


Abstract
Event rates associated with a normal or low-risk myocardial perfusion SPECT imaging study have been shown by numerous investigators to be associated with <1%/y of follow-up. Thus, the aim of this study was to evaluate the prognostic value of a normal 99mTc-tetrofosmin study in a geographically diverse registry of patients undergoing stress myocardial perfusion SPECT. A total of 4,728 consecutively tested patients who underwent stress 99mTc-tetrofosmin SPECT at 5 U.S. hospitals were included in this series. Methods: Patients were monitored for the occurrence of major cardiac events and hospitalizations. Uniform methods of data collection and standardized epidemiologic methods for follow-up were used at all centers. We used a risk-adjusted, Cox proportional hazards model to assess time to cardiac death. Results: Of the 4,728 patients, one third underwent adenosine stress SPECT and two thirds underwent treadmill exercise. The observed annualized survival rate for those patients with a normal 99mTc-tetrofosmin study was 0.6%. Similarly, excellent survival rates were noted for the male and female subsets of this population as well as for patients who could exercise and for those undergoing pharmacologic stress testing. Compared with prior published outcomes studies on stress 201Tl or 99mTc-sestamibi SPECT, the overall survival rates were similar and ranged from 99.3% to 99.7%. Conclusion: Results from this large multicenter registry provide further supportive evidence that the excellent prognosis associated with a normal SPECT scan is independent of the radiopharmaceutical used.
Prior research has revealed that event rates associated with normal or low-risk myocardial perfusion SPECT imaging with 201Tl or 99mTc-sestamibi have been shown by numerous investigators to be <1%/y of follow-up (1–9). This uniformly low event rate is critical when applying myocardial perfusion imaging information to risk stratification. For patients who are at low risk of major cardiac events with a normal perfusion scan, a conservative approach to posttest patient management is expected. To date, few prognostic data are available with the commonly used radioisotope 99mTc-tetrofosmin (10–12).
Thus, the aim of this study was to evaluate the prognostic value of a normal 99mTc-tetrofosmin study in a geographically diverse registry of patients undergoing stress myocardial perfusion SPECT. This initial phase of research is part of an ongoing multicenter registry to determine the relationship between the extent and severity of myocardial perfusion defects with 99mTc-tetrofosmin SPECT and important clinical outcomes.
MATERIALS AND METHODS
Patients
A total of 4,728 consecutively tested patients who underwent stress 99mTc-tetrofosmin SPECT at 5 U.S. hospitals were included in this series. Patients were included in this series if they were referred for myocardial perfusion tomographic imaging at each of the participating sites and if their stress perfusion scan was considered normal or low risk (defined as a summed stress score of <4). Details of the image interpretation are provided below. This referral series includes patients who were outpatients with medically stable chest pain (or anginal equivalent) symptoms for the evaluation of suspected cardiac ischemia or for the evaluation of prior coronary disease. All patients were at intermediate–high risk of coronary disease defined as a range of presentation from the presence of typical chest pain symptoms, >1 traditional risk factor (except diabetes, which is now considered a high-risk equivalent), to established coronary disease determined by coronary angiography or prior hospitalization. Patients who were undergoing risk stratification before discharge, those with unstable angina, or early evaluations after discharge were excluded. Participating institutions included Rush–Presbyterian–St. Luke’s Hospital (Chicago, IL), Duke University Medical Center (Durham, NC), University of California Los Angeles Medical Center (Los Angeles, CA), and Emory University–VA Hospital (Atlanta, GA).
Exercise Testing Protocol
The exercise testing protocol included graded exercise (n = 3,168 patients) with a Bruce or modified Bruce protocol or intravenous adenosine (n = 1,560 patients) using standard procedures (1–9). Patients performed incremental exercise testing until the occurrence of fatigue or ≥85% predicted maximal heart rate. Stress testing was terminated for severe chest pain, ventricular tachycardia or ventricular fibrillation, ST segment elevation in a non-Q wave lead, or ≥3 mm of ST segment depression or with the completion of the pharmacologic stress protocol.
SPECT
SPECT was performed using a dual-isotope protocol with rest 201Tl and stress 99mTc-tetrofosmin at 3 sites or a same-day or 2-d 99mTc-tetrofosmin imaging protocol at 1 site. For the single-day tetrofosmin protocol, 296–370 MBq (8–10 mCi) 99mTc-tetrofosmin were injected at rest and 814–925 MBq (22–25 mCi) were injected at near-peak exercise. The dual-isotope studies used a resting dose of about 129.5–166.5 MBq (3.5–4.5 mCi) 201Tl and 740–1,295 MBq (20–35 mCi) 99mTc-tetrofosmin after stress. The SPECT acquisition was acquired at rest and after peak exercise using a circular orbit (180° for 3 sites; 360° at 1 site), in a 64 × 64 matrix. Specific acquisition parameters were dependent of the camera at each institution (Elscint [Haifa, Israel], Siemens Medical Systems [Hoffman Estates, IL], ADAC Laboratories [Milpitas, CA], and General Electric Medical Systems [Milwaukee, WI]). Image processing was performed in a manner standard to each institution, using a Butterworth filter in all cases. All image sets (horizontal and vertical long-axis and short-axis planes) were normalized to the maximal myocardial activity in that set and displayed in the standard American College of Cardiology orientation.
Two or more experienced observers who were blinded to clinical history and physical examination data reviewed all scans. In the case of a discordant opinion, a third reviewer was used to achieve a consensus opinion on the interpretation. Stress images were compared with rest images.
Each site used the same method for image interpretation including the fact that a semiquantitative scoring system, in which each of 20 segments is scored according to a 5-point scheme, was used to provide a systematic and reproducible method for scan interpretation. The 20-segment scoring system uses 3 short-axis slices (distal [apical], mid, and basal) of the left ventricle, with the apex represented by 2 segments visualized on a midvertical long-axis image (1). Each segment is scored as follows: 0 = normal, 1 = slight reduction of uptake, 2 = moderate reduction of uptake, 3 = severe reduction of uptake, and 4 = absence of radioactive uptake. For this analysis, all patients had a low-risk SPECT scan, defined as a summed stress score of <4, which is considered normal or nearly normal (3–7).
Patients were monitored for the occurrence of major cardiac events and hospitalizations. Individuals blinded to historic and testing data confirmed events. Uniform methods of data collection and standardized epidemiologic methods for follow-up were used at all centers. Follow-up was complete in 97% of surviving patients. Patients lost to follow-up did not statistically differ with regard to their clinical characteristics from patients with completed follow-up.
Primary Data Analysis
The primary endpoint for this analysis was time to cardiac death. We examined independent estimators of cardiac death in this population with a normal or low-risk scan undergoing 99mTc-tetrofosmin SPECT. Using existing site databases, we derived a comparative consecutive series of patients referred for myocardial perfusion SPECT (The Cleveland Clinic Foundation, Emory University, and Duke University Medical Center) and included a consecutive series of patients undergoing stress 201Tl (n = 3,257) and 99mTc-sestamibi (n = 2,423) SPECT who had low-risk myocardial perfusion scans (13). Cox proportional hazards modeling techniques were used to develop a model estimating time to cardiac death. Risk-adjusted multivariable models for the stress nuclear results were developed controlling for age, sex, and type of stress (exercise vs. intravenous adenosine). Model overfitting procedures were considered and included 1 variable for every 5–10 clinical outcomes.
Meta-Analysis
We performed a Medline search of prognostic series using 201Tl or 99mTc-sestamibi that included multicenter observational series or prior meta-analysis published in English and using an adult population of women and men. Key words for the search included “coronary disease/ri”, SPECT, and prognosis. Clinical trials on pharmaceutical agents were excluded (n = 26). Abstracts from a total of 97 published reports were reviewed. From this group of 97 reports, 3 prior series in large observational studies or multicenter registries were reported (7–9). From each report, the annualized cardiac death rate for normal or low-risk SPECT scans was determined. Using a random effects (i.e., Empirical Bayes) model, a weighted average probability of survival was calculated (13).
RESULTS
Clinical Characteristics
Of the 4,728 patients, nearly half were male, with an average age of 61 y (Table 1). One third of the patients had a prior history of coronary disease. Referral for typical angina occurred in 54% of patients and atypical angina occurred in 35% of patients. Cardiac risk factors were prevalent in this series, including hypertension in 50% of patients, diabetes in 16% of patients, and current smoking in 23% of patients. Additionally, one third of the patients underwent pharmacologic stress imaging, with the remaining two thirds of patients undergoing exercise stress testing (Table 2). Only 12% of the population had an ischemic response to stress, and exertional chest pain occurred in 19% of patients. These population characteristics were typical of prior series of patients referred for SPECT (1–4).
Clinical Characteristics of Study Population (n = 4,728 Patients)
Exercise and SPECT Characteristics of Study Population (n = 4,728 Patients)
Unadjusted and Risk-Adjusted Cardiac Survival Rates
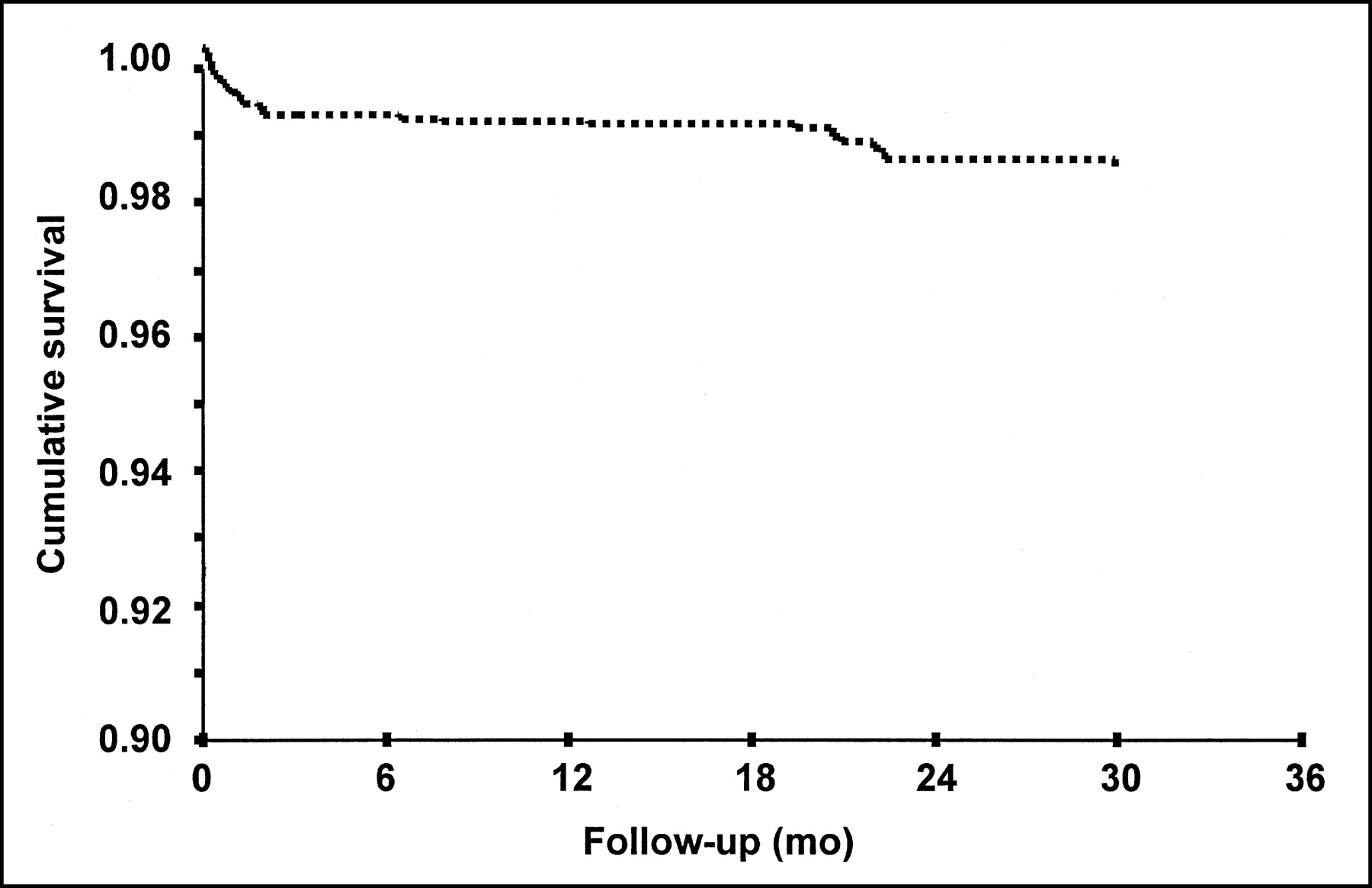
The observed cardiac mortality rate for those patients with a normal 99mTc-tetrofosmin study was 1.4% over 30 mo of follow-up (Fig. 1), with an annualized cardiac death rate of 0.6%. When controlling for age, sex, and the type of stress (i.e., exercise or pharmacologic stress), overall cardiac survival exceeded 99.5%.
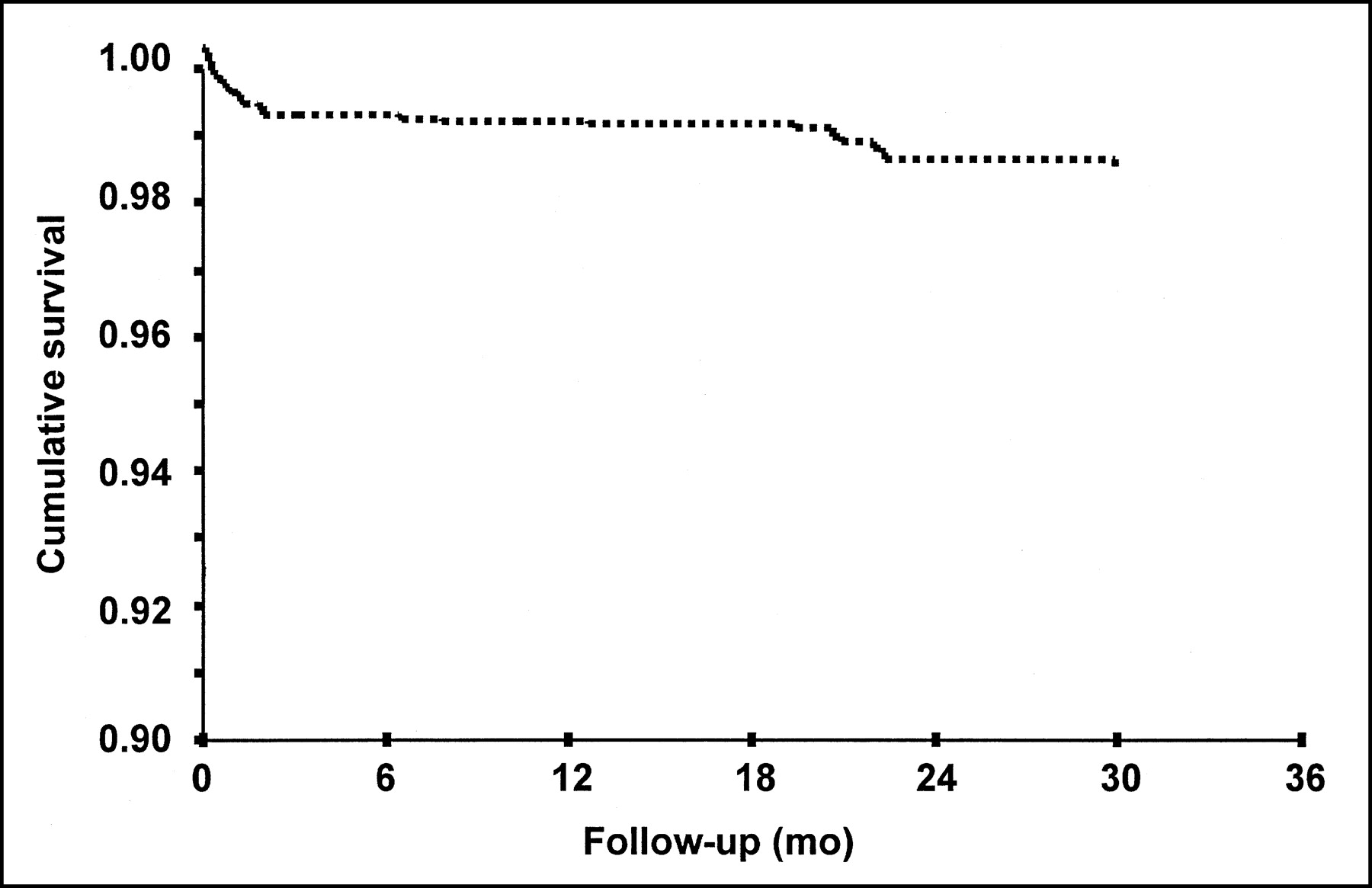
Risk-adjusted (controlling for age, sex, and type of stress performed) Cox survival curve in patients with normal 99mTc-tetrofosmin SPECT. Over 30 mo of follow-up, cumulative survival was 98.6%.
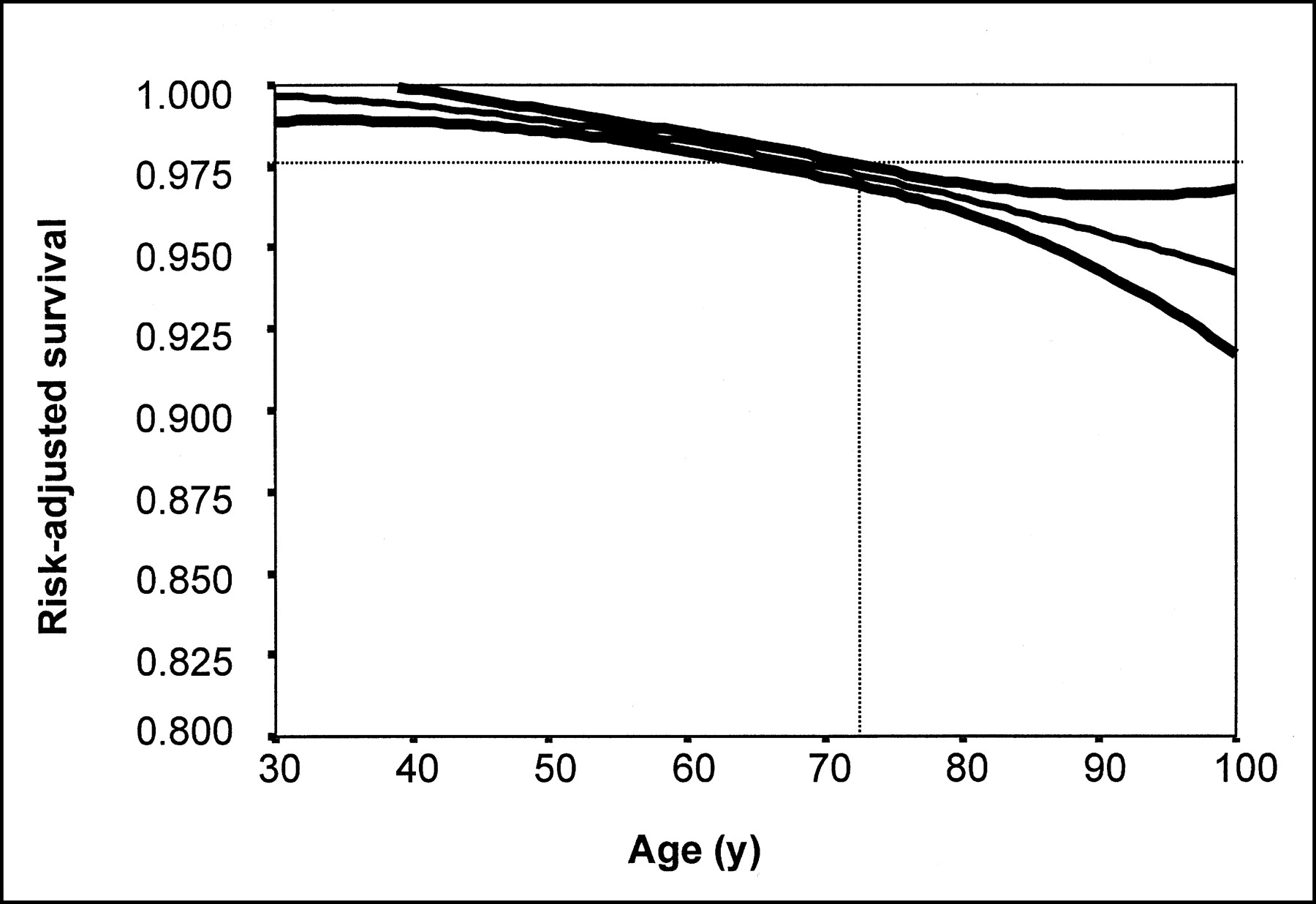
We then examined differential survival in key clinical subsets. For women and men, the average cardiac survival was 99.4% and 98.8%, respectively (P = 0.03). Additionally, for patients performing exercise, the annualized cardiac survival was 99.4%. Among the one third of patients undergoing adenosine stress SPECT, unadjusted cardiac survival was lower at 98.5% (P < 0.001; Table 3) but lost statistical significance when controlling for age, sex, and prior history of coronary disease (P > 0.11). Other important patient subsets included those with a history of coronary disease (30-mo survival = 98.7%), prior myocardial infarction (98.6%), and prior coronary bypass graft surgery (98.8%). In this cohort with low-risk 99mTc-tetrofosmin SPECT scans, the presence of peak exercise ST segment depression was not predictive of cardiac death (P = 0.9). Figure 2 depicts variability in cardiac survival by age groups. For patients <70 y old, the overall 30-mo cardiac mortality was 2.5% (or 1.0%/y of follow-up). However, cardiac mortality increased for patients of advanced age (and a greater frequency of comorbidity) to 1.6%/y–2.0%/y of follow-up for those patients aged 80–100 y (P < 0.0001). Similarly, excellent survival rates were noted for the male and female subsets of this population as well as for patients who could exercise and for those undergoing pharmacologic stress testing.

Risk-adjusted (controlling for age, sex, and type of stress performed) Cox survival curve in normal 99mTc-tetrofosmin SPECT by age of patient. Scatter plot of predicted survival by patient age is depicted. As patient age increases, there is general decline in 30-mo survival. Because of increasing comorbidity, risk factors, and disease prevalence, at ≥73 y old, there is substantial increase in mortality in patients with normal 99mTc-tetrofosmin SPECT.
Average 30-Month Survival in Key Patient Subsets Including Women, Men, Exercise, Known Coronary Disease, and Type of Stress (Intravenous Adenosine or Exercise) 99mTc-Tetrofosmin SPECT
Matched Comparison with 201Tl and 99mTc-Sestamibi
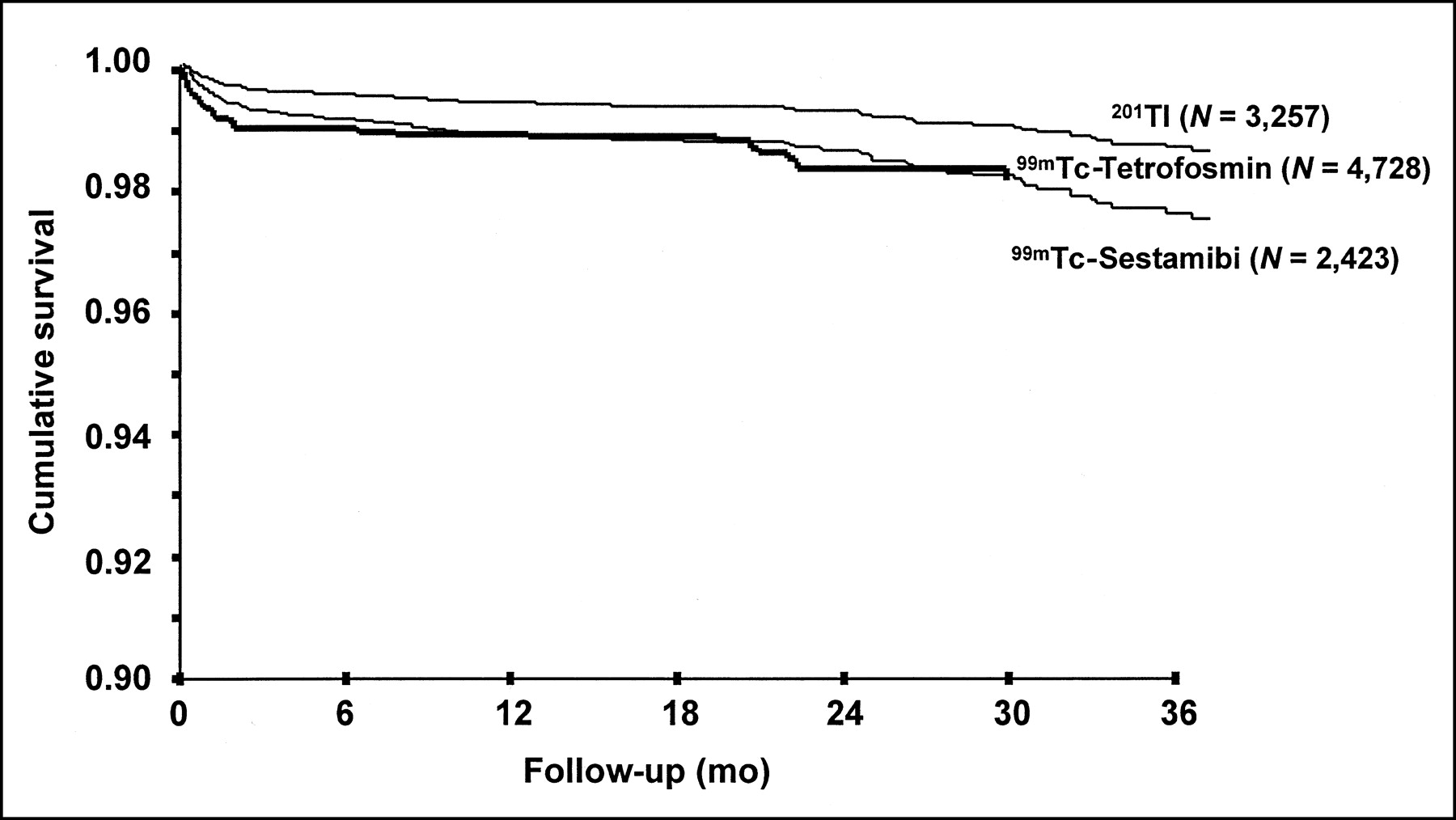
We combined the current series of patients undergoing 99mTc-tetrofosmin SPECT with that of prior prognostic series using 201Tl or 99mTc-sestamibi for a total of 10,408 patients (2,423 patients referred for 201Tl and 3,257 patients referred for 99mTc-sestamibi imaging). The cardiac death model that included age, sex, and type of stress (intravenous adenosine vs. exercise) survival model was significant (model χ2 = 42; P < 0.0001). In a stepwise Cox regression model, age was the single greatest determinant of cardiac death (P < 0.0001). Additionally, sex was a significant estimator of mortality (P = 0.026). However, cardiac survival did not differ for 99mTc-tetrofosmin SPECT when compared with imaging using the other isotopes (P > 0.9) (Fig. 3).

Risk-adjusted (controlling for age, sex, and type of stress performed) Cox survival curve in patients with normal 201Tl, 99mTc-sestamibi, and 99mTc-tetrofosmin SPECT. Similar survival rates were noted for all 3 isotopes—that is, at 3 y, ≥98% of patients with normal or low-risk perfusion scan were alive.
Meta-Analysis
When compared with prior published outcomes studies on stress 201Tl or 99mTc-sestamibi SPECT, the overall survival rates ranged from 99.3% to 99.7% (Fig. 4) (6,9,10). The results of our series revealed similarly excellent survival with 99mTc-tetrofosmin (annualized survival rate = 99.4%). A comparison of annualized survival between normal 201Tl, 99mTc-sestamibi, and 99mTc-tetrofosmin SPECT was nonsignificant (P > 0.20). The annualized cardiac survival rate in normal or low-risk SPECT scans using 201Tl or 99mTc-sestamibi ranged from 99.5% to 99.7%. Annualized cardiac survival rates did not differ between 201Tl or 99mTc-sestamibi and 99mTc-tetrofosmin (P > 0.20); survival = 99.54% (95% confidence interval [CI] = 99.31%–99.71%) for all 3 isotopes.

Meta-analysis of annualized cardiac death rates in normal or low-risk 201Tl, 99mTc-sestamibi, and 99mTc-tetrofosmin SPECT. Published evidence in large observational series of ≥1,000 or in prior multicenter registries is depicted. Of 4 published reports ((7–9) and this study) in ∼30,000 patients, survival in patients with normal or low-risk scan exceeded 99.3%/y. Meta-analysis revealed that annualized cardiac death rate was 99.5% (95% CI = 99.3%–99.7%).
DISCUSSION
Current state-of-the-art interpretation of myocardial perfusion SPECT uses risk stratification based on imaging results (14). Risk stratification with radionuclide perfusion imaging is powerful because the major determinants of cardiovascular disease prognosis are assessed by measurements of SPECT, including the amount of infarcted myocardium and the amount of jeopardized myocardium. This study used a risk-based approach to the interpretation of the 99mTc-tetrofosmin SPECT, including estimation of cardiac death for those with a normal or low-risk scan (based on the summed stress score). This evidence is critical because of the paucity of data on clinical outcomes using this radioisotope (10–12).
Risk stratification is essential to the development of evidence-based strategies for improved patient care in medicine (10–12). For the patient with a low-risk perfusion scan, no additional testing is warranted because of the projected benign course (7,8). However, these data have been restricted to those patients undergoing 201Tl and 99mTc-sestamibi SPECT. For purposes of risk assessment, low risk is defined as a mortality rate of <1%/y (1), as based on published guidelines of care by the American College of Cardiology and the American Heart Association for stable chest pain patients (15,16). Using the results of this study, patients with a normal 99mTc-tetrofosmin SPECT scan (summed stress score of <4) are also at low risk of cardiac death (i.e., ∼0.6%/y), and, in the absence of refractory symptoms, these patients would be candidates for aggressive risk factor modification, using primary and secondary prevention guidelines (15,16).
Previous research on the clinical usefulness of 99mTc-tetrofosmin SPECT has reported differences in the detection of ischemia (17). In a recent report on 81 patients undergoing 99mTc-sestamibi and tetrofosmin vasodilator stress SPECT, the detection of reversible perfusion defects was reduced for tetrofosmin for those patients with mild-to-moderate coronary disease (17). The report by Soman et al. (17) hypothesized that the known reduced extraction fraction of 99mTc-testrofosmin may cause a reduced ability to detect coronary artery disease. A recent editorial noted that there is ample evidence suggesting that differences in radiopharmaceutical extraction do not appear critical to the application of risk stratification, but it may be limited to the subset of patients with prognostically benign coronary disease (14). Furthermore, precise biologic differences often do not translate into marked differences in patient outcome. Despite the differences noted in the prior 81 patient series, our report provides key details as to the excellent prognosis associated with a low-risk 99mTc-tetrofosmin scan.
Regarding the prognostic value of 99mTc-tetrofosmin SPECT, 3 prior reports with small patient series (n = 459, n = 246, and n = 597) have demonstrated that risk stratification is effective (10–12). Our data are consistent with these series and provide similar findings in a much larger number of patients. The inclusion of a greater number of patients from multiple centers allows for a greater generalizability and precision of findings compared with prior series. Our results reveal that the annualized major adverse cardiac event rate was 0.6% (95% CI = 0.4%–0.9%) for those patients with suspected or known coronary disease undergoing stress 99mTc-tetrofosmin SPECT.
These results were consistently applied through a variety of patient subsets including women and men as well as various age subsets. With exception, for those patients of >70 y old, because of increased comorbidity, the annualized rate for cardiac death increases to 1.6%–2.0% for those 80–100 y old. These results are consistent with prior series revealing that the elderly are at higher risk with an increased underlying disease and event burden that may preclude identification of those at very low risk (i.e., <1% annualized event rate) (18).
Several prior multicenter series and large observational studies have compared prognosis with other radionuclide isotopes (Fig. 4) (7,8). We performed several analyses to elucidate differences in larger consecutive patient series undergoing stress 201Tl, 99mTc-sestamibi, and 99mTc-tetrofosmin SPECT. Consistent with the published literature, our initial comparison with the published literature revealed that in >25,000 patients with an intermediate Duke treadmill score or stable chest pain symptoms, the annual cardiac survival rate ranged from 99.5% to 99.6%, similar to the cardiac mortality noted in our study using 99mTc-tetrofosmin.
Additional institutional databases were queried using a consecutive series of patients undergoing stress 201Tl and 99mTc-sestamibi SPECT (Fig. 3) (7). Our results revealed that in a risk-adjusted model (controlling for age, sex, and type of stress), 2.5- to 3.0-y survival was similar for the 2,423 and 3,257 patients undergoing 99mTc-sestamibi and 201Tl myocardial perfusion SPECT.
In the era of cost containment, it becomes increasingly important to determine whether noninvasive test results can be both clinically effective and cost-effective. We have shown previously that patients with normal SPECT scans require a watchful waiting approach to care. This type of management strategy results in cost efficiency and substantial cost savings compared with a more aggressive, invasive diagnostic workup strategy that includes diagnostic cardiac catheterization (19–21). From a prior series of 11,249 consecutive stable angina patients, gathered in a large multicenter trial comprising many laboratories around the United States, initial testing was performed with myocardial perfusion SPECT followed by selective catheterization in patients with provocative ischemia (19). These results reveal that there was a substantial reduction in costs using the myocardial perfusion SPECT plus selective catheterization approach (19–21). This series would extend the results to the population of patients undergoing stress 99mTc-tetrofosmin SPECT.
CONCLUSION
For those patients undergoing stress SPECT, a low-risk 99mTc tetrofosmin scan is associated with annualized cardiac death rates of 0.6%. These results are consistent with prior large registries or meta-analysis using 201Tl or 99mTc-sestamibi. Results from this large multicenter registry provide further supportive evidence that the excellent prognosis associated with a normal SPECT scan is isotope independent.
Acknowledgments
The authors thank Lesley Wood, MA, for her editorial contribution. Grant support was received from Amersham Health.
Footnotes
Received May 6, 2002; revision accepted Sep. 20, 2002.
For correspondence or reprints contact: Leslee J. Shaw, PhD, Atlanta Cardiovascular Research Institute, Suite 225, 5665 Peachtree Dunwoody Rd., Atlanta, GA 30342.
E-mail: lshaw{at}acrionline.org
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- 5-Year Prognostic Value of Quantitative Versus Visual MPI in Subtle Perfusion Defects: Results From REFINE SPECT
- Impact of Appropriate Use on the Prognostic Value of Single-Photon Emission Computed Tomography Myocardial Perfusion Imaging
- Prognostic Value of Stress Cardiac Magnetic Resonance Imaging in Patients With Known or Suspected Coronary Artery Disease: A Systematic Review and Meta-Analysis
- 2012 ACCF/AHA Focused Update Incorporated Into the ACCF/AHA 2007 Guidelines for the Management of Patients With Unstable Angina/Non-ST-Elevation Myocardial Infarction: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines
- 2012 ACCF/AHA Focused Update Incorporated Into the ACCF/AHA 2007 Guidelines for the Management of Patients With Unstable Angina/Non-ST-Elevation Myocardial Infarction: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines
- 2012 ACCF/AHA/ACP/AATS/PCNA/SCAI/STS Guideline for the Diagnosis and Management of Patients With Stable Ischemic Heart Disease: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, and the American College of Physicians, American Association for Thoracic Surgery, Preventive Cardiovascular Nurses Association, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons
- 2012 ACCF/AHA/ACP/AATS/PCNA/SCAI/STS Guideline for the Diagnosis and Management of Patients With Stable Ischemic Heart Disease: Executive Summary: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, and the American College of Physicians, American Association for Thoracic Surgery, Preventive Cardiovascular Nurses Association, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons
- 2012 ACCF/AHA/ACP/AATS/PCNA/SCAI/STS Guideline for the Diagnosis and Management of Patients With Stable Ischemic Heart Disease: Executive Summary: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, and the American College of Physicians, American Association for Thoracic Surgery, Preventive Cardiovascular Nurses Association, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons
- 2012 ACCF/AHA/ACP/AATS/PCNA/SCAI/STS Guideline for the Diagnosis and Management of Patients With Stable Ischemic Heart Disease: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, and the American College of Physicians, American Association for Thoracic Surgery, Preventive Cardiovascular Nurses Association, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons
- 2011 ACCF/AHA Focused Update Incorporated Into the ACC/AHA 2007 Guidelines for the Management of Patients With Unstable Angina/Non-ST-Elevation Myocardial Infarction: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines
- 2011 ACCF/AHA Focused Update Incorporated Into the ACC/AHA 2007 Guidelines for the Management of Patients With Unstable Angina/Non-ST-Elevation Myocardial Infarction: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines
- Improved Near-Term Coronary Artery Disease Risk Classification With Gated Stress Myocardial Perfusion SPECT
- ACC/AHA 2007 Guidelines for the Management of Patients With Unstable Angina/Non-ST-Elevation Myocardial Infarction: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines for the Management of Patients With Unstable Angina/Non-ST-Elevation Myocardial Infarction) Developed in Collaboration with the American College of Emergency Physicians, the Society for Cardiovascular Angiography and Interventions, and the Society of Thoracic Surgeons Endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation and the Society for Academic Emergency Medicine
- ACC/AHA 2007 Guidelines for the Management of Patients With Unstable Angina/Non-ST-Elevation Myocardial Infarction--Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines for the Management of Patients With Unstable Angina/Non-ST-Elevation Myocardial Infarction) Developed in Collaboration with the American College of Emergency Physicians, the Society for Cardiovascular Angiography and Interventions, and the Society of Thoracic SurgeonsEndorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation and the Society for Academic Emergency Medicine
- The Prognostic Value of Normal Exercise Myocardial Perfusion Imaging and Exercise Echocardiography: A Meta-Analysis
- Prognostic Stratification of Obese Patients by Stress 99mTc-Tetrofosmin Myocardial Perfusion Imaging
- The Value of Estimated Functional Capacity in Estimating Outcome: Results From the NHBLI-Sponsored Womens Ischemia Syndrome Evaluation (WISE) Study
- Risk Stratification of Patients with Angina Pectoris by Stress 99mTc-Tetrofosmin Myocardial Perfusion Imaging
- Ethnic Differences in the Prognostic Value of Stress Technetium-99m Tetrofosmin Gated Single-Photon Emission Computed Tomography Myocardial Perfusion Imaging
- Prognostic Value of Automated Quantification of 99mTc-Sestamibi Myocardial Perfusion Imaging
- The year in cardiac imaging