


Abstract
The estrogen receptor α (ERα) is expressed in approximately 70% of ovarian cancer tumors. PET of tumor ERα expression with the tracer 16α-18F-fluoro-17β-estradiol (18F-FES) may be valuable to select ovarian cancer patients for endocrine therapy. The aim of this study was to evaluate the feasibility of 18F-FES PET to determine tumor ERα expression noninvasively in epithelial ovarian cancer patients. Methods: 18F-FES PET/CT was performed shortly before cytoreductive surgery. Tumor 18F-FES uptake was quantified for all lesions 10 mm or greater on CT and expressed as maximum standardized uptake value. 18F-FES PET/CT findings were compared with histology and immunohistochemistry for ERα, ERβ, and progesterone receptor. Receptor expression was scored semiquantitatively using H-scores (percentage of positive tumor cells × staining intensity). The optimum threshold to discriminate ER-positive and -negative lesions was determined by receiver-operating-characteristic analysis. Results: In the 15 included patients with suspected ovarian cancer, 32 measurable lesions greater than 10 mm were present on CT. Tumor 18F-FES uptake could be quantified for 28 lesions (88%), and 4 lesions were visible but nonquantifiable because of high uptake in adjacent tissue. During surgery, histology was obtained of 23 of 28 quantified lesions (82%). Quantitative 18F-FES uptake correlated with the semiquantitative immunoscore for ERα (ρ = 0.65, P < 0.01) and weakly with progesterone receptor expression (ρ = 0.46, P = 0.03) and was not associated with ERβ expression (ρ = 0.21, P = 0.33). The optimum threshold to discriminate ERα-positive and ERα-negative lesions was a maximum standardized uptake value greater than 1.8, which provided a 79% sensitivity, 100% specificity, and area under the curve of 0.86 (95% confidence interval, 0.70–1.00). In 2 of 7 patients with cytology/histology available at primary diagnosis and at debulking surgery, immunohistochemical ERα expression had changed over time. 18F-FES PET was in accordance with histology at debulking surgery but not at primary diagnosis, indicating that 18F-FES PET could provide reliable information about current tumor ERα status. Conclusion: 18F-FES PET/CT can reliably assess ERα status in epithelial ovarian cancer tumors and metastases noninvasively. Evaluation of the predictive value of 18F-FES PET/CT for endocrine therapy in epithelial ovarian cancer patients is warranted.
Epithelial ovarian cancer is the second most common and most lethal gynecologic malignancy. Therefore, new therapeutic strategies are urgently needed. The estrogen receptor α (ERα) is expressed in approximately 70% of the epithelial ovarian cancer patients and presents a potential drug target for these tumors (1). Other hormone receptors, such as ERβ and progesterone receptor (PR), are expressed in approximately 75% and 20% of the patients, respectively (2). In phase II studies in ovarian cancer patients unselected for ERα expression, endocrine therapy generated objective responses in up to 19% and clinical benefit in up to 51% of the patients (3–7).
Given the relatively low response rate, predictive biomarkers would be valuable to select those patients who are most likely to benefit from endocrine therapy. In breast cancer, the ERα is a good predictor for response to endocrine agents (8). It therefore seems reasonable to select also ovarian cancer patients for endocrine therapy based on tumor ERα expression. Surprisingly, however, it is currently unknown whether tumor ERα expression is predictive for treatment response in ovarian cancer. In breast cancer patients, the ERα can be heterogeneously expressed among lesions within individuals, and ERα expression can change during the course of disease (9,10). In a retrospective study, ERα expression was discordant in 32% of 67 ovarian cancer patients with histology from both the primary tumor and a synchronous omental metastasis (2). A noninvasive method to quantify ERα expression in multiple metastases and at different time points might therefore be a valuable asset.
Whole-body imaging of tumor ERα expression could provide such information. It can be performed by PET with the tracer 16α-18F-fluoro-17β-estradiol (18F-FES) (11). 18F-FES PET can predict response to endocrine therapy in breast cancer and support patient-tailored therapy (12,13). It is, however, unknown whether 18F-FES PET can also be used to evaluate ERα expression in ovarian cancer tumors and whether 18F-FES PET can predict response to endocrine therapy in ovarian cancer patients. Visualization and quantification of 18F-FES uptake in ovarian cancer lesions may be impaired by the high physiologic uptake in the liver, gut, uterus, and bladder. We therefore evaluated the feasibility of 18F-FES PET/CT to accurately determine ER density in lesions of patients with epithelial ovarian cancer.
MATERIALS AND METHODS
Patients
Patients diagnosed or with high clinical suspicion of epithelial ovarian cancer were eligible when they had tumor lesions 10 mm or greater on diagnostic CT. Additional eligibility criteria were an Eastern Cooperative Oncology Group performance score of 2 or less and a postmenopausal status. Patients with a history of ER-positive malignancy (breast cancer, endometrial cancer) and patients using antiestrogenic drugs were excluded. All patients underwent 18F-FES PET/CT. Tumor tissue for histology was prospectively collected during surgery performed shortly after 18F-FES PET/CT imaging. Patients were allowed to have received neoadjuvant chemotherapy consisting of carboplatin/paclitaxel before 18F-FES PET/CT imaging. In these patients, 18F-FES PET/CT was performed after the last cycle of neoadjuvant chemotherapy and just before surgery. The Committee on Ethics of the University of Groningen approved this study, and all subjects signed a written informed consent form. The study is registered in the ClinicalTrials.gov database (NCT01439490).
CT and 18F-FES PET/CT Imaging
All patients underwent diagnostic CT to identify tumor lesions. 18F-FES was produced as previously described (14). Patients received approximately 200 MBq of 18F-FES intravenously. Whole-body 18F-FES PET/CT was performed 60 min after tracer injection, using a Biograph 64-slice mCT (PET/CT) camera (Siemens CTI) with 2-mm reconstructed spatial resolution and an emission acquisition time of 3 min per bed position. Low-dose CT (for attenuation and scatter correction) and PET imaging were performed sequentially within 1 procedure. Patients for whom the diagnostic CT scan was 6 wk or older at the moment of the 18F-FES PET/CT also underwent a new diagnostic CT scan in the same procedure. CT scans were evaluated by an experienced radiologist and used to allocate tumor lesions of 10 mm or greater. This threshold was chosen to limit partial-volume effects and resolution limitations during quantification of 18F-FES uptake. Tumor 18F-FES uptake was quantified by a nuclear medicine physician experienced in 18F-FES PET imaging and according to the European Association of Nuclear Medicine guidelines for tumor lesions of 10 mm or greater, using fused PET/CT images (15). In line with previous studies, we used the maximum standardized uptake value (SUVmax) to calculate tumor 18F-FES uptake (12,13). As an explorative analysis, we also measured the mean SUV (SUVmean) using a 70% isocontour of the hottest pixel (16). Concurrent with 18F-FES PET/CT, venous blood was collected from the infusion site (before 18F-FES injection) to evaluate serum estradiol and sex hormone–binding globulin, because these have been reported to negatively affect tumor 18F-FES uptake in breast cancer studies (11,17).
Tumor Histology
All patients were scheduled for cytoreductive surgery aimed at complete debulking of all macroscopic tumor lesions. The locations of resected tumor lesions were recorded to allow comparison between pathology and imaging results. All tumor lesions and macroscopic diameters at pathologic examination were listed in a database. Slides for histologic examination were prepared from all parts with suspected tumor. Hematoxylin and eosin staining was used to evaluate the presence of tumor cells in the resected tissue, and tumors were typed and graded. For all tumor lesions 10 mm or greater for which quantitative 18F-FES uptake was available, additional immunohistochemistry was performed. Paraffin-embedded formalin-fixed tumor blocks were sliced and mounted on 3-aminopropyltriethoxylane–coated glass slides. Immunohistochemistry was performed as previously described. Briefly, ERα was stained using the clinical-grade SP1 monoclonal rabbit anti-ERα antibody (Ventana) and PR using 1E2 monoclonal rabbit anti–PR antibody (Ventana) in the automated slide stainer with an iView DAB Detection kit (Ventana). ERβ was stained using a monoclonal mouse anti-ERβ1 clone PPG5/10 (Serotec).
Immunohistochemical Analysis
Two independent observers scored the slides for percentage of positive cells (0%–100%) and staining intensity (0, none; 1, weak; 2, moderate; and 3, strong) (18,19). For dichotomous classification of receptor positivity, 10% or more of tumor cells with moderate or strong staining was used as cutoff point in reference to other studies in ovarian cancer (20). For semiquantitative analysis, the percentage of positive cells and staining intensity scores were multiplied to obtain the H-score (range, 0–300) (21). To allow correction for tumor cell density, the percentage tumor and stromal tissue were estimated in a 1 cm2 field of view. Dichotomous immunohistochemistry results, H-scores, and ER density were compared with dichotomous and quantitative tumor 18F-FES uptake. Additionally, the association among serum CA-125, estradiol, and sex hormone–binding globulin with tumor 18F-FES uptake was evaluated.
Statistical Analysis
In this pilot study, we aimed to enroll approximately 15 patients to ensure the inclusion of at least 8 patients with ERα-positive histology. A sensitivity of 18F-FES PET/CT of 85% or more was anticipated. A stopping-rule was therefore applied when 4 or more of 8 patients with ER-positive histology did not show tumor 18F-FES uptake (SUVmax < 1.5), because this results in a 95% confidence interval below 85% sensitivity. Receiver-operating-characteristic analysis was performed to identify the optimum threshold to differentiate between ERα-positive and ERα-negative lesions. Sensitivity, specificity, and 95% confidence intervals were calculated. The Mann–Whitney U test was performed to evaluate differences in 18F-FES uptake between receptor (ERα, ERβ, PR)-positive and -negative tumors. A Spearman correlation coefficient was determined to evaluate the correlation between quantitative tumor 18F-FES uptake and semiquantitative measures of receptor expression and the correlation with serum estradiol and sex hormone–binding globulin.
RESULTS
Patient Characteristics
Fifteen patients were included between October 2011 and October 2013. One patient had a carcinosarcoma at pathologic examination and was therefore excluded from further analyses. Of the remaining 14 patients, 13 had serous carcinoma and 1 carcinoma of the transitional cell type. Patients had International Federation of Gynecology and Obstetrics stage III (n = 11), IV (n = 2), and recurrent ovarian cancer (n = 1). Nine (64%) of the 14 patients received 3 cycles of neoadjuvant chemotherapy before 18F-FES PET/CT imaging. 18F-FES PET/CT imaging was performed at a median of 9 d before cytoreductive surgery (range, 1–22 d). All patients had postmenopausal serum estradiol levels at the time of 18F-FES PET/CT (median, 0.04 nmol/L; range, 0.02–0.06 nmol/L) in accordance with the inclusion criteria. Serum CA-125 levels varied greatly at the time of 18F-FES PET/CT (median, 138 kU/L; range, 18–1,771 kU/L). Patient characteristics are shown in Table 1.
Patient Characteristics (n = 14)
18F-FES PET/CT Findings
All patients had a diagnostic contrast-enhanced CT scan available. All patients underwent 18F-FES PET with coregistration of a low-dose CT. Of the 14 patients, 2 patients underwent a new diagnostic CT at the time of 18F-FES PET/CT imaging; the remaining 12 patients had a diagnostic CT scan available that was made less than 6 wk (median, 28 d; range, 7–41 d) before 18F-FES PET/CT imaging.
On 18F-FES PET/CT, 12 of 14 patients had lesions with 18F-FES uptake. Thirty-two lesions of 10 mm or greater were identified on 18F-FES PET/CT. Four additional lesions were larger than 10 mm on earlier diagnostic CT but could not be identified on the low-dose CT at the time of 18F-FES PET/CT imaging. These 4 lesions were, however, present in patients who had received 3 cycles of neoadjuvant chemotherapy at the time of 18F-FES PET/CT, and all 4 lesions were confirmed to have become less than 10 mm due to neoadjuvant chemotherapy at pathologic examination. Finally, 4 lesions were visible on 18F-FES PET/CT, but 18F-FES uptake could not be reliably quantified because of high physiologic background uptake near the lesion (e.g., in the liver, uterus, and intestines). Therefore, 28 lesions, consisting of 12 ovarian tumors and 16 intraabdominal metastases, were used for 18F-FES PET/CT analysis. Examples of positive 18F-FES PET/CT images of abdominal metastases are provided in Figure 1. There were no new lesions discovered on 18F-FES PET/CT that had not yet been recorded on diagnostic CT. One patient had a newly diagnosed pleural effusion, which harbored increased 18F-FES uptake. Mean tumor SUVmax of all quantified lesions was 2.4 (range, 1.1–5.1). It was noted that 18F-FES uptake was absent in cystic parts of the tumor lesions (Fig. 2). Although not a primary aim of our study, it was noted that fusion of PET with the diagnostic CT was crucial for identification of the tumor lesions, because tissue surrounding the lesions, such as the uterus, bladder, and intestines, harbored high physiologic uptake.

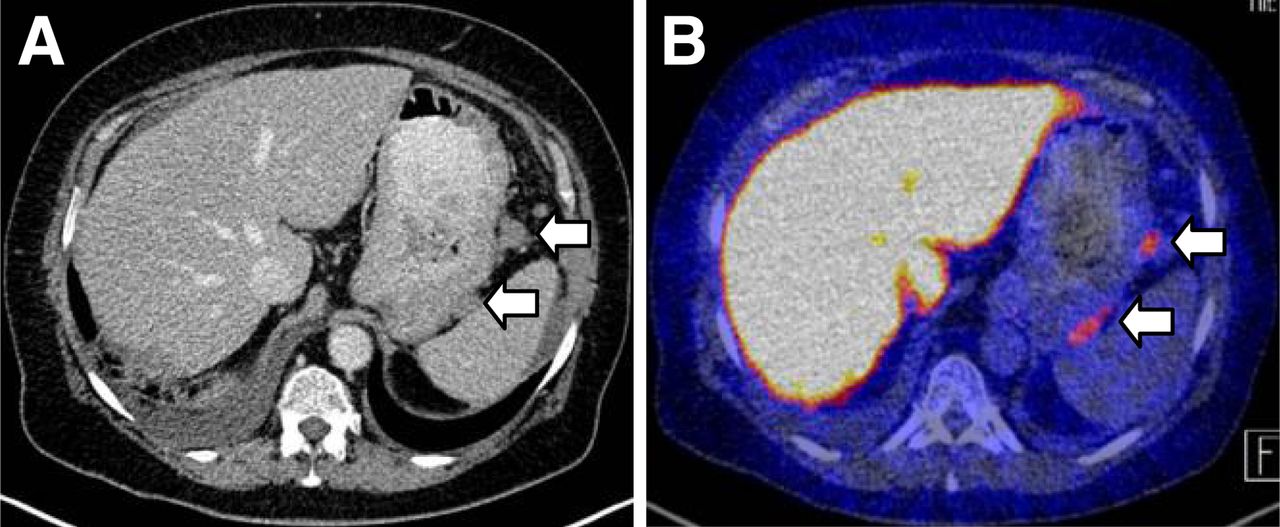
Imaging of patient with metastatic lesions between stomach and spleen (arrows): CT scan (A) and 18F-FES PET/CT (B).

CT (A) and 18F-FES PET/CT (B) findings of same patient as shown in Figure 3. ERα expression was high and tumor 18F-FES uptake (SUVmax) was 5.1. 18F-FES uptake was absent in cystic parts of tumor lesion (arrowhead) when compared with solid parts (arrow).
Concordance Between 18F-FES PET/CT and Pathology
Concurrent histology was available for 23 (82%) of 28 lesions quantified on 18F-FES PET/CT. Histology was not available for the remaining lesions because of inability to perform a complete debulking during surgery. ERα was positive in 19 of 23 lesions (83%), with a median H-score of 101 (range, 0–300); ERβ was positive in 13 lesions (57%), with a median H-score of 84 (range, 0–300); and PR was positive in 10 lesions (43%), with a median H-score of 65 (range, 0–188). Examples of ERα, ERβ, and PR immunostaining are provided in Figure 3.
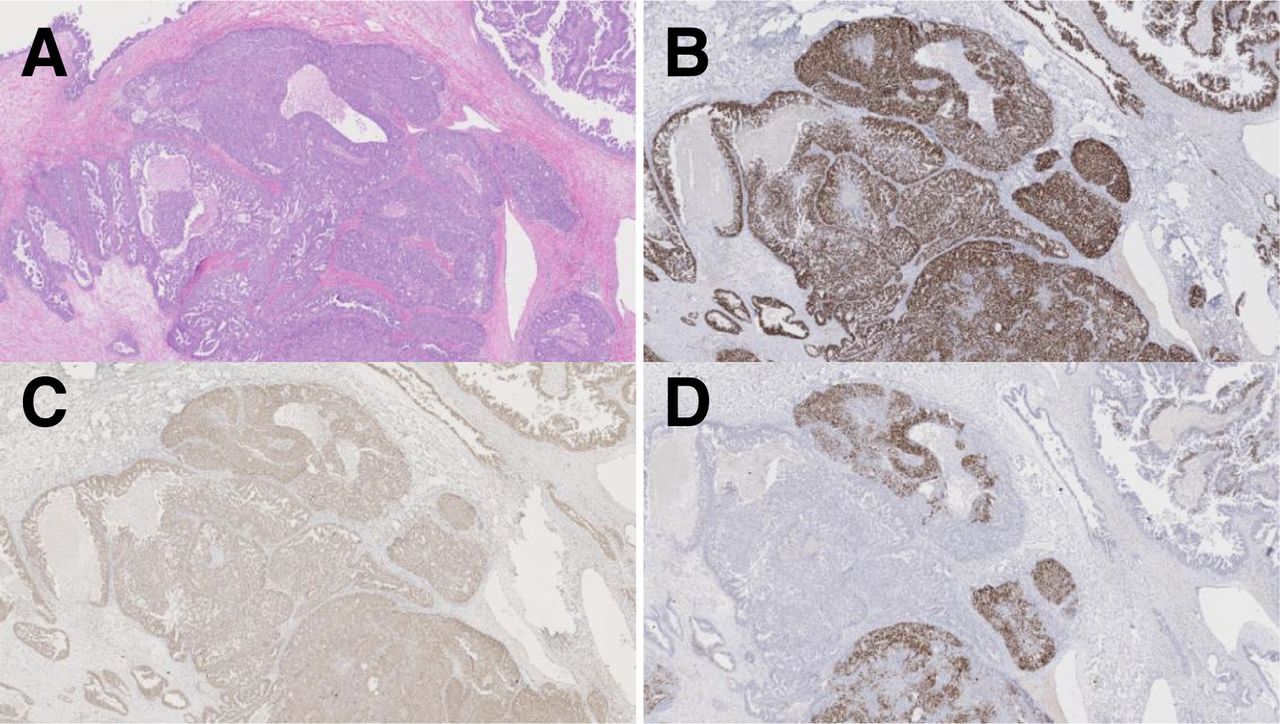
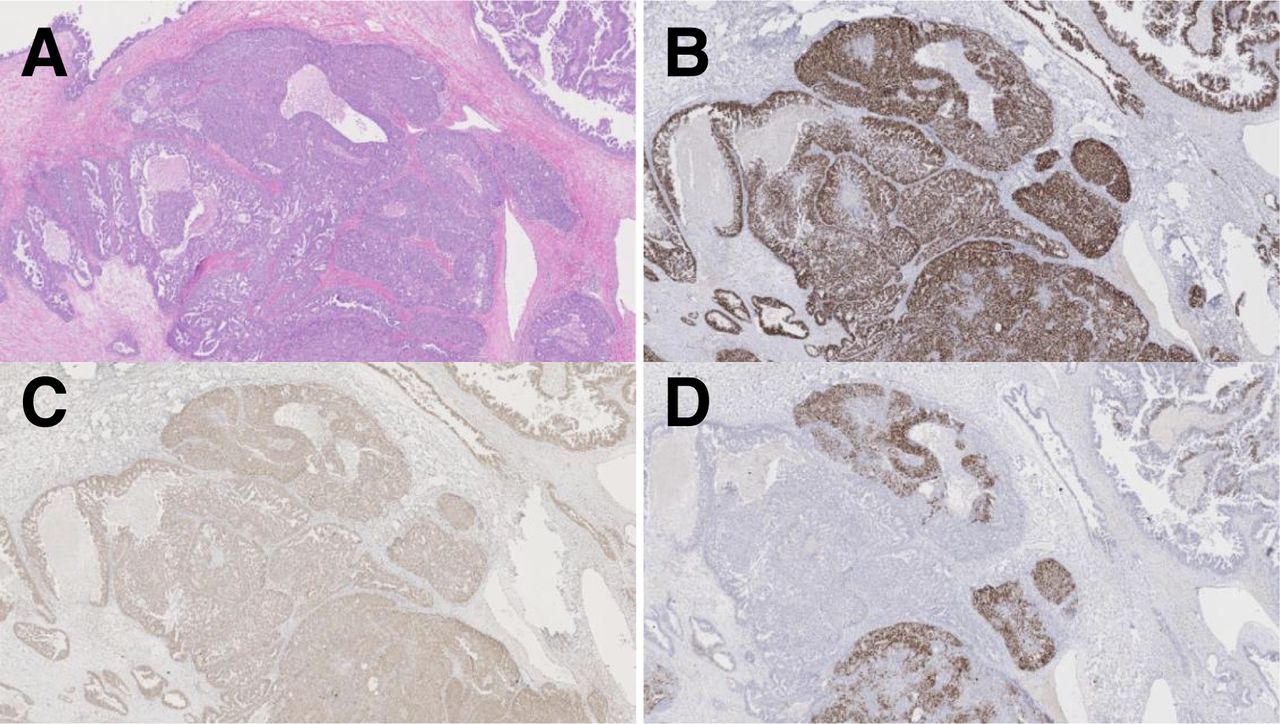
Representative examples of hematoxylin and eosin (A), ERα (B), ERβ (C), and PR (D) staining. In this patient, ERα expression was high, ERβ was moderately expressed, and PR was heterogeneously expressed.
Tumor 18F-FES uptake was higher in ERα-positive lesions than in ERα-negative lesions (SUVmax, 2.8 ± 1.3 vs. 1.4 ± 0.3, P = 0.03). The optimum threshold for quantitative 18F-FES PET imaging to discriminate between ERα-positive and ERα-negative lesions, as determined by receiver-operating-characteristic analysis, was an SUVmax of 1.8. Application of this threshold resulted in a 100% specificity (4/4 lesions with uptake < 1.8 were ERα-negative) and 79% sensitivity (15/19 lesions with uptake > 1.8 were ERα-positive). Also, when this threshold was used, 1 patient had both 18F-FES-positive and 18F-FES-negative lesions.
Mean tumor 18F-FES uptake did not differ significantly between ERβ-positive and ERβ-negative lesions (SUVmax, 2.9 ± 1.4 vs. 2.1 ± 1.0, P = 0.19) and between PR-positive and PR-negative lesions (SUVmax, 3.1 ± 1.5 vs. 2.1 ± 0.8, P = 0.17). As expected, 18F-FES PET/CT was not suitable to differentiate between ERβ-positive and ERβ-negative lesions, with a calculated sensitivity of 77% and specificity of 50%. The calculated sensitivity and specificity of 18F-FES PET/CT for PR-positive lesions were 70% and 38%, respectively. The use of SUVmean instead of SUVmax did not affect the sensitivity and specificity of 18F-FES PET for ERα-positive lesions, with an SUVmean of 1.3 or greater as the optimum threshold to discriminate between ERα-positive and ERα-negative lesions.
In 7 patients with histology at primary diagnosis, and at debulking surgery after neoadjuvant chemotherapy, paired samples were available to evaluate temporal discordance in ERα expression. In 2 patients (29%), there was discordant ERα expression. Both patients had ERα-negative immunohistochemistry at diagnosis, 18F-FES PET/CT showed 18F-FES–positive lesions, and subsequent histology obtained during debulking surgery shortly thereafter was ERα-positive.
Correlation Between Quantitative 18F-FES PET/CT and Receptor Expression
Quantitative tumor 18F-FES uptake (SUVmax) correlated well with the H-score for ERα (ρ = 0.65, P < 0.01, Fig. 4A). 18F-FES uptake showed a weak correlation with PR expression (ρ = 0.46, P = 0.03, Fig. 4B) and was not associated with ERβ expression (ρ = 0.21, P = 0.33, Fig. 4C). The weak correlation observed between 18F-FES uptake and PR expression can likely be explained by the fact that increased ERα expression correlated with increased PR expression (ρ = 0.54, P < 0.01) because PR is an ERα-mediated estrogen-responsive gene. Indeed, median SUVmax was 3.8 in PR-positive tumors that were also ERα-positive (n = 8 lesions) and only 1.2 in PR-positive tumors that were ERα-negative (n = 2 lesions).

Correlation between quantitative tumor 18F-FES uptake (SUVmax) and semiquantitative immunoscore (H-score) for tumor ERα expression (A), ERβ expression (B), and PR expression (C).
The use of SUVmean instead of SUVmax provided a slightly better correlation between quantitative tumor 18F-FES uptake and ERα expression (ρ = 0.75, P < 0.01). Also PR correlated with tumor SUVmean (ρ = 0.55, P < 0.01), whereas ERβ expression did not correlate with tumor 18F-FES uptake using SUVmean (ρ = 0.30, P < 0.01).
In 4 lesions of 2 patients treated with neoadjuvant chemotherapy, quantitative tumor 18F-FES uptake was low, whereas tumor cells were clearly ERα-positive. In these 2 patients, however, the tumors had a relatively low percentage of vital tumor cells. The lower ER density per cm2 therefore likely explains these false-negative findings (Fig. 5).
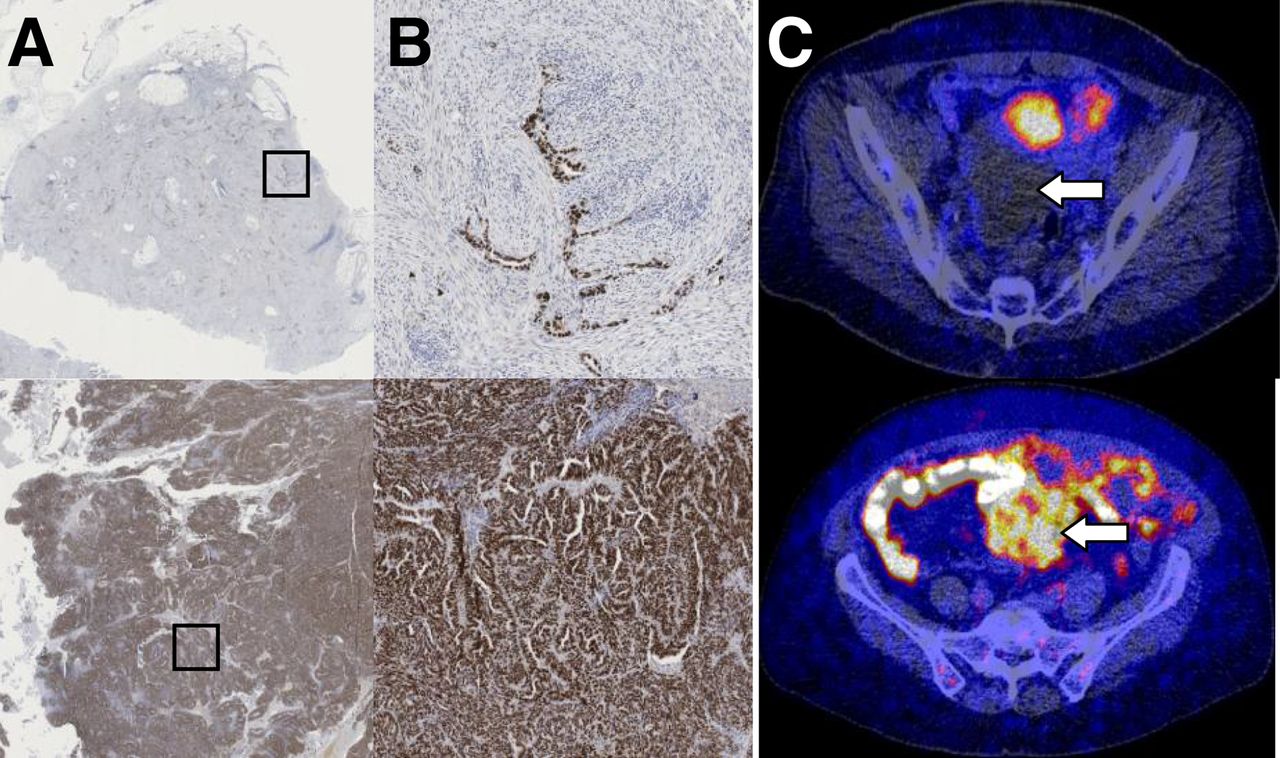
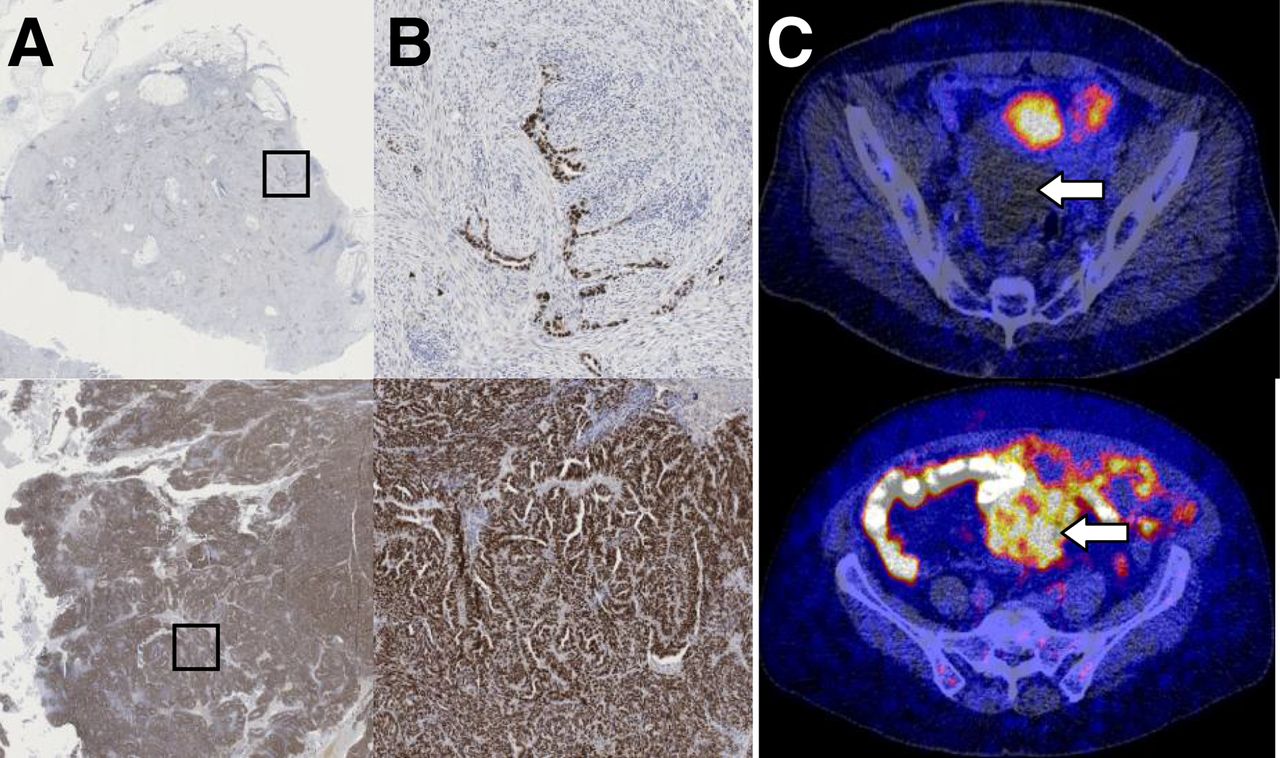
Example of patient with false-negative 18F-FES PET/CT findings (upper) and true-positive 18F-FES PET/CT findings (lower). (A) 1 cm2 overview of ERα staining. (B) 1 mm2 overview of ERα staining of indicated area in A. (C) Corresponding 18F-FES PET/CT findings. Arrows indicate tumor mass. 18F-FES uptake (SUVmax) was 1.3 in tumor shown in upper panel and 4.9 in lower panel. Low tumor cell density in upper panel likely explains negative findings on 18F-FES PET/CT.
Correlation Between Quantitative 18F-FES PET/CT and Serum Estradiol and Sex Hormone–Binding Globulin
All patients had postmenopausal serum estradiol levels. Within the postmenopausal range, there was no trend toward lower 18F-FES uptake in individuals with higher serum estradiol levels (ρ = 0.06, P = 0.56). Increased sex hormone–binding globulin levels were reported to negatively affect tumor 18F-FES uptake in larger breast cancer studies (17). In our study, high serum sex hormone–binding globulin levels did not correlate with lower tumor 18F-FES uptake (ρ = −0.18, P = 0.59).
DISCUSSION
This is the first study, to our knowledge, that showed that 18F-FES PET/CT can reliably assess tumor ERα status in patients with epithelial ovarian cancer. Twelve of 14 patients had tumor lesions with an increased 18F-FES uptake.
To the best of our knowledge, no earlier studies describing 18F-FES PET/CT in ovarian cancer are available, apart from 1 preliminary case report of 18F-FES PET in a patient with ovarian cancer and leiomyoma in a review article that indicated that 18F-FES uptake can be observed in ovarian cancer (22).
In our feasibility study, we learned several aspects that can be of relevance for future 18F-FES PET studies in ovarian cancer patients. First, we showed that 18F-FES uptake was absent in the cystic parts of lesions and therefore a sufficiently large (e.g., >10 mm) solid component is required for quantification of tumor 18F-FES uptake. Second, in contrast to breast cancer, for which 18F-FES–positive lesions can usually readily be observed also without a concurrent CT scan (23), in this study, ovarian cancer lesions had to be allocated using a concurrent or recent contrast-enhanced diagnostic CT scan. This limitation is because most lesions develop in the abdominal cavity, in which visualization is hampered by high physiologic background tracer levels in the liver, gallbladder, intestines, uterus, kidneys, and bladder (24). Finally, our study design allowed the inclusion of patients who had received neoadjuvant chemotherapy, which has potentially affected tumor 18F-FES uptake. The inclusion of neoadjuvant-treated patients with high-stage disease allowed us to obtain both 18F-FES PET/CT data and concurrent histology of multiple lesions from the same patient, which was also one of the strengths of our study. In 2 of 9 of neoadjuvant-treated patients, however, all lesions larger than 10 mm on earlier diagnostic CT scans were reduced in size to less than 10 mm due to chemotherapy effects precluding the assessment at the time of 18F-FES PET. In 2 other neoadjuvant-treated patients, 4 lesions greater than 10 mm harbored only a few vital tumor cells at pathologic examination. Thus, antitumor effects in patients treated with neoadjuvant chemotherapy may have affected 18F-FES PET sensitivity.
To date, most 18F-FES PET studies have used SUVmax to quantify tumor 18F-FES uptake (11). This method of quantification has several advantages, among which is its easy reproducibility. As an explorative analysis, we also measured SUVmean using an arbitrary 70% isocontour. Although this slightly increased the correlation between tumor 18F-FES uptake (SUVmean) and ERα expression, it did not result in a better sensitivity and specificity. The most optimum way to quantify tumor 18F-FES uptake, using SUVmax or SUVmean with a percentage isocontour, with or without correction for background physiologic 18F-FES uptake needs to be addressed in future studies.
The current gold standard to determine hormone receptor expression is immunohistochemistry. This standard has some limitations in patients with metastatic disease, including possible difficulty in obtaining a biopsy because of, for example, the location of the lesion. Also, determining the current ER status of the patient on stored tissue samples can be unreliable because of changes in ER expression over time. Finally, because of intratumor and intertumor heterogeneity, a biopsy may not always reflect actual ER status. These issues have especially been shown to play a role in breast cancer (9,10) but may also apply to ovarian cancer. Specifically, we showed previously that heterogeneous ER expression among lesions within the same individual does also exist in ovarian cancer (2). In the current study, in 2 of 7 patients with biopsies at diagnosis and at surgery several months later, discordant ERα expression was observed. Because the first biopsy was performed as a diagnostic procedure before inclusion in the study, we were unable to precisely determine which lesion was biopsied. Therefore, the discordance might be explained by heterogeneity between lesions or by changes in ER expression, for example, because of neoadjuvant chemotherapy effects. Either way, this difference illustrates that a single tumor biopsy may not always reliably reflect ERα status during the course of disease.
18F-FES PET has previously been evaluated to assess ER status in breast cancer metastases, which showed a good sensitivity of 84% and excellent specificity of 98% (11,25–28). In addition, 18F-FES PET was shown to be a predictive biomarker for response to antihormonal therapy in various studies in metastatic breast cancer patients (12,13,29). In ovarian cancer patients, the role of endocrine therapy is limited. Objective tumor responses to endocrine agents are observed in 8%–19% of heavily pretreated patients in several phase II studies (4,5,30–32). But surprisingly, these studies did not generally select patients based on ER expression by their tumor. In a retrospective study in 26 patients with ovarian cancer treated with the pure ER antagonist fulvestrant, higher levels of ER expression by the tumor were associated with clinical benefit (33).
CONCLUSION
18F-FES PET/CT can reliably assess ERα status in epithelial ovarian cancer tumors and metastases noninvasively, with a 79% sensitivity and 100% specificity. On the basis of the findings of this study, exploration of the value of 18F-FES PET to predict treatment response to endocrine agents is warranted. Ideally, patients with ovarian cancer presenting with especially solid tumor lesions larger than 10 mm seem candidates for evaluating the potential of 18F-FES PET/CT as a predictive imaging biomarker.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. This study was supported by a grant from the Dutch Cancer Society, RUG 2009-4529. No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Dec. 4, 2014.
- © 2015 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication August 21, 2014.
- Accepted for publication October 28, 2014.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Management challenges in low-grade serous ovarian cancer with a BRCA mutation
- Low-grade serous ovarian cancer: expert consensus report on the state of the science
- Synthesis and Evaluation of the Estrogen Receptor {beta}-Selective Radioligand 2-18F-Fluoro-6-(6-Hydroxynaphthalen-2-yl)Pyridin-3-ol: Comparison with 16{alpha}-18F-Fluoro-17{beta}-Estradiol
- 18F-Fluoroestradiol PET: Current Status and Potential Future Clinical Applications
- Molecular Imaging of Ovarian Cancer