


Abstract
Echocardiography plays a key role in the diagnosis of infective endocarditis (IE) but can be inconclusive in patients in whom prosthetic valve endocarditis (PVE) is suspected. The incremental diagnostic value of 18F-FDG PET and radiolabeled leukocyte scintigraphy in IE patients has already been reported. The aim of this study was to compare the respective performance of 18F-FDG PET and leukocyte scintigraphy for the diagnosis of PVE in 39 patients. Methods: 18F-FDG PET and leukocyte scintigraphy were performed on 39 consecutive patients admitted because of clinically suspected PVE and inconclusive echocardiography results. The results of 18F-FDG PET and leukocyte scintigraphy were analyzed separately and retrospectively by experienced physicians masked to the results of the other imaging technique and to patient outcome. The final Duke–Li IE classification was made after a 3-mo follow-up. Results: Of the 39 patients, 14 were classified as having definite IE, 4 as having possible IE, and 21 as not having IE. The average interval between 18F-FDG PET and leukocyte scintigraphy was 7 ± 7 d. Sensitivity, specificity, positive predictive value, negative predictive value, and accuracy were 93%, 71%, 68%, 94%, and 80%, respectively, for 18F-FDG PET and 64%, 100%, 100%, 81%, and 86%, respectively, for leukocyte scintigraphy. Discrepancies between the results of 18F-FDG PET and leukocyte scintigraphy occurred in 12 patients (31%). In patients with definite IE, 5 had true-positive 18F-FDG PET results but false-negative leukocyte scintigraphy results. Of these 5 patients, 3 had nonpyogenic microorganism IE (Coxiella or Candida). Of patients for whom endocarditis had been excluded, 6 had true-negative leukocyte scintigraphy results but false-positive 18F-FDG PET results. These 6 patients had been imaged in the first 2 mo after the last cardiac surgery. The last patient with a discrepancy between 18F-FDG PET and leukocyte scintigraphy was classified as having possible endocarditis and had positive 18F-FDG PET results and negative leukocyte scintigraphy results. Conclusion: 18F-FDG PET offers high sensitivity for the detection of active infection in patients with suspected PVE and inconclusive echocardiography results. Leukocyte scintigraphy offers a higher specificity, however, than 18F-FDG PET for diagnosis of IE and should be considered in cases of inconclusive 18F-FDG PET findings or in the first 2 mo after cardiac surgery.
- infective endocarditis
- cardiac prosthetic valves
- 18F-FDG positron emission tomography
- radiolabeled leukocyte scintigraphy
Infective endocarditis (IE) is a serious complication of valve replacement and has been reported in 1%–6% of patients with a valve prosthesis (1). Despite improvement in medical treatment and surgery, prosthetic valve endocarditis (PVE) remains associated with a high mortality rate (2,3). Early identification of PVE is of paramount importance, because these patients have a high mortality rate in the absence of antibiotherapy (4). When abscess or extensive perivalvular infection is present, cardiac surgery is usually recommended (5). Echocardiography plays a key role in the diagnosis of PVE, but the presence of endocarditis can be difficult to confirm in patients with cardiac prosthetic material, in particular during the early stages of the infectious process.
Recently, 2 different imaging techniques have demonstrated their incremental value over echocardiography for the diagnosis of endocarditis: 18F-FDG-PET (6,7) and radiolabeled leukocyte scintigraphy (8,9). Each of these techniques presents specific advantages and drawbacks for the detection of infection in patients with suspected PVE. On the one hand, 18F-FDG PET has the advantage of relatively short acquisition times and high sensitivity for the detection of cells with high metabolic activity. 18F-FDG PET does not, however, allow for discrimination between infective and inflammatory processes. In addition, analysis of 18F-FDG uptake in cardiac valves can be hampered by physiologic uptake in the neighboring myocardium. On the other hand, leukocyte scintigraphy offers high specificity for the presence of acute infection when radiolabeled leukocytes accumulate in tissues. However, in vitro radiolabeling of leukocytes requires special equipment, is time-consuming, and involves direct handling of blood products. In addition, imaging with leukocyte scintigraphy is performed over 24 h and has a lower signal than 18F-FDG PET. The precise role of each of these 2 imaging techniques in the diagnosis of PVE still needs to be defined. The aim of this study was to compare the respective performance of 18F-FDG PET and leukocyte scintigraphy for the diagnosis of PVE in a cohort of 39 consecutive patients who underwent both imaging modalities for clinical indications.
MATERIALS AND METHODS
Patient Characteristics
Between May 2010 and July 2013, 39 consecutive patients with a valve prosthesis, patch, or aortic tube implanted by open-chest cardiac surgery admitted to Bichat University Hospital because of suspected PVE underwent both 18F-FDG PET imaging and leukocyte scintigraphy. During this time, 382 patients, including 67 with a cardiac prosthesis, underwent 18F-FDG PET imaging in our institution because of suspected endocarditis, and 50 patients underwent leukocyte scintigraphy because of suspected PVE. Patients were excluded from this study if they had only an implanted stimulation device, a vascular prosthesis, or a left ventricular assist device or if they had complicated PVE requiring immediate surgery. In addition, patients for whom more than 1 mo had passed between 18F-FDG PET and leukocyte scintigraphy imaging were excluded from the study. Clinical characteristics, Duke–Li criteria for the diagnosis of endocarditis (10), and the results of leukocyte scintigraphy and 18F-FDG PET were collected for each patient. All patients underwent initial transesophageal echocardiography with a multiplanar probe by an expert echocardiographer. Abnormal findings on cardiac echocardiography were classified as previously described (8). The Institutional Review Board of Bichat University Hospital approved this study, and all subjects gave written informed consent for review of their records.
18F-FDG PET/CT
Imaging Protocol
Patients received a low-carbohydrate, high-fat meal the evening before 18F-FDG PET imaging and were then asked to fast for least 12 h to limit physiologic myocardial 18F-FDG uptake. Imaging was performed only if the fasting glucose level was lower than 7.7 mmol/L before 18F-FDG injection. 18F-FDG was injected intravenously at a dose of 4 MBq/kg (average total injected dose, 300 MBq). PET and CT were performed with a PET/CT hybrid system (Discovery 690; GE Healthcare). Imaging started 60 min after 18F-FDG injection with a nonenhanced, low-dose CT scan (120 kV, 80 mA), which was followed by a whole-body PET acquisition in 3-dimensional mode with an acquisition time of 4 min per bed position. Transverse PET slices were reconstructed into a 256 × 256 matrix with an iterative 3-dimensional reconstruction algorithm of the system software. Low-dose CT was used for attenuation correction of PET images and for localization of prosthetic and tissue structures. The radiation dose for this acquisition protocol was estimated to be 10 mSv.
Interpretation Criteria
18F-FDG PET acquisitions were interpreted using the Advantage Workstation of the PET/CT system (GE Healthcare) by an experienced nuclear medicine physician masked to the results of leukocyte scintigraphy and to patient outcome. Image analysis was based on visual interpretation and semiquantitative measurement of 18F-FDG uptake using the following previously described criteria (6).
On visual analysis, hypermetabolic activity in the prosthetic or periprosthetic areas was considered abnormal. Increased 18F-FDG uptake in these areas had to be confirmed on non–attenuation-corrected PET images. Visual analysis defined whether PET/CT results were classified as positive or negative. Septic emboli were defined as extracardiac abnormal 18F-FDG uptake in tissue. In addition, the pattern of 18F-FDG uptake in the myocardium was divided into 3 groups: diffuse uptake, focal uptake, and no significant uptake.
In the semiquantitative analysis, the mean standardized uptake value (SUVmean) of the prosthetic area was calculated as the average maximal SUV adjusted for patient weight measured on 3 adjacent axial slices in the prosthetic area with the highest 18F-FDG uptake. SUVmean of blood was calculated as the average SUVmean in 3 adjacent axial slices within the right atrium in areas devoid of significant spillover activity from adjacent tissues. Prosthetic-valve–to–background ratio was calculated by dividing the SUVmean of the prosthetic area by the SUVmean of blood measured in the right atria.
Leukocyte Scintigraphy
Granulocyte Radiolabeling
Leukocytes were labeled with 99mTc using the recommended method (11). Briefly, 50 mL of whole blood were withdrawn from the patient into a syringe containing 10 mL of acid-citrate-dextrose anticoagulant solution. Granulocytes were isolated by sequential blood centrifugation. For granulocyte radiolabeling, hexamethyl propylene amine oxime (Ceretec; GE Healthcare) was labeled with freshly eluted 99mTc (800 MBq) and incubated for 15 min with granulocytes. Radiolabeled granulocytes were separated from hexamethyl propylene amine oxime by a first centrifugation in the presence of platelet-rich plasma at 4,000 rpm for 10 min and a second centrifugation in the presence of plasma at 2,000 rpm for 5 min. Labeling efficiency was measured as a percentage by dividing the radioactivity of the pellet by the radioactivity of the pellet plus supernatant. Labeling efficiency was considered adequate if more than 40%. The cells were then resuspended in plasma and injected directly and slowly into a vein of the patient. The total activity injected ranged from 400 to 500 MBq.
Imaging Protocol
Scintigraphy was performed 4 and 24 h after radiolabeled-leukocyte injection. All images were acquired using a SPECT/CT system (Symbia T2; Siemens). Anteroposterior and oblique planar acquisitions over the chest were obtained at 4 and 24 h after injection of radiolabeled leukocytes (low-energy high-resolution collimators; matrix size, 256 × 256; energy window centered on the 140-keV photopeak of 99mTc using a width of 20%; acquisition time for each planar acquisition, 900 s at 4 h and 1,200 s at 24 h). SPECT/CT was performed over the thorax at 4 and 24 h after injection. A 2-slice CT scan was first acquired over the thorax with a tube current of 110 kV and an intensity of 40–60 mA and was followed by a dual-head SPECT acquisition (matrix size, 128 × 128; 32 projections per detector; 60 s per projection). Images were reconstructed using an ordered-subset expectation maximization algorithm with a Butterworth filter, a cutoff frequency of 1.35 cycles/cm, and 8 iterations without and with attenuation correction based on low-dose CT acquisitions. Transverse, sagittal, and coronal slices of SPECT data were merged with CT using a dedicated workstation (Syngo; Siemens). The radiation dose associated with this imaging protocol was 8 mSv.
Interpretation Criteria
Planar and SPECT/CT acquisitions were analyzed using the Xeleris workstation (GE Healthcare) by an experienced nuclear medicine physician masked to the results of 18F-FDG PET and to patient outcome. Scintigraphy results were classified as positive when foci of labeled leukocyte uptake greater than background activity were detected in the cardiac area and when contrast between these foci and background signal increased over time. Foci of nonphysiologic abnormal uptake that decreased after 24 h were considered nonspecific.
Diagnosis of PVE
The final diagnosis was made by experienced cardiologists according to the clinical and echocardiographic evolution of the patient during a 3-mo follow-up after admission, as well as the presence of an alternate diagnosis explaining the initial infectious syndrome, and was based on the clinical or pathologic modified Duke–Li criteria (10). For patients who underwent surgery after imaging, any visual observations of the cardiac surgeon during the intervention were included in his final report and collected.
Statistical Analysis
Statistical analysis was performed using MedCalc software. Comparisons of values measured in 2 different groups were 2-sided and performed with the Student t test when the number of values was more than 25 and with the Wilcoxon test when the number of values was less than 25. A P value of less than 0.05 was considered significant.
RESULTS
Patient Characteristics
Thirty-nine patients (17 women and 22 men) aged 62 ± 17 y underwent leukocyte scintigraphy and 18F-FDG PET imaging. Patient characteristics are detailed in Tables 1 and 2. The patients were imaged on average 45 mo (range, 14 d to 24 y) after open-chest cardiac surgery. The average time between 18F-FDG PET and leukocyte scintigraphy acquisitions was 7 ± 7 d. Of the 39 patients, 14 were classified before imaging as having definite IE, 19 as having possible IE, and 6 as not having IE based on the modified Duke–Li classification. Antibiotherapy had been started in 28 patients (72%) before imaging. In these patients, the median duration of antibiotic therapy before 18F-FDG PET imaging and leukocyte scintigraphy was not statistically different (15 d [range, 3–326 d] vs. 18 d [range, 3–308 d], P = 0.98). After 3 mo of follow-up, 14 patients were classified as having definite IE, 4 as having possible IE, and 21 as not having IE based on the modified Duke–Li classification.
Patient Characteristics: Previous Cardiac Open-Chest Surgery
Patient Characteristics (Criteria from Modified Duke–Li Classification)
Performance of 18F-FDG PET Imaging
Among the 39 consecutive patients who underwent 18F-FDG PET, 21 (54%) were considered to have positive results. Sensitivity, specificity, positive predictive value, negative predictive value, and accuracy for the diagnosis of PVE were 93%, 71%, 68%, 94%, and 80%, respectively. Myocardial 18F-FDG uptake was graded as elevated, mild, or low in 10 patients (26%), 11 patients (28%), and 18 patients (46%), respectively.
Among the 21 patients with positive 18F-FDG PET results, the final classification at 3 mo was definite IE for 13, possible IE for 2, and no IE for 6. SUVmean at the site of suspected endocarditis was 6.5 (range, 3.9–14.7) in patients with definite IE, 4.4 (range, 4.0–4.8) in patients with possible IE, and 4.9 (range, 3.3–6.2) in patients with no IE (P = 0.08 for the comparison of SUV in patients with definite vs. no IE). Prosthetic-valve–to–background ratios at the site of suspected endocarditis were 4.1 (range, 2.3–7.8) in patients with definite IE, 2.5 (range, 2.3–2.7) in patients with possible IE, and 3.4 (range, 2.4–4.4) in patients with no IE (P = 0.24 for the comparison of prosthetic-valve–to–background ratio in patients with definite vs. no IE). All patients with an SUVmean greater than 6.2 and a prosthetic-valve–to–background ratio greater than 4.4 in the area of suspected endocarditis were classified as having definite PVE. Septic emboli were identified in 5 patients (24%) with positive 18F-FDG PET results. Among the 6 patients with positive 18F-FDG PET results who underwent surgery, PVE was confirmed in 5 patients by positive cultures of cardiac material; the remaining patient had valve dehiscence 1 mo after the initial surgery without evidence of infection. All patients in whom 18F-FDG PET results were positive and endocarditis was excluded (n = 6) were imaged in the first 2 mo after cardiac surgery (median, 33 d; range, 14–47 d).
Among the 18 patients with negative 18F-FDG PET results, the final classification at 3 mo was no IE for 15, possible IE for 2, and definite IE for 1. Three patients with negative results underwent surgery, and PVE was excluded. The only patient with confirmed IE and negative 18F-FDG PET results was infected with Lactobacillus sp.
Performance of Leukocyte Scintigraphy
Among the 39 consecutive patients who underwent leukocyte scintigraphy, 9 (23%) were considered to have positive results. Sensitivity, specificity, positive predictive value, negative predictive value, and accuracy for the diagnosis of PVE were 64%, 100%, 100%, 81%, and 86%, respectively.
The 9 patients with positive results on leukocyte scintigraphy were classified as having definite IE. Among the 3 patients with positive results who underwent surgery, all were confirmed to have PVE and an abscess.
Among the 30 patients with negative results on leukocyte scintigraphy, the final classification at 3 mo was no IE for 21, possible IE for 4, and definite IE for 5. Six patients with negative results underwent surgery: PVE was excluded in 4 but was definite in 2. These 2 patients had PVE with nonpyogenic germs (Coxiella burnetti and Candida).
Comparison of 18F-FDG PET and Leukocyte Scintigraphy
The results of 18F-FDG PET and leukocyte scintigraphy were discrepant in 12 patients (31%). Of patients with definite IE, 5 had results that were true-positive on 18F-FDG PET but false-negative on leukocyte scintigraphy (Fig. 1). Of these 5 patients, 3 had IE with nonpyogenic microorganisms (Coxiella or Candida). The 2 remaining patients showed no signs of abscess on transesophageal echocardiography and had a favorable outcome under antibiotherapy. Of the patients in whom endocarditis had been excluded, 6 had results that were true-negative on leukocyte scintigraphy but false-positive on 18F-FDG PET (Fig. 2). These 6 patients had been imaged in the first 2 mo after the last cardiac surgery. When patients imaged in the first 2 mo after cardiac surgery (n = 9) were excluded from the analysis, sensitivity, specificity, positive predictive value, negative predictive value, and accuracy for the diagnosis of PVE were 57%, 100%, 100%, 67%, and 77%, respectively, for leukocyte scintigraphy and 92%, 100%, 100%, 93%, and 96%, respectively, for 18F-FDG PET. The last patient with a discrepancy between 18F-FDG PET and leukocyte scintigraphy was classified as having possible endocarditis and was positive on 18F-FDG PET and negative on leukocyte scintigraphy.

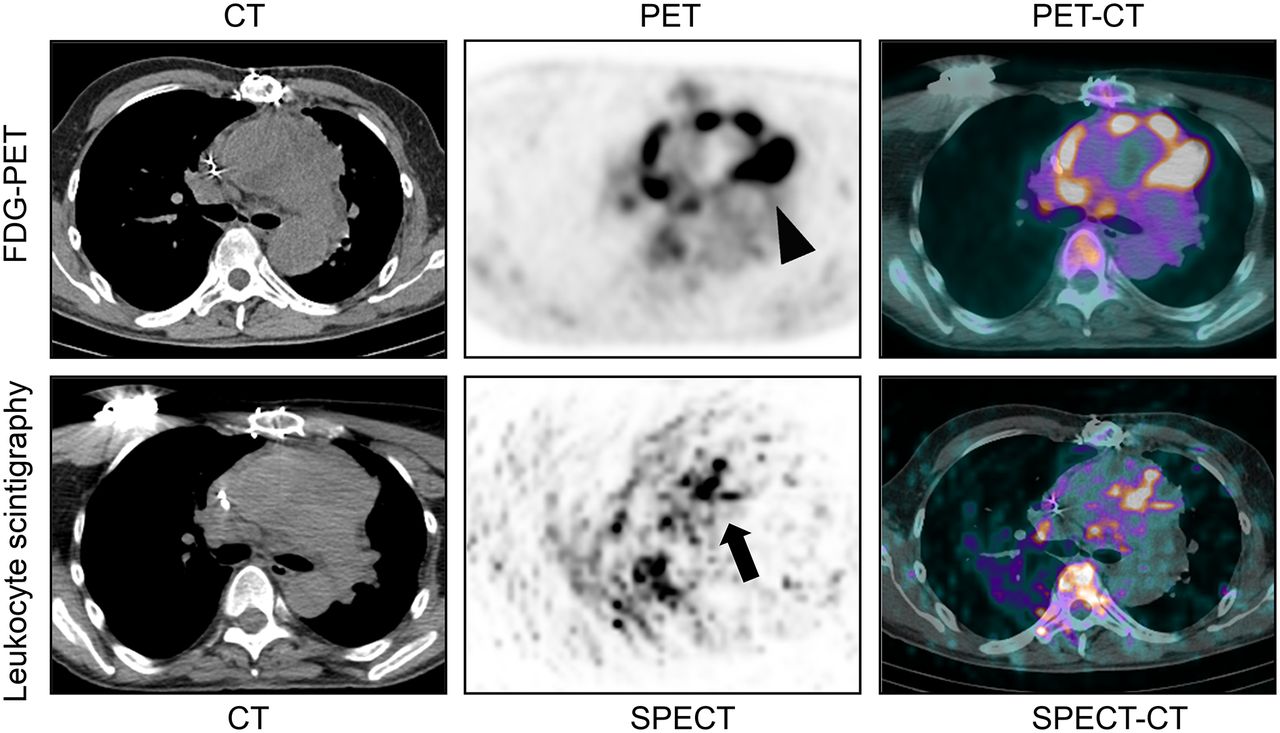
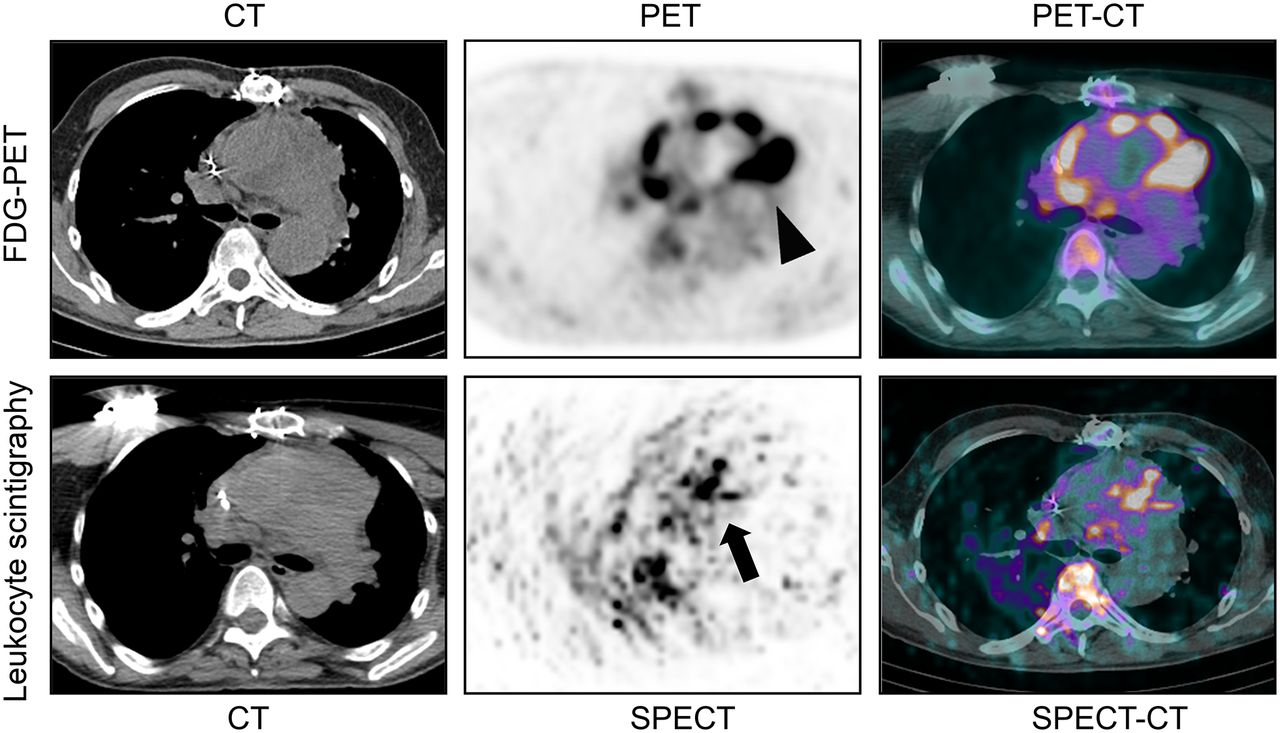
Representative example of patient with true-positive 18F-FDG PET findings and false-negative leukocyte scintigraphy findings. A 37-y-old woman was admitted for ischemic stroke. She had a history of rheumatoid valve disease with mitral valve replacement by mechanical prosthesis 1 y earlier. Transesophageal echocardiography revealed 10-mm-long mobile mass appended to mitral valve and new mild perivalvular mitral regurgitation. No criterion for endocarditis was present in blood cultures or serologies. Intense 18F-FDG uptake was detected on attenuation-corrected PET images (arrowhead) and in prosthetic mitral valve on axial PET/CT images. In same patient, no significant accumulation of radiolabeled leukocytes was detected in cardiac region on axial reconstructed SPECT images (arrow), in particular in the mitral valve area located using SPECT/CT. Patient underwent repeated surgery with excision of all material because of progression of partial valve dehiscence. Bacteriology of prosthetic valve confirmed active infection with Coxiella burneti.

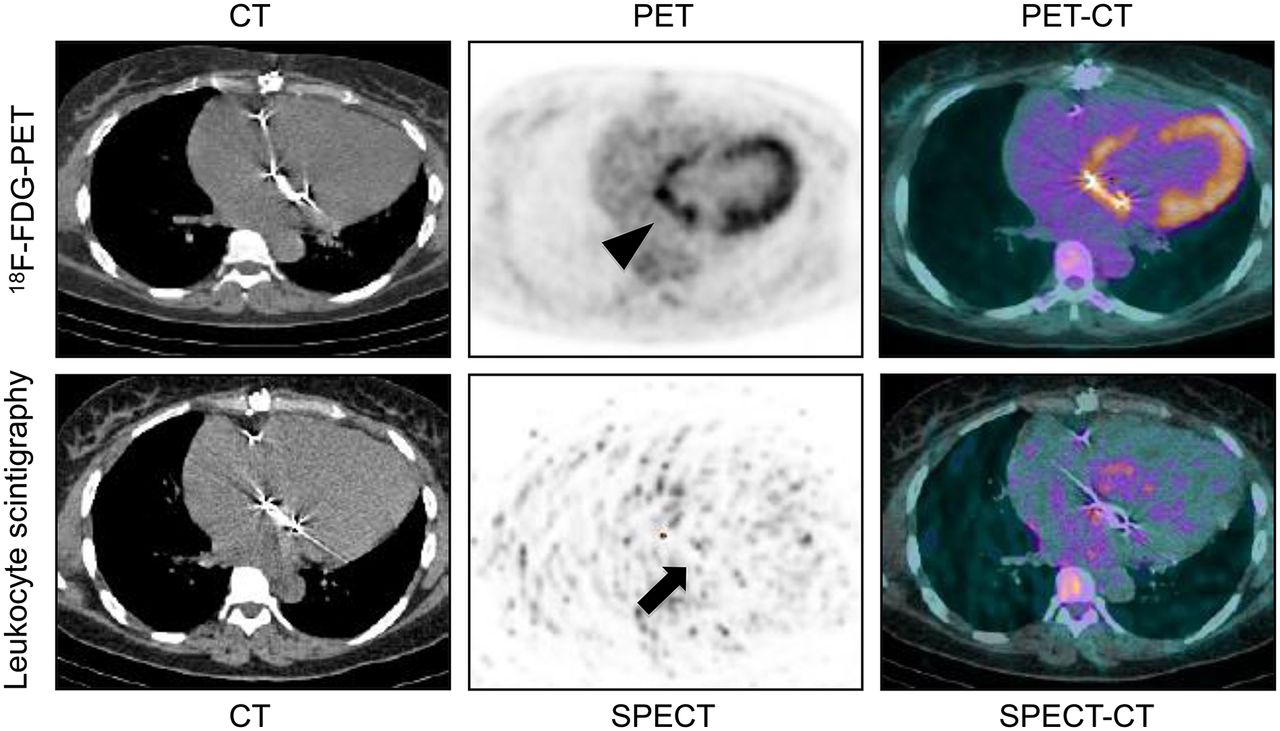
Representative example of patient with false-positive 18F-FDG PET findings and true-negative leukocyte scintigraphy findings. A 38-y-old woman was admitted after aortic valve replacement. She had a history of aortic valve replacement by mechanical prosthesis 2 y earlier. She developed acute endocarditis with blood cultures positive for Neisseria sicca and large vegetations and underwent urgent repeated surgery. Transesophageal echocardiography performed 40 d after intervention revealed presence of mild perivalvular regurgitation. No criterion for endocarditis was present in blood cultures under antibiotherapy. Moderate 18F-FDG uptake was detected on attenuation-corrected PET images (arrowhead) and around prosthetic aortic valve on axial PET/CT images. In same patient, no significant accumulation of radiolabeled leukocytes was detected in cardiac region on axial reconstructed SPECT images (arrow), in particular in the aortic valve area located using SPECT/CT. Patient remained asymptomatic and did not have any recurrent endocarditis 6 mo later.
Among patients classified with definite PVE caused by pyogenic germs, patients with positive leukocyte scintigraphy results had a nonstatistically significant higher 18F-FDG uptake in the valvular area (Fig. 3) than did patients with negative leukocyte scintigraphy results (SUVmean, 7.1 [range, 4.1–14.7] vs. 5.9 [range, 4.0–9.3]; prosthetic-valve–to–background ratio, 4.7 [range, 2.4 −7.8] vs. 2.9 [range, 2.3–4.1], P = 0.21 and 0.17, respectively).
Representative example of patient with true-positive 18F-FDG PET findings and true-positive leukocyte scintigraphy findings. A 60-y-old man was admitted for fever associated with Staphylococcus aureus septicemia. He had a history of aortic aneurysm of ascending thoracic aorta treated 2 y earlier by aortic valve replacement with biologic prosthesis and replacement of ascending aorta. Transesophageal echocardiography did not show any criteria for endocarditis. Intense 18F-FDG uptake was detected on attenuation-corrected PET images (arrowhead) and around aortic tube on axial PET/CT images. In same patient, diffuse accumulation of radiolabeled leukocytes was detected on axial reconstructed SPECT images (arrow) and along aortic tube on SPECT/CT images, corresponding to area identified on 18F-FDG PET images. On basis of results of both types of scintigraphy, patient underwent repeated surgery with excision of all material. Intraoperative analysis confirmed presence of pus around aortic tube, and valve culture was positive for Staphylococcus aureus.
The performance of an imaging strategy consisting of performing leukocyte scintigraphy in patients with positive 18F-FDG PET results in the first 2 mo after cardiac surgery was evaluated in this cohort of patients. Sensitivity, specificity, positive predictive value, negative predictive value, and accuracy for the diagnosis of PVE based on this imaging strategy were 93%, 100%, 100%, 95%, and 97%, respectively. After 18F-FDG PET and leukocyte scintigraphy, 18 patients (46%) were correctly reclassified in the modified Duke–Li classification (Table 3).
Impact of 18F-FDG-PET and Leukocyte Scintigraphy on Classification of Patients with Modified Duke–Li Classification
DISCUSSION
In the present study, the performance of 18F-FDG PET and leukocyte scintigraphy for the diagnosis of PVE was evaluated in patients who underwent the 2 imaging modalities for clinical indications. This study confirmed the high sensitivity of 18F-FDG PET for the diagnosis of endocarditis in patients with suspected PVE. False-positive 18F-FDG PET results were, however, identified in the first 2 mo after open-chest cardiac surgery, probably as a consequence of inflammatory reactions taking place in the early stages after implantation of foreign material. In comparison to 18F-FDG PET, leukocyte scintigraphy demonstrated lower sensitivity but higher specificity for the detection of PVE. This imaging technique therefore seems particularly interesting for evaluating patients with suspected PVE in the first 2 mo after cardiac surgery or in cases of inconclusive 18F-FDG PET results.
Performance of 18F-FDG PET Imaging for Detection of PVE
18F-FDG PET imaging presents several advantages for the evaluation of patients with suspected PVE. First, PET acquisitions are performed only 1 h after the injection of 18F-FDG. This translates into high activities in tissues, good image quality, and short acquisition times. Second, 18F-FDG PET has become widely available. Third, whole-body 18F-FDG PET acquisitions can help to identify the origin of the infection and the presence of septic emboli. However, 18F-FDG PET presents certain limitations for the evaluation of patients with suspected PVE. The presence of intense myocardial uptake can hamper analysis of the contours of a valvular prosthesis, particularly in the mitral position. In the current study, suppression of physiologic 18F-FDG uptake was obtained by 12 h of fasting and preparation with a low-carbohydrate, high-fat meal before imaging. Myocardial 18F-FDG uptake was classified as low or mild in 75% of the patients using this protocol and did not represent an important limitation for the PET evaluation of cardiac valves. Furthermore, 18F-FDG uptake is often present in noninfected grafts or material wherein chronic aseptic inflammation is taking place and can be difficult to discriminate from an infectious process (12). In this study, 18F-FDG uptake caused by inflammatory reactions in prostheses represented an important issue especially in patients imaged in the first 2 mo after open-chest cardiac surgery, because the intensity of the radiotracer uptake in inflammatory tissues during this period can be high and similar to that in infected tissues. Later after the surgery, the intensity of inflammation around prostheses tends to decrease and can therefore be more easily discriminated from infective processes.
Performance of Leukocyte Scintigraphy for Detection of PVE
In previous work (8,9), leukocyte scintigraphy demonstrated an excellent specificity for the detection of perivalvular infection and abscesses in patients with suspected PVE. In addition, the intensity of perivalvular radiolabeled leukocyte accumulation on scintigraphy allows for the evaluation of local and extended infectious activity and therefore represents an interesting prognostic marker in patients with PVE (8). However, leukocyte scintigraphy has some important limitations for the evaluation of patients with suspected PVE. First, radiolabeling of leukocytes involves direct handling of blood products. Second, leukocyte scintigraphy, as compared with 18F-FDG PET, offers a lower sensitivity for the detection of PVE, which can be explained by several factors: the spatial resolution and sensitivity are intrinsically lower in single-photon γ cameras than in PET systems; the signal detected with leukocyte scintigraphy is weak because acquisitions are performed 24 h after injection of 99mTc-radiolabeled leukocytes; accumulation of leukocytes is high in active abscesses but weak in vegetations or drained abscesses; and only granulocytes were radiolabeled for leukocyte scintigraphy in the present study. Patients with Q fever or Candida endocarditis show, on histologic examination, an infiltration consisting mostly of lymphocytes and monocytes in the cardiac valves (13,14), possibly explaining why leukocyte scintigraphy was falsely negative in the 3 patients with nonpyogenic germs (2 patients infected with Coxiella burnetii and 1 patient with Candida).
Imaging Strategy in Patients with Suspected PVE and Inconclusive Echocardiography Results
Because of its high sensitivity, 18F-FDG PET is well suited as the first-line imaging technique in patients with suspected PVE and inconclusive echocardiography results. In patients with negative 18F-FDG PET results, the probability of PVE is low. In patients showing intense 18F-FDG uptake in the cardiac valves on PET (prosthetic-valve–to–background ratio > 4.4 in this study), the probability of infection is high. In the presence of mild, diffuse 18F-FDG uptake around cardiac prostheses, the diagnosis of infection can be difficult, particularly in patients imaged early after cardiac surgery. In these cases, leukocyte scintigraphy seems to represent a useful imaging technique to discriminate between infective and inflammatory processes in the cardiac valves. Indeed, the specificity for the identification of PVE increased in this study from 71% when only 18F-FDG PET imaging was considered to 100% when a combination of the 2 imaging techniques was used. Even though this point was not evaluated in the current study, in our experience PET images can also be useful for the analysis of leukocyte scintigraphy: identification of regions with high 18F-FDG uptake on PET helped to localize the cardiac areas that should be evaluated on corresponding leukocyte scintigraphy images.
Limitations of the Study
This study had some limitations. First, the study was monocentric, and the diagnostic performance of leukocyte scintigraphy and 18F-FDG PET was measured using physicians trained to evaluate PVE with scintigraphy. In our experience, integrating clinical history with echocardiography and scintigraphy results is the key to improving the accuracy of these imaging techniques. Second, patients evaluated in this study represented only a selection presenting with suspected PVE. Only patients who benefited from both 18F-FDG PET imaging and leukocyte scintigraphy for clinical indications were included in this study. The diagnostic performance of each imaging modality in this study was, however, similar to previous findings (6,9), except for the sensitivity of radiolabeled leukocyte scintigraphy for the diagnosis of endocarditis, which was lower in this study (64%) than in the study of Erba et al. (90%) (9). 18F-FDG PET was performed on all patients in this study and has been shown to dramatically improve sensitivity for the diagnosis of PVE (6). The fact that additional patients were diagnosed with PVE because of 18F-FDG PET imaging could explain the lower sensitivity of leukocyte scintigraphy in this study. Third, the presence of PVE in patients with positive 18F-FDG PET results in the first 2 mo after cardiac surgery cannot be formally excluded on the basis of the modified Duke–Li probability score. Early PVE is, however, often associated with poor outcome. The good clinical evolution of these 6 patients during follow-up represents an additional clue against the presence of infection. Finally, the performance of a sequential strategy consisting of 18F-FDG PET as first-line imaging and leukocyte scintigraphy as second-line imaging for the diagnosis of PVE has been extracted from a relatively small, selected group of patients. This approach, though promising, needs to be validated prospectively in a larger group of patients with suspected PVE.
CONCLUSION
In summary, 18F-FDG PET offers high sensitivity for the detection of active infection in patients with suspected PVE and inconclusive echocardiography findings and represents a useful first-line imaging technique in this situation. Leukocyte scintigraphy, however, offers higher specificity than 18F-FDG PET for the diagnosis of PVE. In this study, a sequential strategy consisting of performing 18F-FDG PET imaging initially and following it with leukocyte scintigraphy when the former was inconclusive or when patients had positive 18F-FDG PET results in the first 2 mo after cardiac surgery strongly improved the diagnosis of PVE. The validity of this imaging strategy in patients with suspected PVE will need to be confirmed in a prospective clinical study with a larger number of patients.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Nov. 11, 2014.
- © 2014 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication April 21, 2014.
- Accepted for publication September 11, 2014.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Imaging Inflammation Past, Present, and Future: Focus on Cardioimmunology
- Hot Spot Imaging in Cardiovascular Diseases: An Information Statement from SNMMI, ASNC, and EANM
- Nuclear Imaging of Bacterial Infection: The State of the Art and Future Directions
- Molecular Imaging of Cardiovascular Device Infection: Targeting the Bacteria or the Host-Pathogen Immune Response?
- Prognostic Value of 18F-Fluorodeoxyglucose Positron Emission Tomography/Computed Tomography in Infective Endocarditis
- A New Match Between Surgery and Transcatheter Aortic Valve Replacement: Fear the Endocarditis
- Methicillin-Resistant Staphylococcus aureus Prosthetic Valve Endocarditis: Pathophysiology, Epidemiology, Clinical Presentation, Diagnosis, and Management
- Merits of FDG PET/CT and Functional Molecular Imaging Over Anatomic Imaging With Echocardiography and CT Angiography for the Diagnosis of Cardiac Device Infections
- Molecular Imaging of Myocardial Inflammation With Positron Emission Tomography Post-Ischemia: A Determinant of Subsequent Remodeling or Recovery
- Targeting Cardiovascular Implant Infection: Multimodality and Molecular Imaging
- Metabolic Imaging of Infection
- 18F-Fluorodeoxyglucose Positron Emission Tomography-Computed Tomography in Cardiac Implantable Electronic Devices Infection: Ready for Routine Care!
- Characterization of 18F-Fluorodeoxyglucose Uptake Pattern in Noninfected Prosthetic Heart Valves
- 18F-Fluorodeoxyglucose Imaging of Inflammation: Ready to Represent a Standard in Diagnosing Endocarditis?
- Challenges in Infective Endocarditis
- New diagnostic approaches in infective endocarditis
- Diagnosing pulmonic valve infective endocarditis with positron emission tomography-CT
- Improving the Diagnosis of Infective Endocarditis in Prosthetic Valves and Intracardiac Devices With 18F-Fluordeoxyglucose Positron Emission Tomography/Computed Tomography Angiography: Initial Results at an Infective Endocarditis Referral Center
- Positron Emission Tomography/Computed Tomography Imaging in Device Infective Endocarditis: Ready for Prime Time
- Critical Questions About Left-Sided Infective Endocarditis
- Detection of Mycotic Aneurysms of Lower Limbs by Whole-Body 18F-FDG-PET