


Abstract
This study was performed to investigate the role of 68Ga-DOTANOC SUVmax as a potential prognostic factor in patients with pancreatic neuroendocrine tumor (pNET). Methods: Among the patients who underwent 68Ga-DOTANOC PET/CT, we retrospectively collected the data of those who had G1 or G2 pNET (2010 World Health Organization classification), presented with disease on PET/CT and CT, and had at least 6 mo of follow-up. Patients with multiple endocrine neoplasia were excluded. Results: Overall, 43 patients were included. No significant differences in SUVmax were observed with respect to sex, tumor syndrome, stage, World Health Organization classification, or Ki-67. During follow-up (median, 20 mo), 11 patients (35.6%; median, 33 mo; interquartile range, 20–48 mo) had stable disease and 32 (74.4%; median, 19 mo; interquartile range, 14–26 mo) had progressive disease. SUVmax at 24 mo of follow-up was significantly higher (P = 0.022) in patients with stable disease than in patients with progressive disease. The best SUVmax cutoff ranged from 37.8 to 38.0. The major risk factors for progression included an SUVmax of no more than 37.8 (hazard ratio, 3.09; P = 0.003), a Ki-67 of more than 5% (hazard ratio, 2.89; P = 0.009), and medical therapy alone (hazard ratio, 2.36; P = 0.018). Advanced stage (IV) (P = 0.026), an SUVmax of less than 37.8 (P = 0.043), and medical therapy alone (P = 0.015) were also confirmed at multivariate analysis. Median progression-free survival was 23 mo. Significant differences in progression-free survival were observed in relationship to Ki-67 (median, 45 mo for Ki-67 ≤ 5% and 20 mo for Ki-67 > 5%; P = 0.005), SUVmax (<37.8 vs. >38.0: 16.0 vs. 27.0 mo; P = 0.002), and type of therapy (medical vs. peptide receptor radionuclide therapy: 16.0 vs. 26.0 mo; P = 0.014). Conclusion: 68Ga-DOTANOC SUVmax is a relevant prognostic factor in patients with G1 and G2 pNET, and its routine use will improve disease characterization and management in these patients, who may present with atypical cases showing heterogeneous clinical behavior.
Pancreatic neuroendocrine neoplasms (pNETs) are considered rare, with a wide spectrum of clinical presentation. Their real incidence is quite controversial: although they are found in about 1% of autopsies, their clinical incidence is reported to be only about 0.5–1/100,000 (1,2). Although pNETs are characterized by an overall better prognosis than other forms of solid tumor, patient outcome can vary greatly depending on tumor grade (3) and disease extent (4). However, the improved diagnostic and therapeutic management of these patients has led to an increase in prevalence of the disease, and in turn, atypically presenting cases showing heterogeneous clinical behavior have increased, either at diagnosis or during the course of the disease. Therefore, the possibility of identifying prognostic parameters that may help clinicians stratify patients into different risk groups is extremely relevant.
The diagnostic flowchart for pNETs currently includes several imaging modalities, both morphologic (sonography, CT, MRI) and functional (somatostatin receptor scintigraphy, PET/CT with 68Ga-DOTA-peptides) (5–7). In the past 5 y, PET/CT with 68Ga-DOTA-peptides has been increasingly used for its high accuracy in detecting lesions (at both primary and metastatic sites), safety, contained costs (5–7), and ability to select patients for whom peptide receptor radionuclide therapy (PRRT) is appropriate.
Once the tumor is detected, the possibility of identifying accurate prognostic factors for disease progression is crucial to the management of these patients. Studies have investigated the role of grading, staging, functioning status, and somatostatin receptor density as potential prognostic factors in pNETs (8). Two studies indicated that SUVmax measured in the lesion with the highest 68Ga-DOTANOC uptake was a prognostic parameter in heterogeneous populations of neuroendocrine tumors with different primary sites (including gastroenteropancreatic and lung tumors) (9,10).
However, since pNETs may present a clinical course different from that of NETs with other primary sites (8,11), the aim of the present study was to investigate whether SUVmax measured at 68Ga-DOTANOC PET/CT may be used as a prognostic factor in NET patients with a pancreatic primary.
MATERIALS AND METHODS
Among the patients who underwent 68Ga-DOTANOC PET/CT at our PET center from September 2006 to October 2014, we retrospectively collected the data of those with pathologically proven G1 or G2 pNET (2010 World Health Organization [WHO] classification) (3). The additional two inclusion criteria were the presence of disease at both 68Ga-DOTANOC PET/CT and CT (performed within a month of each other) and at least 6 mo of clinical follow-up.
Patients with multiple endocrine neoplasia syndrome type 1, a condition well known to present with clinical behavior different from that of other gastroenteropancreatic NETs, were excluded from the analysis.
All patients underwent physical examination, and their clinical history was taken with the aim of investigating the putative clinical features of the functioning tumors. Laboratory and radiologic examinations were performed to evaluate the location of the tumor and to stage the disease. According to recent literature on pNETs, patients were divided into two groups according to a Ki-67 cutoff of 5% (8,12,13).
The presence of clinical symptoms associated with an increase in serum peptide levels was used to identify patients with functioning tumors.
Clinical follow-up was performed at the internal medicine outpatient service dedicated to pNET patients and included a CT scan every 3 mo during the first year and every 6 mo afterward.
Treatment after PET/CT with everolimus (10 mg daily of Afinitor [Novartis]), cold somatostatin analogs alone every 28 d (30 mg of octreotide acetate [Sandostatin LAR; Novartis] or 120 mg of lanreotide acetate [Somatuline Autogel; Ipsen]), or cold somatostatin analogs in association with PRRT was recorded.
All patients gave written informed consent to participate in the study. The study protocol was approved by the local Ethical Committee of the S. Orsola–Malpighi Hospital and was performed according to the Helsinki Declaration for human studies.
PET/CT with 68Ga-DOTANOC was performed following current international guidelines (intravenous injection of 120–185 MBq followed by an uptake time of 60 min [range, 45–90 min], without specific examination preparation) (14). 68Ga-DOTANOC was synthesized by the Radiopharmacy of the Nuclear Medicine Unit of S. Orsola–Malpighi Hospital. 68Ga was eluted from a 68Ge/68Ga generator, and DOTANOC was labeled with 68Ga following the procedure described by Zhernosekov et al. (15). 68Ga-DOTANOC PET scans were obtained using a dedicated PET/CT scanner (Discovery LS; GE Healthcare). PET emission images were recorded for 4 min per bed position; CT images were used for nonuniform attenuation correction (acquisition parameters, 140 kV, 90 mA, 0.8-s tube rotation, 5-mm thickness). All images were corrected for scatter, randoms, dead time, and decay. Images were reconstructed with a 2-dimensional ordered-subset expectation maximization iterative algorithm (2 iterations, 28 subsets).
PET/CT images were acquired from the skull base to the middle of the thigh. PET/CT results were evaluated by 2 skilled nuclear medicine specialists unaware of the results of the other imaging modalities, and the definitive report was reached by consensus. Any localization with an intensity greater than background that could not be explained by physiologic activity (pituitary gland, spleen, liver, adrenals, kidneys, or urinary bladder) was considered to indicate somatostatin receptor expression.
SUVmax was calculated by measuring the maximal concentration of the labeled tracer in the region of interest corrected for body weight and injected dose (SUVmax = maximum activity concentration/[injected dose/body weight]) (16). For each PET scan, SUVmax was measured by choosing the region of interest in the lesion with the highest tracer uptake. For large tumors, the region of interest was moved over several sites within the mass to ensure that the true SUVmax was obtained.
All data were collected, and a computerized data sheet was created. Data on demographic, clinical, and pathologic features were retrospectively analyzed. The tumors were classified according to the 2010 WHO classification (3), and the novel TNM classification/G grading system (4). The Ki-67 proliferation index was expressed as the percentage of Ki-67–positive cells in 2,000 tumor cells in the most highly immunostaining areas using the MIB1 antibody (DBA). The tumors were measured and scored according to RECIST (17).
Median values and the respective interquartile range (IQR, 25th–75th percentile) were used to describe the data. Groups were compared using the Pearson χ2 test (the Fisher exact test was used when necessary) or the Mann–Whitney U test for continuous variables. The area under the receiver-operating-characteristic curve was evaluated to determine the accuracy of SUVmax at diagnosis in predicting disease progression. The best prognostic cutoff was estimated by a maximum-likelihood-ratio method.
Progression-free survival (PFS) was defined as the interval between 68Ga-DOTANOC PET/CT and the time of disease progression. PFS was measured using the Kaplan–Meier method, and the results were compared using the log-rank test. The predictive risk factors for progressive disease were analyzed by univariate and multivariate analysis using the Cox proportional-hazards method. Risk factors were expressed as hazard ratios and 95% confidence intervals. The multivariate model was constructed using the forward-stepwise method after all variables had been included. All analyses performed for risk factors are listed in the tables.
The P value was considered significant when less than 0.05. Statistical analysis was performed using dedicated software (SPSS, version 19.0; IBM).
To evaluate the potential role of SUVmax on prognosis, we divided the patients on the basis of disease status (progressive disease vs. stable disease) at an arbitrarily selected follow-up time point. A 24-mo time point was chosen for three reasons: about half our patients underwent PRRT; PFS in patients treated with PRRT was 23 mo in the pancreatic subgroup of a recent multicenter trial (18); and our follow-up schedule included a radiologic evaluation at 24 mo (CT every 3 mo during the first year and every 6 mo afterward).
RESULTS
Patient Characteristics
Overall, 43 patients (22 men and 21 women; median age, 58 y; IQR, 48–64 y) with pNETs were included in the study. Eight patients (18.6%) had functioning tumors: 5 gastrinomas, 1 insulinoma, 1 VIPoma (vasoactive intestinal peptide–secreting tumor), and 1 ACTHoma (adrenocorticotropin hormone–secreting tumor). In the remaining 35 patients (81.4%), the tumor was nonfunctioning. According to the 2010 WHO classification, 14 patients (32.3%) had a G1 pNET and 29 (67.7%) a G2 pNET.
The median Ki-67 index was 6.1% (IQR, 2.0%–8.9%); 22 of 43 patients (51.2%) had a Ki-67 of 5% or less, and 21 of 43 patients (48.8%) had a Ki-67 of more than 5%. According to the TNM classification, 7 patients (16.3%) had stage IIIB disease and 36 (83.7%) stage IV.
The characteristics of all 43 patients are listed in Table 1.
SUVmax Median and IQR (25th–75th Percentiles) Among Different Groups of Patients
68Ga-DOTANOC SUVmax
Data on median SUVmax and the respective IQRs (25th–75th percentiles) among the different groups of patients are reported in Table 1. There were no significant differences with respect to sex, presence of tumor syndrome, stage, and 2010 WHO classification.
Follow-up
All patients were evaluated for a median of 20 mo (IQR, 15–33 mo). Twenty of the 43 patients (46.5%) were treated with medical therapy: 13 with long-acting somatostatin analogs alone (Sandostatin LAR [30 mg] every 28 d or Somatuline Autogel [120 mg] every 28 d), 2 with long-acting somatostatin analogs plus everolimus (Afinitor [10 mg] every day), and 5 with everolimus alone. Twenty-three (53.5%) had combined treatment with both long-acting somatostatin analogs and PRRT.
During follow-up, 11 patients (35.6%; median, 33 mo; IQR, 20–48 mo) had stable disease and 32 (74.4%; median, 19 mo; IQR, 14–26 mo) had disease progression.
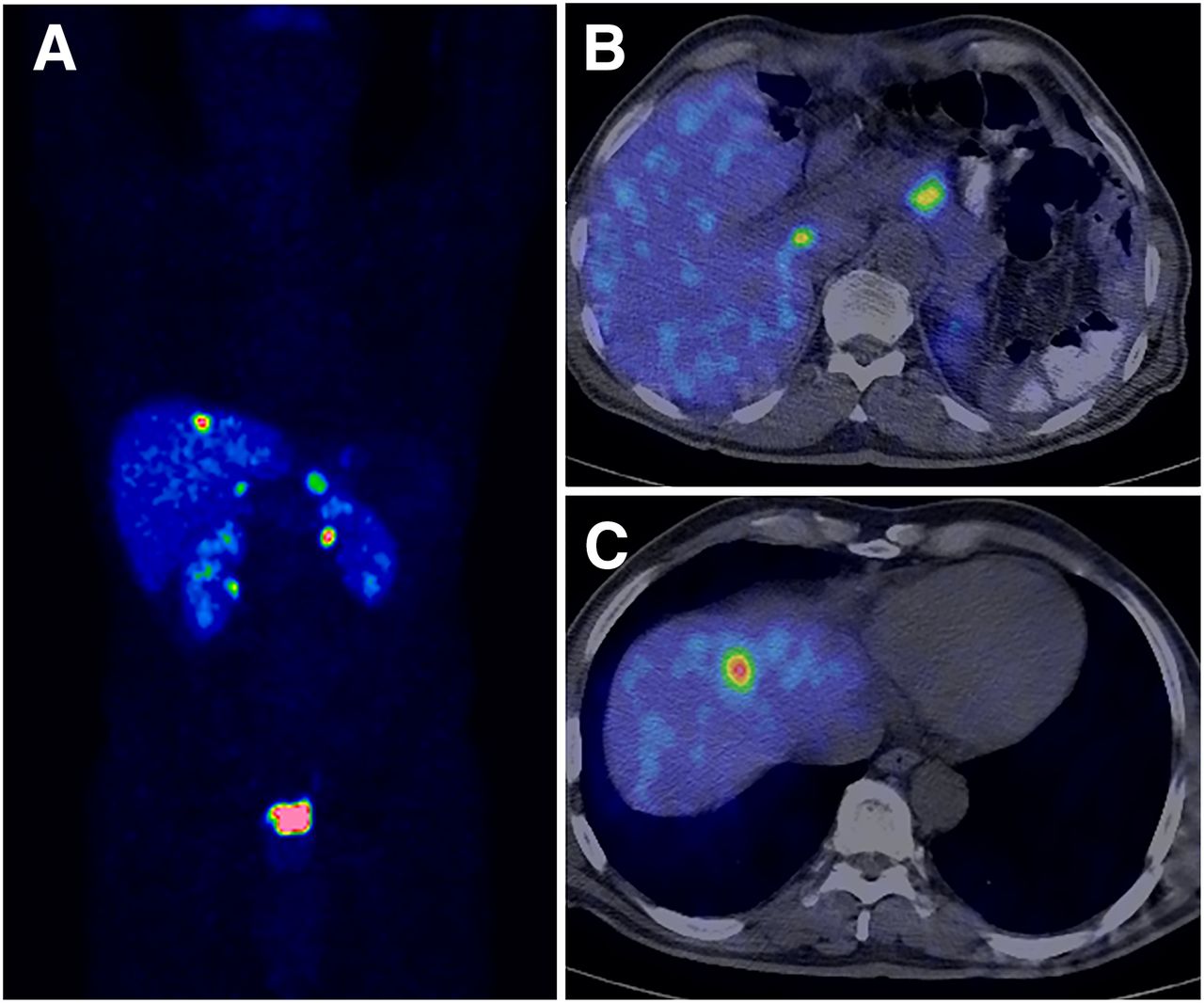
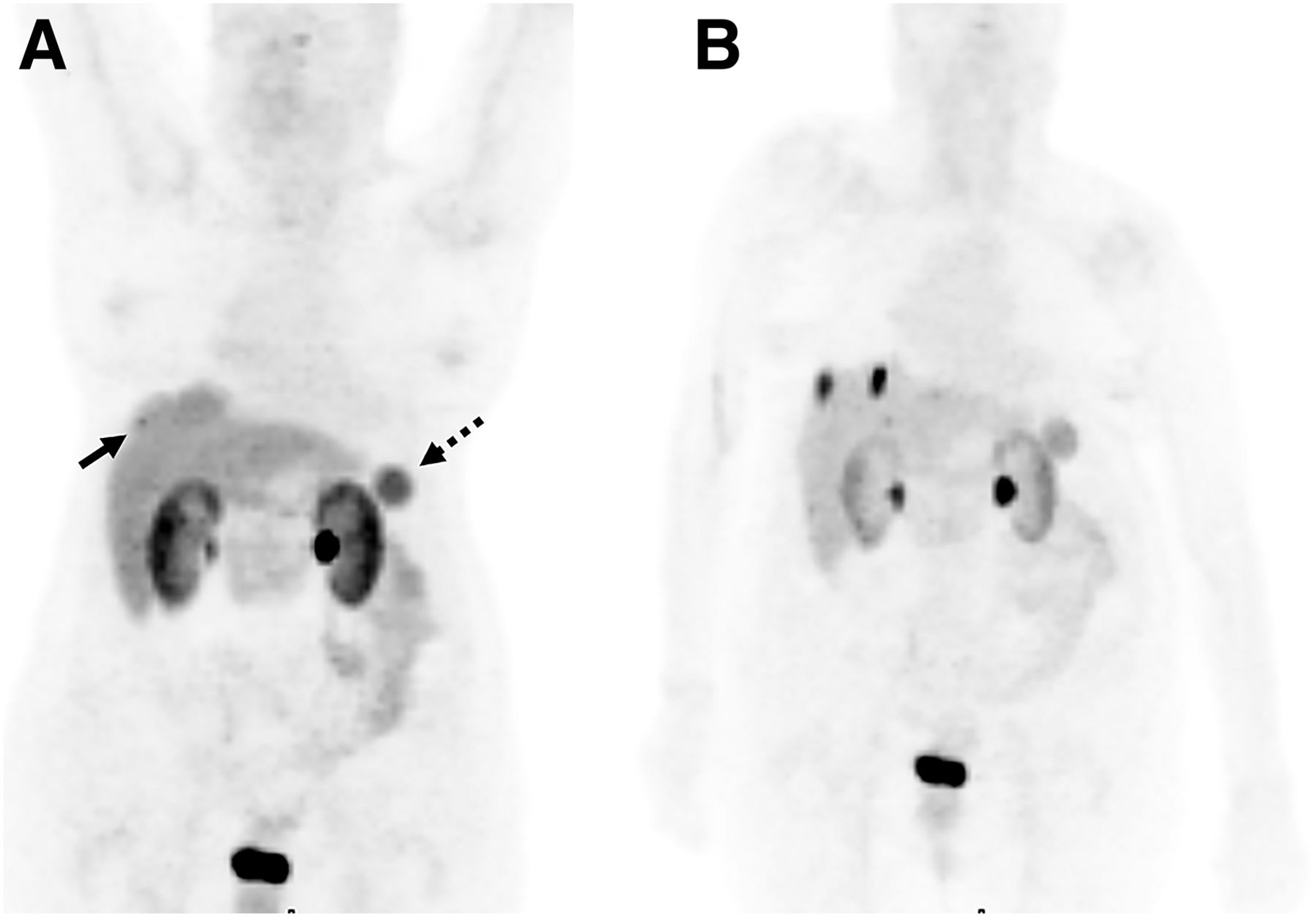
To evaluate the potential role of SUVmax on prognosis, we divided the patients on the basis of disease status (progressive vs. stable) at 24 mo of follow-up. As reported in Table 1, SUVmax was significantly higher (P = 0.022) in patients with stable disease (Fig. 1) (18 patients; median, 49.8; IQR, 44.9–78.8) than in patients with progressive disease (20 patients; median, 33.4; IQR, 26.1–52.4; Fig. 2). Five patients were not included in the analyses because they had stable disease and less than 24 mo of follow-up.
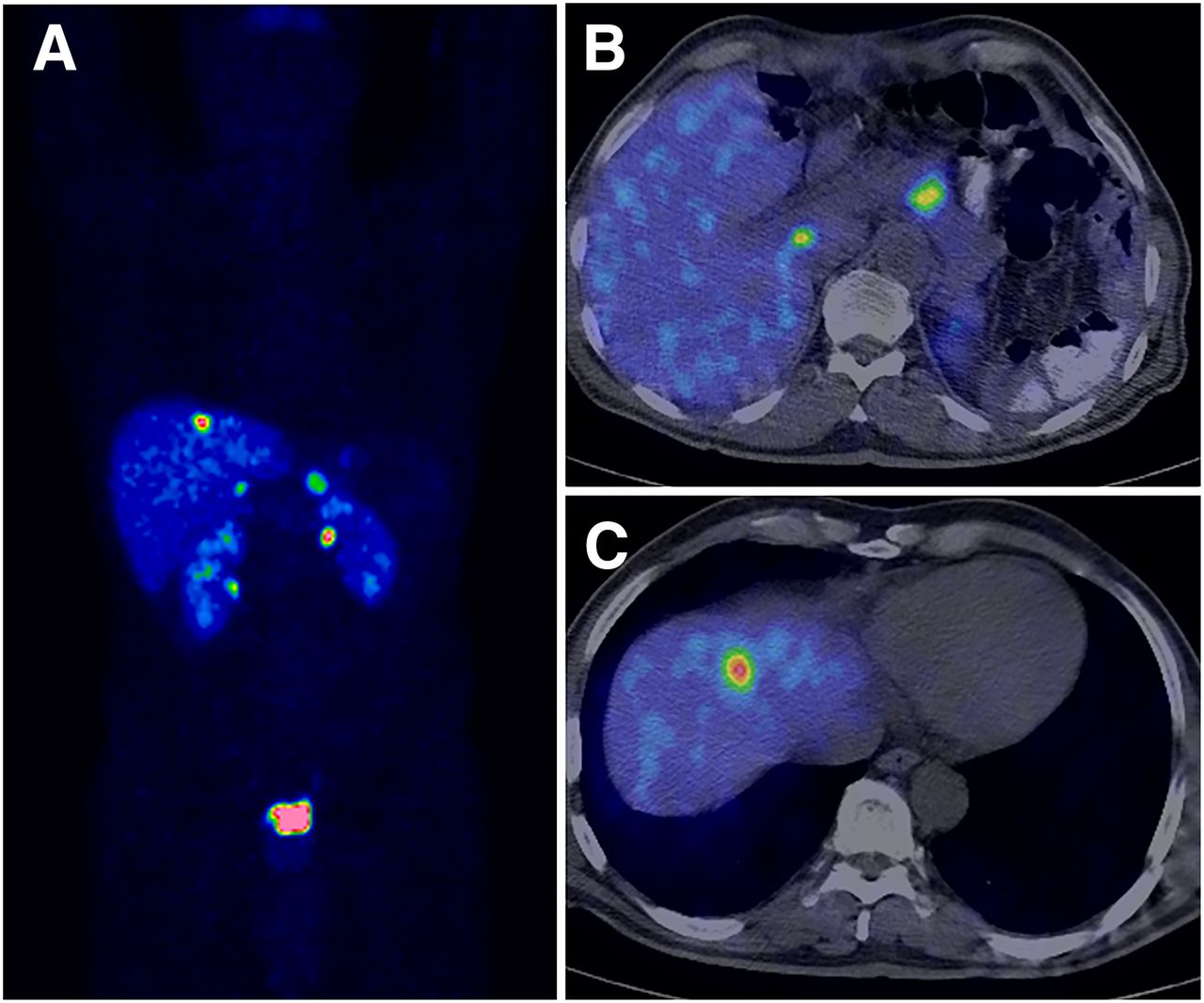
68Ga-DOTANOC PET/CT maximum-intensity-projection (A) and transaxial images (B and C) of patient with G2 pNET (A and B) and liver metastasis (A and C). Measured SUVmax was 56. Patient had stable disease at follow-up.
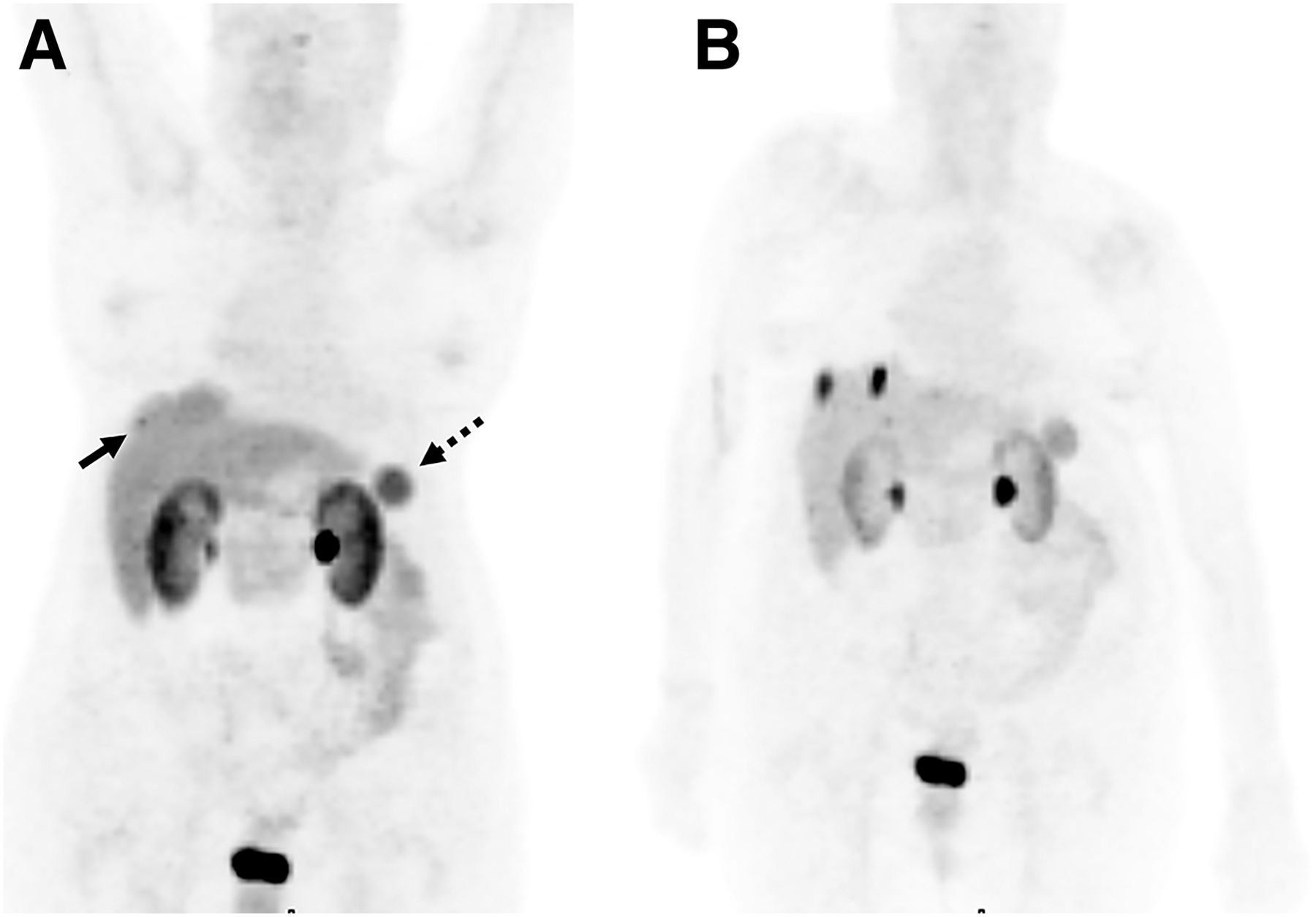
(A) 68Ga-DOTANOC PET/CT maximum-intensity-projection images of patient who previously underwent surgery for pNET and presented with liver metastasis having SUVmax of 6.7 (solid arrow). (B) Patient showed disease progression at follow-up. Dashed arrow indicates accessory spleen.
The receiver-operating-characteristic curve of SUVmax was quite accurate in predicting patients who had progressive disease after 24 mo of follow-up (area under the curve ± SE, 0.715 ± 0.084; P = 0.023), and the best cutoff ranged from 37.8 to 38.0. The sensitivity and specificity obtained using the best cutoff were 72.2% and 70.0%, respectively.
Predictors for Tumor Progression
The variables found by univariate analysis to be risk factors for tumor progression are summarized in Table 2. Risk factors for tumor progression were an SUVmax of no more than 37.8 (HR, 3.09; P = 0.003), medical therapy alone (HR, 2.36; P = 0.0148), and a Ki-67 of more than 5% (HR, 2.89; P = 0.009). The variables found by multivariate analysis to be risk factors for tumor progression were a Ki-67 of more than 5% (HR, 3.24), stage IV (HR, 3.31), medical therapy alone (HR, 2.70), and an SUVmax of no more than 37.8 (HR, 2.37).
Risk Factors for Disease Progression During Follow-up at Univariate and Multivariate Analysis
PFS
Median PFS was 23 mo (Fig. 3). Significant differences in PFS were observed in relationship to Ki-67 (median, 45 mo for Ki-67 ≤ 5% and 20 mo for Ki-67 > 5%; P = 0.005; Fig. 3A), SUVmax (<37.8 vs. >38.0: 16.0 vs. 27.0 mo; P = 0.002; Fig. 3B), and type of therapy (medical vs. PRRT: 16.0 vs. 26.0 mo; P = 0.014; Fig. 3C). No significant difference was found according to the 2010 WHO classification (NET G1 vs. NET G2: 30.0 vs. 23.0 mo; P = 0.097), disease stage (IIIB vs. IV: 46.0 vs. 20.0 mo; P = 0.195), or functioning status (functioning vs. nonfunctioning: 26.0 vs. 20.0 mo; P = 0.191).

PFS in 43 patients with well-differentiated pNET (G1 and G2) according to Ki-67 (A) (dashed line = Ki-67 > 5%; solid line = Ki-67 < 5%; P = 0.005), SUVmax (B) (dashed line = SUVmax < 37.8; solid line = SUVmax > 38; P = 0.002), and treatment (C) (dashed line = medical therapy; solid line = medical therapy plus PRRT; P = 0.014).
DISCUSSION
In the past decade, both optimization of diagnostic algorithms (especially after the advent of 68Ga-DOTA-peptide PET/CT) and use of novel therapeutic strategies (mainly PRRT and biologic target drugs) determined an increase in NET prevalence. Correspondingly, clinicians witnessed an increment of atypical cases that did not fit the classic paradigm that NETs are always indolent. Therefore, identification of easily assessable prognostic parameters is crucial for an accurate evaluation both at baseline and during the course of the disease, since an initially indolent tumor may become aggressive. SUVmax is an optimal parameter because it can easily be assessed in a relatively noninvasive way. Moreover, being a whole-body procedure, PET/CT provides a functional evaluation of the whole tumor burden that is not feasible with the commonly used Ki-67.
There is much literature on 68Ga-DOTA-peptide PET/CT focused on assessing diagnostic accuracy (5,7) and comparing the performance of one tracer with another (19,20).
Unlike the potential prognostic role of 18F-FDG SUVmax (21,22), that of 68Ga-DOTA-peptide SUVmax has, to our knowledge, scarcely been investigated. Two papers reported how the 68Ga-DOTANOC SUVmax correlates with somatostatin receptor expression (9,23), and two investigated the potential prognostic role of SUVmax in patients with neuroendocrine tumors with different primary sites (9,10). However, pNETs generally show more aggressive clinical behavior than other forms of NET (8,11), with 5-y survival rates ranging between 25% and 75% (2,24,25). Therefore, the identification of specific prognostic factors assessed in a homogeneous population of NET patients with a pancreatic primary is mandatory.
In view of these clinical needs, the population under study included only patients with a pancreatic primary and a long follow-up (median, 20 mo); cases of multiple endocrine neoplasia (a condition known to present a different clinical behavior) were excluded.
Our study showed that SUVmax may be used to predict outcome in pNET patients. In particular, a higher SUVmax was associated with a better outcome. The best cutoff to discriminate between patients with stable disease or partial response and those with progressive disease ranged between 37.8 and 38.0. This range is higher than those reported in either previous study that included patients with different primary sites (19.3 and 14.5, respectively) (9,10). The explanation may in part be the documented higher SUVmax of the pancreatic primary tumors (9). A report by O’Toole et al. (26) noted a higher level of somatostatin receptor 2 and 5 messenger RNA in neuroendocrine tumor patients with a pancreatic primary than in those with a different primary.
To our knowledge, ours is the first report of the role of SUVmax in predicting PFS in pNETs. Several reports have analyzed the role of different prognostic factors in PFS. In particular, Panzuto et al. described the role of poorly differentiated tumors with a Ki-67 of more than 5% and no treatment after diagnosis as a risk factor for disease progression on multivariate analysis (8). In line with such results, our data support the use of a Ki-67 cutoff of 5% for differentiating patients who will present with more aggressive disease from those with more indolent disease (as opposed to the widely accepted cutoff of 2%, which is used for NETs with other primary sites) (8).
Recently, there has been much attention on the potential role of double-tracer imaging (68Ga-DOTA-peptide/18F-FDG) for a complete biologic characterization of the disease, since a poorer prognosis is generally driven by the presence of one or more 18F-FDG–positive lesions. This approach may overcome the inherent limitations of Ki-67 tissue sampling (invasive assessment of only the biopsied site and the use of different manual and automated digital image analyses for its quantification). Although several papers have addressed this issue (27,28), larger prospective studies are needed to better clarify which patients may most benefit from double-tracer imaging and when it should be performed during the course of the disease. The latter is certainly a relevant issue, in terms of both health care costs and radioprotection, in view of the longer life expectancy of most of these patients. Interestingly, in a recent study by Sharma et al. (10) performed on a limited number of NETs with different primary sites and including cases of multiple endocrine neoplasia syndrome type 1, only SUVmax measured on 68Ga-DOTANOC imaging was reported to correlate with prognosis (18F-FDG SUVmax did not). Several reports indicated that when positive, 18F-FDG is associated with a worse prognosis, although to our knowledge most studies investigated the impact on PFS of 18F-FDG positivity and not the role of SUVmax specifically (27,28). Recently, in a population of 20 pNET patients undergoing pretreatment evaluation with 18F-FDG PET/CT, Kim et al. (29) reported the potential utility of the metabolic tumor volume of the primary tumor, along with American Joint Committee on Cancer stage, as an independent prognostic factor for overall survival.
The current treatment approach to pNETs is not standardized, and several different options, not mutually exclusive, are available (30). Phase 3 clinical trials have been performed only for the long-acting somatostatin analogs everolimus and sunitinib. Although biased by the retrospective nature of data collection, our results showed a longer PFS in patients treated with PRRT (26 vs. 16 mo). This finding is in line with previous reports of pNET PFS in a recently published retrospective multicenter analysis (23 mo) (18) on radiolabeled somatostatin analog treatment. Acknowledging the inherent problems of interstudy comparisons, the reported effect of PRRT on PFS (18,31–33) seems to be superior to that of chemotherapy (median PFS < 18 mo) (34,35) or targeted therapies such as sunitinib (11.4 mo) (36) and everolimus (11.0 mo) (37).
The results reported in this paper therefore support the role of PRRT in the therapeutic management of pNET patients and underline the need to standardize regimens over different centers and countries. In fact, for PRRT, only practical guidance signed by the International Atomic Energy Agency, European Association of Nuclear Medicine, and Society of Nuclear Medicine and Molecular Imaging is currently available (30).
CONCLUSION
68Ga-DOTANOC SUVmax is a demonstrated prognostic parameter in patients with well-differentiated pNETs (G1 and G2) and should be used in clinical practice in association with other known prognostic factors to foresee patient outcome. Considering that different 68Ga-DOTA-peptides are currently available for neuroendocrine tumor imaging and the fact that the corresponding SUVmax is not directly comparable, specific studies are needed to establish cutoffs for other β-emitting somatostatin analog tracers.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Sep. 24, 2015.
- © 2015 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication June 25, 2015.
- Accepted for publication September 14, 2015.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Semiautomatic Tumor Delineation for Evaluation of 64Cu-DOTATATE PET/CT in Patients with Neuroendocrine Neoplasms: Prognostication Based on Lowest Lesion Uptake and Total Tumor Volume
- Somatostatin Receptor Imaging and Theranostics: Current Practice and Future Prospects
- 64Cu-DOTATATE PET/CT and Prediction of Overall and Progression-Free Survival in Patients with Neuroendocrine Neoplasms