


Abstract
Epigenetic modifiers, including the histone deacetylase inhibitor vorinostat, may sensitize tumors to chemotherapy and enhance outcomes. We conducted a multicenter randomized phase II neoadjuvant trial of carboplatin and nanoparticle albumin-bound paclitaxel (CP) with vorinostat or placebo in women with stage II/III, human epidermal growth factor receptor 2 (HER2)–negative breast cancer, in which we also examined whether change in maximum standardized uptake values corrected for lean body mass (SULmax) on 18F-FDG PET predicted pathologic complete response (pCR) in breast and axillary lymph nodes. Methods: Participants were randomly assigned to 12 wk of preoperative carboplatin (area under the curve of 2, weekly) and nab-paclitaxel (100 mg/m2 weekly) with vorinostat (400 mg orally daily, days 1–3 of every 7-d period) or placebo. All patients underwent 18F-FDG PET and research biopsy at baseline and on cycle 1 day 15. The primary endpoint was the pCR rate. Secondary objectives included correlation of change in tumor SULmax on 18F-FDG PET by cycle 1 day 15 with pCR and correlation of baseline and change in Ki-67 with pCR. Results: In an intent-to-treat analysis (n = 62), overall pCR was 27.4% (vorinostat, 25.8%; placebo, 29.0%). In a pooled analysis (n = 59), we observed a significant difference in median change in SULmax 15 d after initiating preoperative therapy between those achieving pCR versus not (percentage reduction, 63.0% vs. 32.9%; P = 0.003). Patients with 50% or greater reduction in SULmax were more likely to achieve pCR, which remained statistically significant in multivariable analysis including estrogen receptor status (odds ratio, 5.1; 95% confidence interval, 1.3–22.7; P = 0.023). Differences in baseline and change in Ki-67 were not significantly different between those achieving pCR versus not. Conclusion: Preoperative CP with vorinostat or placebo is associated with similar pCR rates. Early change in SULmax on 18F-FDG PET 15 d after the initiation of preoperative therapy has potential in predicting pCR in patients with HER2-negative breast cancer. Future studies will further test 18F-FDG PET as a potential treatment-selection biomarker.
Chemotherapy is currently the only standard neoadjuvant treatment for women with triple-negative (estrogen receptor [ER]–negative, progesterone receptor [PR]–negative, human epidermal growth factor receptor 2 [HER2]–negative) breast cancer and is also administered to women with the luminal B subtype before endocrine therapy. Many women experience recurrence and death despite this approach, emphasizing the need for new therapeutic strategies. Preclinical research supports the investigation of epigenetic modifiers such as the histone deacetylase inhibitor vorinostat for the treatment of breast cancer. In ER-positive and ER-negative breast cancer cell lines, vorinostat reduces proliferation, induces cell cycle arrest and modulates gene expression (1), and enhances the cytotoxicity of chemotherapy in in vitro models (2). Phase I investigation of the combination of vorinostat with carboplatin and paclitaxel was well tolerated and yielded a recommended phase II dose (3).
Prognostic and treatment-selection biomarkers for breast cancer patients, that could be determined at baseline or after a short duration of therapy, are also needed. Preoperative systemic therapy (PST) is an attractive model for the assessment of novel therapeutic agents and surrogate biomarkers of response (4). Pathologic complete response (pCR) after PST is an accepted primary endpoint in clinical trials, predicting improved disease-free and overall survival (5–7). Several biomarkers have been proposed that may predict pCR, including early changes in 18F-FDG uptake on PET (8); however, prospective studies establishing standardized methods and defining optimal cut points are needed to determine the clinical utility of this tool.
We hypothesized that the addition of vorinostat would improve the pCR rate observed with PST alone in women with stage II–III, grade 2–3, HER2-negative breast cancer. We also hypothesized that changes by cycle 1 day 15 (C1D15) of therapy in tumor standardized uptake values corrected for lean body mass (SULmax) on 18F-FDG PET, and the proliferation index Ki-67, would predict pCR. To test these hypotheses we performed a double-blind, randomized, placebo-controlled multicenter phase II study of 12 wk of preoperative carboplatin and nanoparticle albumin-bound (nab) paclitaxel (CP) with vorinostat or placebo, incorporating early tissue and 18F-FDG PET imaging biomarker evaluations (NCT00616967).
MATERIALS AND METHODS
Eligibility
Women 18 y or older, with histologically proven infiltrating carcinoma of the breast, were eligible if they presented with operable, clinical stage T1c, N1–3 or T2–4 lesions, any N, and M0. Tumors must have been HER2-negative and grade 2 or 3, with any ER or PR status. Eastern Cooperative Oncology Group performance status 0–1 and adequate organ function were required. Exclusion criteria were outlined in the clinical protocol. Women signed an informed consent form approved by the Institutional Review Boards of participating institutions.
Study Design
Before initiating the multicenter, double-blind, randomized phase II portion of the study, we conducted a nonrandomized, single-site open-label safety run-in phase. Participants received 12 wk of preoperative carboplatin (area under the curve of 2, weekly) and nab-paclitaxel (100 mg/m2 weekly) with vorinostat (400 mg orally daily, days 1–3 of every 7-d period). Statistical considerations were included in the research protocol.
Participants in the phase II portion of the study were randomly assigned 1:1 to receive CP with vorinostat or placebo using permuted block randomization, stratified by hormone receptor status (ER and PR < 1% vs. ER or PR ≥ 1%). Common Terminology Criteria for Adverse Events, version 3.0, was used to grade toxicity. Additional nonstudy chemotherapy (adriamycin and cyclophosphamide [AC], per guidelines) was allowed per treating physician discretion before definitive surgery, for patients with incomplete response or disease progression on study treatment. Tumor biopsy and blood sample were requested before nonstudy chemotherapy.
Prophylactic growth factor support and dose modifications for toxicity were suggested in the research protocol. Axillary evaluation before initiating study therapy and final surgery type were per treating surgeon discretion. Administration of postoperative radiation and systemic therapies were also per discretion of the treating team, with guidelines in the research protocol.
18F-FDG PET/CT
Participants underwent 18F-FDG PET/CT from midskull to midfemur level before tumor biopsy, as previously described, at baseline and C1D15 (9). Each site was asked to acquire and reconstruct a specific phantom study for central site review. That phantom was reviewed for a variety of quantitative features (e.g., uniformity and maximum and mean standardized uptake values [SUVs]) before the site was qualified for participation in the trial. Each site also submitted a whole-body 18F-FDG PET clinical study example for review by a physicist at the central site before site’s acceptance into the study. A uniform imaging protocol was provided to all users, which included dosing (8.14 MBq [0.22 mCi]/kg ± 20%), uptake (60 ± 10 min), and plasma glucose recording. Imaging was not performed if plasma glucose was greater than 200 mg/dL. The protocol was based on our own clinicians’ 18F-FDG PET/CT protocol with components drawn from published protocols as well as institutional experience (10).
Regions of interest were captured over the entire volume of disease tissue and primary tumor. SULmax was collected because it is more consistent in absolute value than SUV from patient to patient in normal tissues, being less weight-dependent (11). Imaging and quantitation were centrally reviewed.
Immunohistochemistry
A study-specific core biopsy was obtained at baseline, C1D15, before nonstudy preoperative chemotherapy if given, and at the time of definitive surgery. Tumor biopsy at baseline and C1D15 was performed preferably about 4 h after vorinostat dose and before carboplatin and nab-paclitaxel dose. Slides were stained for Ki-67 and ER using commercially available monoclonal antibodies (Ki-67 [Immunotech], ER [Leicabiosystems], clone 6f11) in a CLIA (Clinical Laboratory Improvement Amendment)-certified laboratory and centrally quantified by the study pathologist.
Statistical Considerations
The primary endpoint was pCR, defined as no viable invasive cancer in the breast and axilla. All other cases were defined as non-pCR. The pCR rate was determined in each arm separately by performing an intent-to-treat (ITT) analysis of all randomized patients. Patients with unknown pCR status were considered pathologic nonresponders. The computation of associated 90% confidence intervals did not account for the sequential design.
The study included a concurrent randomized control arm of CP plus placebo for the primary endpoint. The design required 31 women per arm to detect a 25% pCR rate from null response rate of 10% using a Simon 2-stage design with 80% power and 10% type I error rate. There was no intention to formally compare the two arms. A single interim analysis for futility was performed once 16 patients underwent surgery in each arm by the study statistician and an investigator independent of the study conduct, both masked to treatment. A preplanned masked interim analysis for toxicity was conducted in the first 24 patients.
Key secondary objectives were to correlate change in tumor SULmax on 18F-FDG PET by C1D15 with pCR and to correlate baseline and change in Ki-67 with pCR. Percentage reduction in SULmax treated as a continuous variable was compared between responders and nonresponders using the nonparametric Wilcoxon rank sum test and the Fisher exact test when dichotomized at a predefined threshold (≥50% reduction). A receiver-operating-characteristic curve analysis was performed to explore the best cutoff of SULmax reduction and its predictive accuracy for pCR. The association of baseline and change in SULmax or Ki-67 with pCR was evaluated using logistic regression models, with adjustment for hormone receptor status in multivariable analysis. Additional unplanned post hoc analyses, performed for both primary and secondary objectives, considered patients who received additional therapies before surgery as pathologic nonresponders.
Safety analysis included patients who received at least 1 dose of any study drug. All quantitative parameters were expressed as mean ± SD or median and range. All statistical tests were 2-sided and considered statistically significant at a P value of less than 0.05. The analyses were performed using SAS (version 9.2; SAS Institute) and R software packages (version 2.15.2). The research protocol and article were written by the authors and reviewed by the pharmaceutical funders, who had no access to the study database and were not involved in study analysis or interpretation of results.
RESULTS
Safety Run-in
Six patients were enrolled in the safety run-in phase. The combination was well tolerated, with predominantly grade 1 and 2 adverse events. The recommended phase II dose for CP was as described in the “Study Design” section, in combination with 400 mg of vorinostat or placebo.
Phase II
Patient Characteristics
From October 2009 to November 2011, 62 women enrolled in the study, with patient characteristics well balanced across treatment groups (Table 1). Of the 62 randomized, 61 completed study drugs and 60 completed primary surgery. Two patients with unknown pCR status were regarded as pathologic nonresponders on an ITT basis. Eighteen of 60 women (6 vorinostat arm, 12 placebo arm) also received preoperative nonstudy chemotherapy (anthracycline-based) because of incomplete clinical response or physician preference (including 8 women with clinical complete response) and were included in the ITT analysis (Fig. 1). Dose modifications are described in Supplemental Table 1 (supplemental materials are available at http://jnm.snmjournals.org). Thirty-three patients received AC, and 2 received cisplatin, postoperatively.
Patient Characteristics

CONSORT flow diagram for phase II. All 73 patients who signed consent for formal eligibility assessment are included.
Treatment Safety
Hematologic and nonhematologic toxicities are shown in Supplemental Table 2. There were no significant differences in adverse events between the arms. The preplanned masked interim toxicity analysis did not meet the criteria for early stopping.
Treatment Efficacy
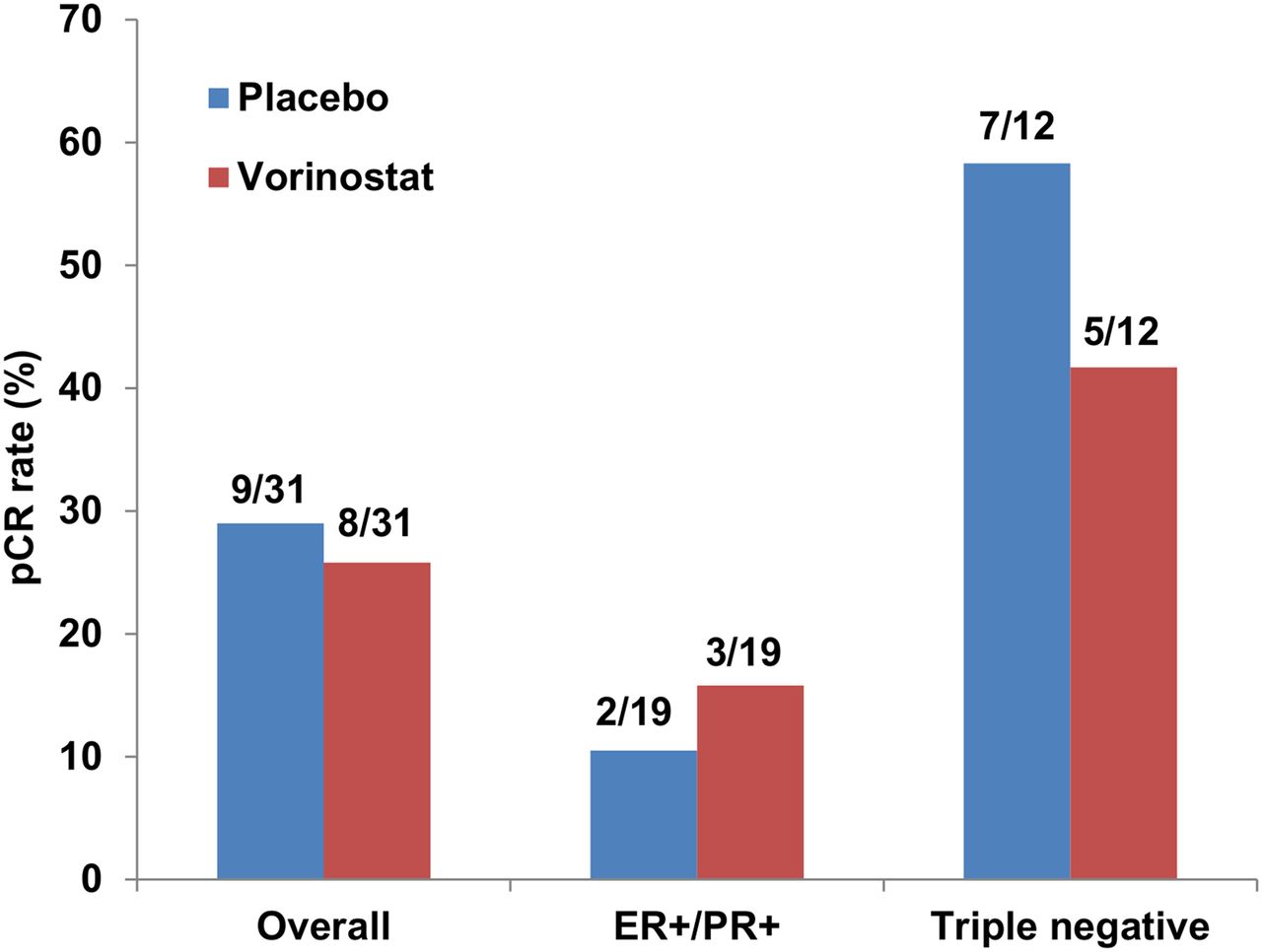
Overall, pCR was observed in 17 patients (27.4%; 95% confidence interval [CI], 16.9%–40.2%) in the ITT population, meeting the predefined aim of 25% in each arm: 8 in the vorinostat arm (25.8%; 95% CI, 11.9%–44.6%) and 9 in the placebo arm (29.0%; 95% CI, 14.2%–48.0%). Because the pCR rates in both arms were similar, we pooled the arms to obtain this overall pCR rate with a 95% CI. Of patients obtaining pCR, 12 were ER- and PR-negative, 5 were ER- or PR-positive (2 with known BRCA mutations, 1 in each arm, one of whom received preoperative nonstudy chemotherapy), and all were grade 3. When stratified by hormone receptor status, the pCR rate in the placebo arm was 10.5% (2/19; 95% CI, 1.3%–33.1%) and in the vorinostat arm 15.8% (3/19; 95% CI, 3.4%–39.6%) for patients with ER- or PR-positive disease. For patients with triple-negative breast cancer, the pCR rate was 58.3% (7/12; 95% CI, 27.6%–84.8%) in the placebo arm and 41.7% (5/12; 95% CI, 15.2%–72.3%) in the vorinostat arm (Fig. 2). Additionally, we performed an analysis considering patients who received additional nonstudy preoperative chemotherapy as pathologic nonresponders, to provide a conservative estimate for the pCR rate with study therapy alone. The overall pCR rate was 17.7% (11/62; 95% CI, 9.2%–29.5%), 16.1% for the vorinostat arm (5/31; 95% CI, 5.5%–33.7%), and 19.4% for placebo arm (6/31; 95% CI, 7.5%–37.5%).

pCR rates overall and by subgroup (ITT analysis).
Baseline and Change in Biomarkers and Correlation with Response to Therapy
All 62 patients underwent baseline study biopsy and 18F-FDG PET, and 59 (95.2%) and 61 (98.4%) underwent both baseline and C1D15 biopsy and 18F-FDG PET, respectively. Baseline 18F-FDG PET occurred within 30 d before the initiation of study therapy (75% within 1 wk of initiation of therapy, range 0–30), and C1D15 18F-FDG PET occurred on day 15 in 66% of cases (range, days 14–22). 18F-FDG PET was performed before study biopsy in all but 4 cases (baseline) and in all cases at C1D15. No significant differences in the biomarkers were found between treatment groups, and thus a pooled analysis was performed using data from patients with valid 18F-FDG PET data at baseline and C1D15. Change in SULmax was evaluated in 59 women (16 pCR, 43 no pCR), where 3 were not evaluable (technically invalid 18F-FDG PET data [n = 2] or no available C1D15 18F-FDG PET [n = 1]). Median baseline SULmax in pathologic responders was significantly higher than in pathologic nonresponders (7.6 vs. 5.3; P = 0.018; Table 2). A significant difference in change in SULmax was observed between pathologic responders and nonresponders (median percentage reduction, 63% vs. 33%; P = 0.003; Fig. 3; Table 2). Seventy-five percent of pathologic responders exhibited a 50% or greater reduction in SULmax at C1D15 versus 30% of nonresponders (P = 0.003; Table 2). Patients with a 50% or greater reduction in SULmax were more likely to achieve a pCR, as suggested by both univariate (odds ratio, 6.6; 95% CI, 1.9–27.3; P = 0.004) and multivariable analyses adjusting for hormone receptor status (odds ratio, 5.1; 95% CI, 1.3–22.7; P = 0.023; Table 3). By receiver-operating-characteristic analysis, discrimination between patients with pCR (pathologic responders) and no pCR (pathologic nonresponders) resulted in an area under the curve of 0.76 (95% CI, 0.60–0.91), with a sensitivity of 0.75 and specificity of 0.74 at a cutoff of 52% reduction in SULmax that maximized the sum of sensitivity and specificity. Negative predictive value and positive predictive value were 89% and 52%, respectively. A post hoc sensitivity analysis was performed excluding patients who received additional nonstudy preoperative therapy and demonstrated similar results (Supplemental Tables 3 and 4).
Baseline and Change in SULmax Between Pathologic Responders and Nonresponders
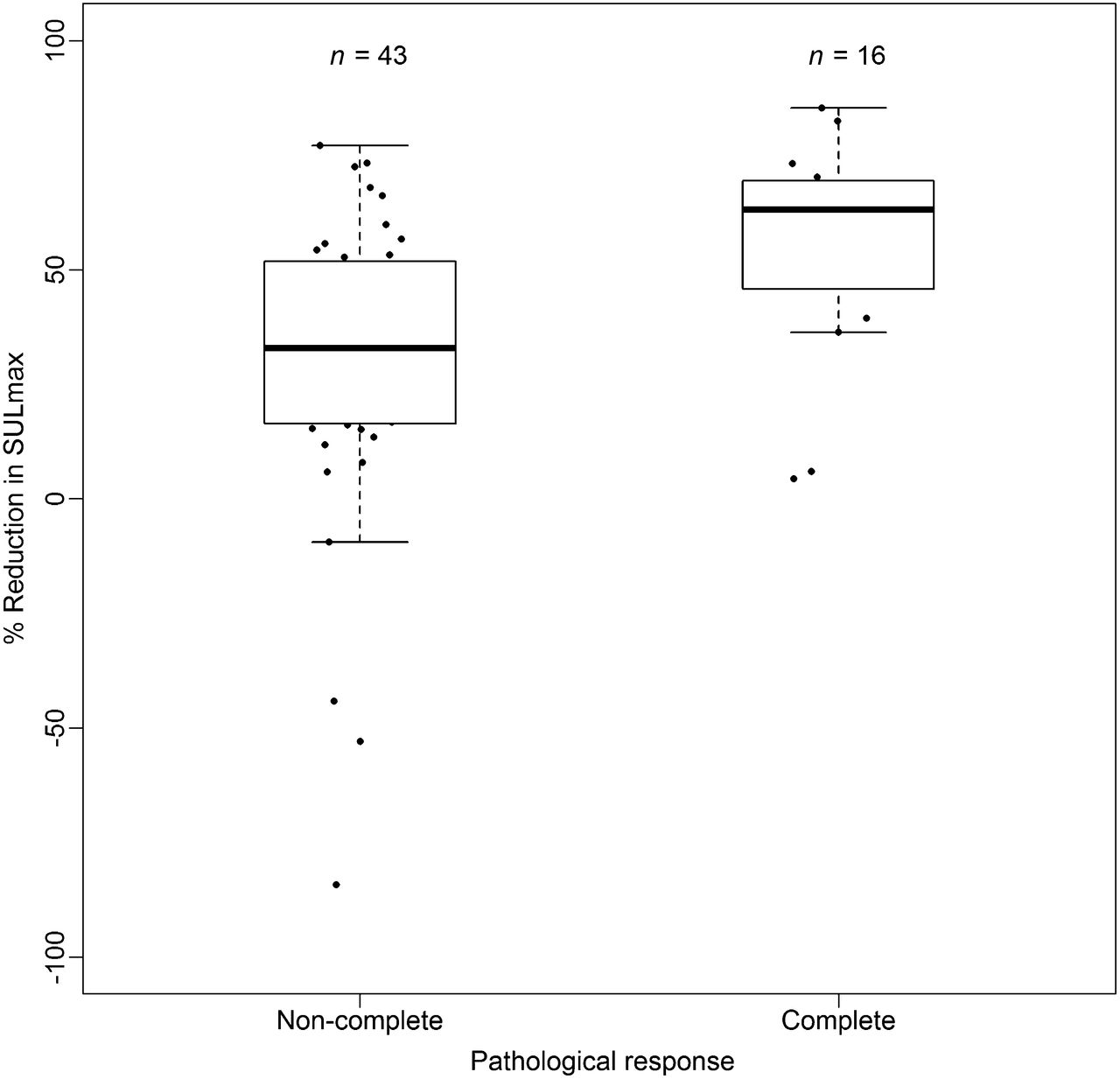
Box plots of reduction in SULmax in patients with pCR and non-pCR. Horizontal line inside box shows median. Lower and upper hinges of box represent 25th and 75th percentiles, respectively. ● = actual values of percentage reduction in SULmax.
Analysis of Association of SULmax with Pathologic Response
Forty-four matched specimens (baseline, C1D15) were evaluable for change in Ki-67 (8 pCR, 36 non-pCR); nonevaluable samples had no tumor cells present or Ki-67 unavailable at either or both time points. We did not observe statistically significant differences in baseline and C1D15 percentage change in Ki-67 between pathologic responders and nonresponders nor a significant change in ER status between before and after therapy (Supplemental Table 5).
DISCUSSION
We demonstrated that preoperative CP plus vorinostat or placebo was associated with similar pCR rates in women with HER2-negative breast cancer. The pCR rate observed overall in the ITT population (27%) was greater than initially predicted on the basis of historic data in unselected breast cancer subtypes (12). However, a proportion of patients received additional nonstudy preoperative chemotherapy per physician discretion, which likely had an impact on the assessment of the primary endpoint. pCR was observed only in women with grade 3 tumors and predominantly in those with triple-negative disease. Interestingly, of those with ER- or PR-positive tumors who experienced a pCR, 2 patients had BRCA mutations, suggesting that CP may warrant further evaluation in this population. These results are reflective of the high pCR rate observed, irrespective of hormone receptor status, in a recent study of neoadjuvant cisplatin in patients with BRCA1 mutations (13).
Early change in SUV on 18F-FDG PET has been investigated as a predictor of response to PST (8). In a prospective trial in which 104 patients with large (≥3 cm) or locally advanced breast cancer were randomized to 2 anthracycline/taxane-based neoadjuvant chemotherapy regimens, 18F-FDG PET scans were obtained at baseline and after 1 and 2 cycles of chemotherapy (14). A threshold of 45% decrease in SUV after the first cycle of chemotherapy correctly identified 11 of 15 patients who obtained a pCR, and those who did not obtain a pCR were identified with a negative predictive value of 90%. After the second cycle of chemotherapy, a threshold of 55% relative decrease in SUV predicted pCR. We enrolled a similar patient population, and all participants received a relatively homogeneous chemotherapy regimen. A meta-analysis of 19 studies and 920 patients with pCR aimed to predict pathologic response in primary breast lesions by 18F-FDG PET (15). The best correlation with pCR used a 55%–65% reduction rate cutoff value of SUV. An exploratory receiver-operating-characteristic analysis from our study indicated that a 52% reduction in SULmax predicted pCR, with a sensitivity of 75%, specificity of 74%, negative predictive value of 89%, and positive predictive value of 52% (area under the curve, 0.76; 95% CI, 0.60–0.91). Other studies performed to date have been predominantly retrospective and associated with significant heterogeneity of the breast cancer subtypes investigated, chemotherapy administered, timing of imaging in relation to chemotherapy, and definitions of response to therapy (14,16–19). The significant difference we observed in median percentage reduction in SULmax on 18F-FDG PET between pathologic responders and nonresponders in a pooled analysis with a relatively large odds ratio suggests that SULmax is a promising biomarker for early prediction of treatment response to this regimen. Coupled with others, our results provide valuable data regarding the optimal cut point of reduction in SULmax, which can be used in future studies designed to assess whether altering therapy based on early changes will be associated with improved pCR. This study was designed before the PET Response Criteria in Solid Tumors 1.0 were published, but it is expected that SULpeak (the highest-valued 1-cm3 spheric volume of interest for which the center point lies within the volume boundary) changes would provide similar results, possibly with greater precision than SULmax (11).
Strengths of our study include the multicenter prospective randomized and placebo-controlled design. All 62 patients underwent baseline 18F-FDG PET and biopsy, with almost all patients undergoing serial 18F-FDG PET scans and biopsies, an invaluable resource for correlative analyses. Study sites were provided with 18F-FDG PET imaging protocol recommendations to achieve a high level of multisite consistency. This consistency was documented by a few cases with uptake periods outside the specified range of 50–70 min after injection (n = 10/62), only 3 patients with blood sugar readings at the time of imaging in excess of 150 mg/dL, though all were below 200 mg/dL, and different scanners being used between baseline and follow-up scans in only 3 of the 62 cases. Because of the small numbers involved, it is unlikely that the use of different scanners between baseline and follow-up affected the study results. Central analysis of 18F-FDG PET was successful, and 90% of images were evaluable for change in SULmax. Finally, we chose an early time point for the second 18F-FDG PET scan (after 2 wk) to define as early as possible in the treatment paradigm those patients who will benefit from an alternative approach. A rapid and significant decrease in glucose metabolism as early as 8 d after the administration of 1 cycle of combination chemotherapy in women who responded to the regimen has been previously observed and can allow for a rapid change in therapy for women who are not expected to derive benefit (8). This has theoretic advantages over later time points in terms of discrimination abilities between pCR and non-pCR (11,20).
Limitations of our study include that a proportion of women received additional anthracycline-based preoperative chemotherapy after study treatment, which may complicate both the evaluation of our primary endpoint and the role of 18F-FDG PET in predicting treatment response. However, post hoc sensitivity analysis, which excluded patients who received preoperative nonstudy chemotherapy, yielded similar results (Supplemental Tables 3 and 4). Only 72% of matched samples were evaluable for Ki-67 analysis, partly because of the lack of viable tumor cells in C1D15 specimens, which may have been due to early treatment effect. The challenges surrounding serial Ki-67 measurement in tumor samples have been previously described (21). These results suggest that the ability to quantify and image the entire tumor by 18F-FDG PET imaging may be an advantage over a biopsy of a small region of tumor. In a small number of cases (n = 4), baseline study biopsy was performed before 18F-FDG PET, which may have inflated the SULmax value due to an inflammatory response. The cost associated with serial 18F-FDG PET imaging, as well as additional radiation exposure over and above standard of care, may also be a barrier to implementing change in SULmax as a treatment-selection biomarker in the clinic. However, a noninvasive biomarker that is readily available may be preferable to a tissue-based biomarker, which requires additional procedures for patients. Our study did not incorporate serial MR imaging, which may be an alternative to 18F-FDG PET and associated with less radiation exposure (20). Newer 18F-FDG PET cameras and CT algorithms can also acquire high-quality images with lower radiation doses.
CONCLUSION
Our study confirms the feasibility of conducting multicenter neoadjuvant studies that add novel agents to chemotherapy backbones and incorporate serial tissue biopsies and quantitative imaging for biomarker development. Although our study did not indicate a benefit for the addition of vorinostat to CP, the pCR rate observed suggests a potential role for platinum agents in specific breast cancer subtypes, namely high-grade triple-negative or BRCA-associated tumors. Future studies will use the optimal cut point of reduction in SULmax we have identified to determine whether altering therapy based on early changes in SULmax is of clinical utility.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. Research support for this study was provided by the Specialized Program of Research Excellence in Breast Cancer (P50 CA88843), NCI Quantitative Imaging Network (QIN) contract (5U01CA140204), Imaging Response Assessment Core Lab (3 P30 CA006973), Abraxis Bioscience, Merck & Co, Inc., and the Cindy Rosencrans Fund for Triple Negative Breast Cancer Research. Support was also from the Translational Breast Cancer Research Consortium (TBCRC) from the AVON Foundation, the Breast Cancer Research Foundation, and Susan G. Komen for the Cure. Vorinostat and placebo were supplied by Merck & Co, Inc. Nanoparticle albumin-bound paclitaxel (nab-paclitaxel) was supplied by Abraxis Bioscience (Celgene Corporation). Support was also provided by QVC and Fashion Footwear Association of New York (FFANY). Vered Stearns has received research grants from Merck & Co. Inc., Abraxis Bioscience (Celgene Corporation), Abbott, Pfizer, Novartis, and Medimmune. Roisin M. Connolly has received research grants from Novartis, Puma Biotechnology, and Genentech. Richard L. Wahl has received research grants from GlaxoSmithKline and Actinium Pharmaceuticals. John Carpenter has received an honorarium from Genentech and consultant fee from Sanofi Aventis. No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank Michael Carducci, MD, for independent review of interim data. We thank Gary Rosner, ScD, for a critical review of the manuscript.
Footnotes
Published online Dec. 4, 2014.
- © 2015 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication July 1, 2014.
- Accepted for publication November 4, 2014.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- 18F-Fluoroestradiol PET Imaging in a Phase II Trial of Vorinostat to Restore Endocrine Sensitivity in ER+/HER2- Metastatic Breast Cancer
- Utilizing novel fluorothymidine PET imaging in a phase I study of veliparib on an intermittent and continuous schedule given in combination with carboplatin in metastatic breast cancer
- Association of Tumor-Infiltrating Lymphocytes with Homologous Recombination Deficiency and BRCA1/2 Status in Patients with Early Triple-Negative Breast Cancer: A Pooled Analysis
- FDG-PET/CT and MRI for Evaluation of Pathologic Response to Neoadjuvant Chemotherapy in Patients With Breast Cancer: A Meta-Analysis of Diagnostic Accuracy Studies
- 18F-FDG PET/CT for the Early Evaluation of Response to Neoadjuvant Treatment in Triple-Negative Breast Cancer: Influence of the Chemotherapy Regimen
- Quo Vadis: PET and Single-Photon Molecular Breast Imaging
- Multicenter Clinical Trials Using 18F-FDG PET to Measure Early Response to Oncologic Therapy: Effects of Injection-to-Acquisition Time Variability on Required Sample Size
- Predictive Value of Positron Emission Tomography/Computed Tomography to Assess Early Treatment Response to Dual Human Epidermal Growth Factor Receptor 2 (HER2) Blockade Without Chemotherapy for HER2-Positive Metastatic Breast Cancer: Are We Ready to Embrace This "Early Metabolic Look" Strategy?
- Measuring Tumor Metabolism by 18F-FDG PET Predicts Outcome in a Multicenter Study: A Step Off in the Right Direction