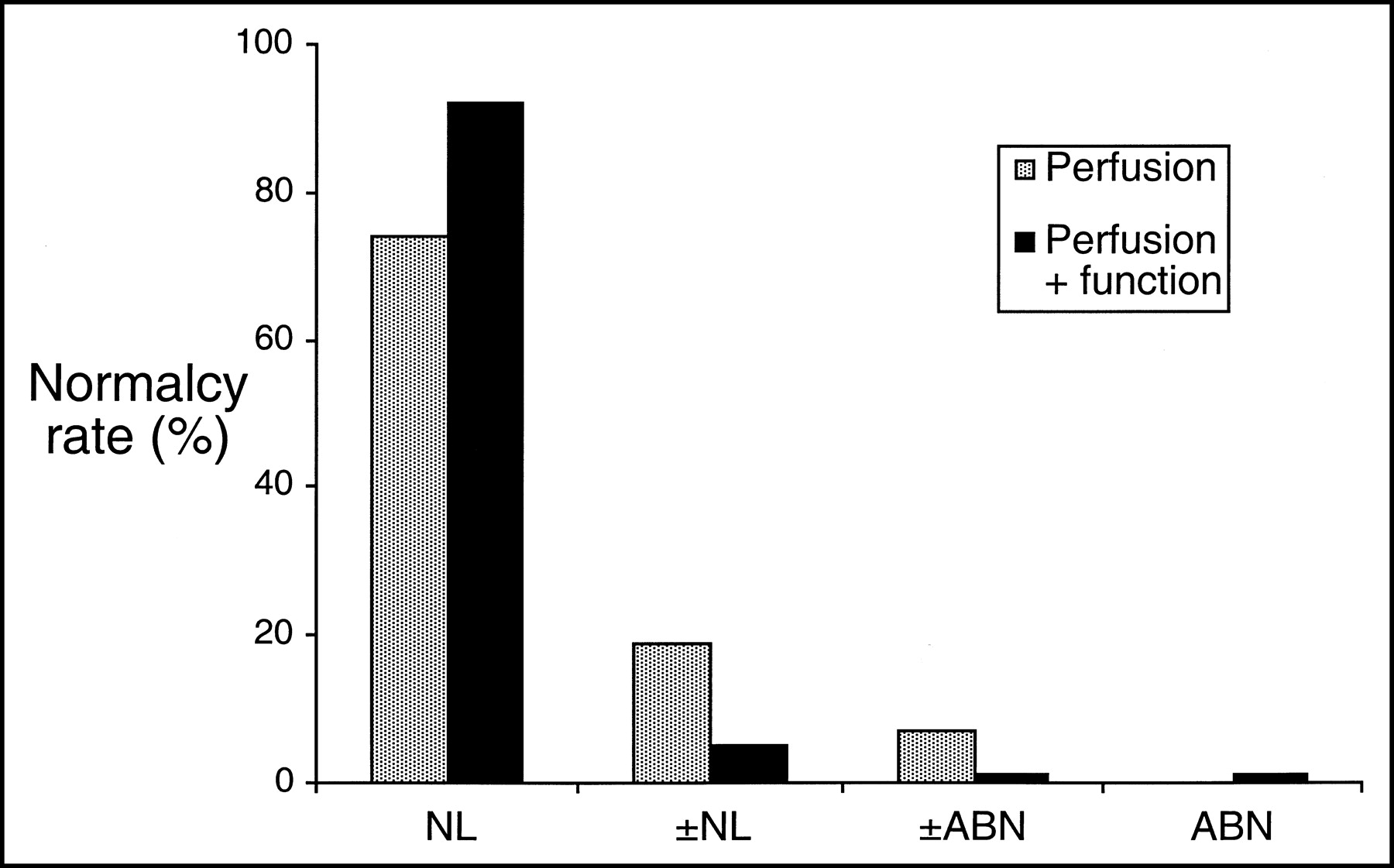
In patients with low likelihood of CAD, normalcy rate increased from 74% to 93%, and borderline readings decreased from 32% to 10% when functional data from gating are incorporated into study interpretation. NL = normal; ±NL = borderline normal; ±ABN = borderline abnormal; ABN = abnormal. (Modified and reprinted with permission of (22).)
Diagnosis of CAD
The detection of CAD, particularly multivessel disease, is also enhanced by the capability to obtain functional information through gating. Though proven in various studies that SPECT myocardial perfusion imaging reliably detects CAD, the question of underestimating ischemia in the case of multivessel disease or left main disease because of balanced global hypoperfusion comes into question. According to several reports, only 13%–50% of patients with 3-vessel CAD or left main disease actually have perfusion abnormalities in multiple territories (23–25). This could potentially lead clinicians to underestimate risk or incorrectly predict prognosis. Several studies have clearly demonstrated the incremental value of using both functional and perfusion data in detecting multivessel disease or high-grade stenoses over perfusion data alone, although there are some conflicting data on sensitivity and specificity. Sharir et al. examined a population of 99 patients who underwent dual-isotope resting 201Tl/exercise gated 99mTc-sestamibi SPECT with normal resting perfusion. Multivariate regression analysis showed that both extensive perfusion abnormalities and the presence of wall motion abnormalities in multiple territories were independent predictors of severe multivessel CAD but that the addition of wall motion variables to perfusion data resulted in a significant increase in the global χ2 for predicting severe proximal left anterior descending as well as severe multivessel CAD. For perfusion alone, sensitivity was 49%, whereas combined perfusion and wall motion abnormality yielded a sensitivity of 82% (26). Lima et al. demonstrated that evaluation of segmental poststress thickening abnormalities on gated SPECT better identified patients with severe angiographic triple-vessel disease. The addition of functional data derived from gated SPECT to perfusion data improved detection of multivessel disease from 46% to 60% (P < 0.05) and triple-vessel disease from 10% to 25% (P < 0.001) (27).
The use of rest and stress LVEF may also assist in the detection of multivessel coronary disease, as demonstrated in a study by Yamagishi et al., wherein the combination of perfusion data and worsening of the LVEF significantly increased sensitivity in detecting multivessel CAD over 201Tl perfusion defects or rest LVEF and postexercise LVEF alone (43.3% vs. 26.9%, 25.4%, and 25.4%, respectively). In this study, though sensitivity increased, there was also a significant decrease in specificity, although this remained acceptable at approximately 90% (28). Another study sought to correlate the degree of angiographic stenosis with the presence of regional wall motion abnormalities (RWMA) on exercise stress/rest gated 99mTc SPECT studies (29). Reversible RWMA were found to be highly specific for angiographic stenoses of >70%, both overall and for specific vascular territories (94%–100%). Furthermore, when patients were stratified according to the severity of angiographic stenoses (50%–79% and 80%–99%), the presence of reversible RWMA distinguished a higher angiographic severity with positive predictive values between 77% and 88% for specific vascular territories. Of note, these improvements in specificity were at the expense of sensitivity, which were much less compared with perfusion alone (53% for reversible RWMA vs. 89% for perfusion alone).
In addition, diastolic dysfunction on poststress gated SPECT imaging has been shown as an indicator of CAD (30,31). Poststress diastolic dysfunction is though to be a manifestation of myocardial ischemia causing increased early filling pressures. Indices of diastolic dysfunction include peak filling rate (PFR) and time to PFR of the left ventricle. PFR computed by gated SPECT using 8 frames per R—R interval has a poor correlation of 0.51 compared with equilibrium radionuclide angiography (ERNA) (30). The correlation improves if more frames are used. Paul et al. measured diastolic parameters through gated SPECT and found that PFR was lower in poststress patients with severe reversible scintigraphic perfusion defects compared with rest images (2.23 s−1 and 2.94 s−1; P < 0.005) (31). Yet, other parameters such as LVEF, end-diastolic volume, and end-systolic volume were also all significantly lower in the same patient groups. Although gated SPECT allows observations of diastolic dysfunction, this parameter does not currently have incremental diagnostic value over existing standards.
Prognosis and Risk Stratification
As with the case with perfusion imaging in general, gated SPECT imaging has also found an important role in the risk assessment of patients with known or suspected CAD. This is not surprising, given the well-recognized prognostic role of LV function with regard to long-term survival, as has been shown using a variety of techniques for LV functional assessment. Among a large series of 1,690 consecutive patients who underwent dual-isotope gated SPECT imaging, those whose EFs were <45% were associated with reduced survival, irrespective of the perfusion defect size or severity. Additionally, those patients with normal end-systolic volumes of <70 mL or an EF of >45% had a very low cardiac mortality rate, despite severe perfusion abnormalities (Fig. 4) (32). This group also examined the relative value of perfusion and function in the risk stratification in 2,686 patients into low-, intermediate-, and high-risk categories for cardiac death and MI (33). LVEF was most predictive of death and the amount of ischemia (summed difference score on perfusion imaging) was the best predictor of nonfatal MI. Functional information was found to be of incremental value in the prediction of cardiac death beyond the perfusion imaging parameters. Interestingly, the presence of ischemia did not influence prognosis in patients with LVEFs of <30%, due to the already high mortality rate.

Annual cardiac death rates stratified by LV volume and EF. Patients with LVEF of ≥45% or end-systolic volume (ESV) of <70 mL have low mortality rate regardless of severity of perfusion defects. Similar findings are noted for patients with low EF (<45%). (Modified and reprinted with permission of (32).)
After an acute MI, LV function has long been a key determinant for survival. Recently, a study of 128 postinfarct survivors confirmed the value of gated SPECT imaging for risk stratification in post-MI patients, as an LVEF of <40% with this method was found to increase the risk of a subsequent cardiac event by almost 3-fold (34). Interestingly, neither the presence of a fixed or reversible defect had independent predictive value in this study, although the latter finding may be a result of the censoring of high-risk patients who underwent early revascularization.
ECG-gated SPECT is also commonly used for preoperative risk stratification for noncardiac surgery. A study done by Hashimoto et al. assessed the relationship between perioperative cardiac events and various predictors, including clinical factors, perfusion, and functional assessment using the QGS program to assess LV function and estimate regional wall motion. Multivariate analysis demonstrated functional analysis to be an independent predictor of perioperative cardiac events. Function and wall motion assessment proved especially useful in patients with normal perfusion scans (35).
Ischemic Cardiomyopathy and Viability Determination
In patients with dilated cardiomyopathy, the distinction between an ischemic and nonischemic etiology has clinical relevance and may greatly affect management decisions. Danias et al. demonstrated that ischemic and nonischemic cardiomyopathy can be reliably distinguished from each other noninvasively with gated SPECT imaging. Summed stress scores and the amount of regional variability in function are greater in ischemic cardiomyopathies than in nonischemic cardiomyopathies and this is an important parameter in distinguishing between these broad categories (36).
In patients with CAD and LV dysfunction, the issue of myocardial viability is often highly relevant in the decision-making process regarding revascularization. Several modalities have been studied and used for the assessment of viability, including 201Tl stress—redistribution, rest—redistribution, or reinjection scintigraphy with either 201Tl or 99mTc-sestamibi (37–44), low-dose dobutamine echocardiography (45), contrast-enhanced MRI, and 18F-FDG PET (46–48). Although 18F-FDG PET is widely considered the gold standard, with sensitivities ranging from 71% to 100%, a recent meta-analysis by Bax et al. showed no clear advantage of one technique over another (49). The principal limitation of 18F-FDG PET is the fairly high cost of the equipment, thus limiting its availability in all medical centers. Other modalities are usually used to determine viability before using PET. The addition of functional information provided by ECG gating is thought to have an incremental value for the prediction of viability over perfusion studies alone. In a small study by Levine et al., perfusion and wall motion combined significantly improved the sensitivity and accuracy for the prediction of viability, as defined by an ≥20% improvement in perfusion or function when compared with perfusion imaging alone (95% vs. 86% sensitivity, 91% vs. 85% accuracy). Specificity remained the same at 55% (50). In another trial, gated SPECT 99mTc-tetrofosmin assessment of wall thickening (rather than wall motion) combined with perfusion data increased the sensitivity for assessment of viability, using 18F-FDG PET as the gold standard, from 79% to 85% but decreased the specificity from 79% to 56% (51). Other investigators have demonstrated that the assessment of wall thickening on gated SPECT may have its impact on improved specificity with regard to postrevascularization recovery of regional function, depending on tracer activity on perfusion. When segments with >50% tetrofosmin activity have detectable wall thickening, there is a higher likelihood of functional improvement when compared with segments with no contractile function; however, in segments with <50% tracer activity, there was no significant difference (52). It is important to note that though these particular studies demonstrate an advantage of combined function and perfusion assessment, the actual sensitivities and specificities are not significantly different from the weighted mean sensitivities and specificities of the meta-analysis (49), and most of these studies have small populations and varied study designs.
Low-dose dobutamine has been used successfully to demonstrate contractile reserve for many imaging modalities, including echocardiography (45), radionuclide angiography (53), MRI (54), and, most recently, gated SPECT imaging (55–57). Gated SPECT has shown the increase in contractile function that accompanies low-dose dobutamine, with the LVEF increasing from 14% to 46% at baseline to 23%–71% and 25%–85% at 5 and 10 μg/kg/min of dobutamine infusion (58). Viability measurements based on contractile reserve have higher specificity than perfusion imaging overall; this finding has been confirmed for gated SPECT imaging as well. In a study by Leoncini et al., the use of low-dose dobutamine gated SPECT significantly improved the specificity and overall accuracy for predicting functional recovery after coronary revascularization. The visual assessment of regional function after low-dose dobutamine was especially useful for hypokinetic segments, where the specificity for postrevascularization functional improvement increased to 94% as compared with 23% for perfusion imaging. However, the sensitivity for prediction of improvement in akinetic regions was inferior with dobutamine gated SPECT compared with quantitative perfusion imaging (Fig. 5). This study suggests a combined approach, using data from both contractile reserve and quantitative tracer activity (55). In the same series, they also assessed global LV function with low-dose dobutamine infusion as a predictor of postrevascularization functional improvement and found that gated SPECT had a predictive value similar to that of echocardiography (59). An increase in the LVEF of >5 EF units was found to be a good predictor of improvement in EF after revascularization (56). Again, it is important to note that the main limitation of these studies, as well as other studies looking at functional recovery, is the small population size.
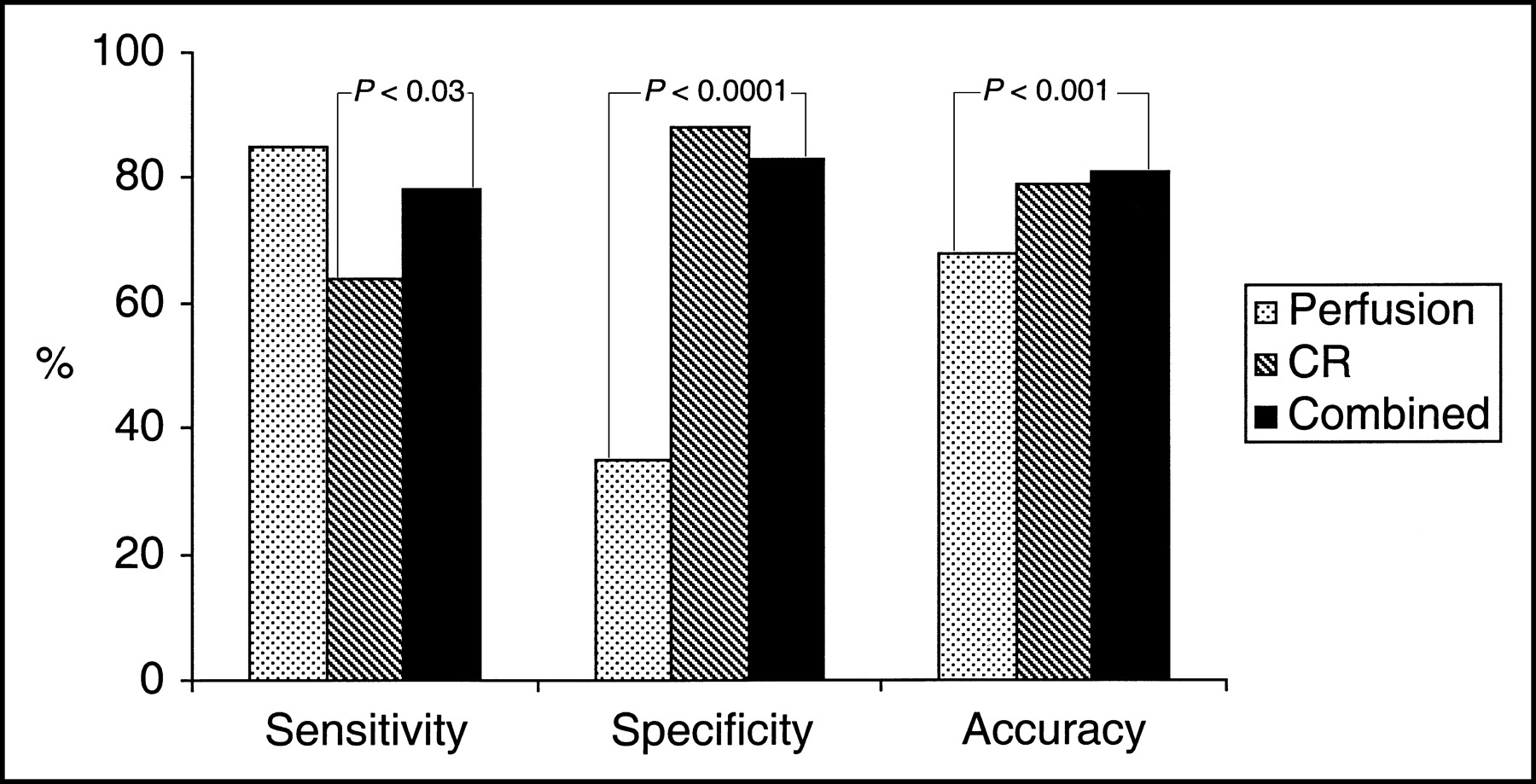
Prediction of functional recovery with nitrate-enhanced 99mTc-sestamibi dobutamine gated imaging. For all asynergic segments, using combination of tracer activity and contractile reserve (black bars; combined) improved specificity and overall accuracy significantly when compared with perfusion quantification alone (stippled; perfusion). Sensitivity was not altered significantly with combined approach but was higher than using contractile reserve alone (hatched bars; CR). (Modified and reprinted with permission of (55).)
Other Diagnostic Applications
Aside from its well-studied applications in determining systolic function, attempts have been made to expand the clinical applications of ECG-gated SPECT imaging. Echocardiography has been the most commonly used method for assessing LV diastolic function. Radionuclide techniques, specifically equilibrium radionuclide angiography, have more recently been applied as well. Several diastolic parameters have been used, including PFR, which measures the most rapid change in ventricular counts in early-to-mid diastole, the time to peak filling (the time interval from the nadir of LV counts to the moment of the PFR), and the filling fraction (percentage of filling that has occurred at one third, one half, and two thirds of diastole). A small study has applied ECG-gated SPECT to assess the same diastolic parameters (specifically PFR), and found a close correlation between PFR generated by and gated SPECT using a higher frame rate of 32 frames per cardiac cycle (the most commonly used frame rate is 8 frames per cycle) (30). In another study, the diastolic parameters of a small group of patients with systemic sclerosis were examined using gated SPECT, and again a closer correlation and higher accuracy was found when using 16 frames per cycle (60). Both of these studies used 3-detector SPECT systems. These findings are consistent with the concept that accurate assessment of diastolic function by radionuclide techniques requires a high temporal resolution and reliability of the diastolic filling phase of the time–activity curve. In addition, the fidelity of the diastolic filling phase of the time–activity curve is also affected by the traditional problems associated with gating based on R—R interval, such as arrhythmias or premature ventricular contractions, and thus alternative acquisition modes (such as list mode acquisition) or “bad-beat rejection” filters have to be applied. These technical considerations have currently limited the usefulness of gated SPECT for assessment of diastolic function.
Another potential underdeveloped application of gated SPECT is the assessment of right ventricular size and wall motion. In a case report, an unsuspected pulmonary embolism was diagnosed when unexplained right ventricular dilatation and hypokinesis was detected on gated SPECT imaging (61). More studies are definitely warranted for this application, but routine examination of right ventricular size and motion when interpreting studies may provide additional clinical information.
CONCLUSION
Gated SPECT imaging has attained widespread use because it provides a wealth of additional information that is useful not only to the reader interpreting myocardial perfusion imaging studies but also to the referring clinician. Although the major benefit of perfusion imaging has been its ability to improve artifact recognition, the use of functional information also improves the detection of severe and extensive coronary disease, provides independent and incremental prognostic information, and aids in the evaluation of myocardial viability. Novel applications have also been described and unique values of this technique will undoubtedly continue to evolve.
Footnotes
Received Jun. 23, 2003; revision accepted Jan. 7, 2004.
For correspondence or reprints contact: Robert C. Hendel, MD, Section of Cardiology, Department of Medicine, Rush-Presbyterian-St. Luke’s Medical Center, 1725 W. Harrison St., Suite 020, Chicago, IL 60612-3864.
E-mail: Robert_C_Hendel{at}rush.edu
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Prognostic Value of Myocardial Perfusion Imaging by Cadmium Zinc Telluride Single-photon Emission Computed Tomography in Patients with Suspected or Known Coronary Artery Disease A Systematic Review and Meta-analysis
- Clinical Utility of Enhanced Relative Activity Recovery on Systolic Myocardial Perfusion SPECT: Lessons from PET
- Assessment of Severity of Coronary Artery Stenosis in a Canine Model Using the PET Agent 18F-Fluorobenzyl Triphenyl Phosphonium: Comparison with 99mTc-Tetrofosmin
- Detection of an occult thymoma on 99Tcm-Tetrofosmin myocardial scintigraphy
- Intramyocardial Implantation of Bone Marrow-Derived Stem Cells Enhances Perfusion in Chronic Myocardial Infarction: Dependency on Initial Perfusion Depth and Follow-up Assessed by Gated Pinhole SPECT
- Initial Infarct Size Predicts Subsequent Cardiac Remodeling in the Rat Infarct Model: An In Vivo Serial Pinhole Gated SPECT Study
- Positron Emission Tomography-Measured Abnormal Responses of Myocardial Blood Flow to Sympathetic Stimulation Are Associated With the Risk of Developing Cardiovascular Events
- Gated Myocardial Perfusion SPECT: Basic Principles, Technical Aspects, and Clinical Applications