


Abstract
Currently, there is no consensus on the use of 90Y radioembolization for salvage patients with colorectal cancer liver metastases. The purpose of this study was to provide a comprehensive overview of the available data on tumor response and survival after 90Y radioembolization for this group of patients. Methods: A systematic literature search was conducted in PubMed (Medline), Excerpta Medica (EMBASE), and the Cochrane Library (September 2012) with synonyms for “radioembolization” and “colorectal cancer liver metastases.” Results were described separately for patient cohorts treated with 90Y radioembolization as monotherapy and with 90Y radioembolization in combination with chemotherapy. Results: The search yielded 13 relevant articles for systematic review on 90Y radioembolization as monotherapy and 13 relevant articles on 90Y radioembolization combined with chemotherapy. Disease control rates (i.e., complete response, partial response, and stable disease) ranged from 29% to 90% for 90Y radioembolization as monotherapy and from 59% to 100% for 90Y radioembolization combined with chemotherapy. Heterogeneity in the data prohibited pooling of response rates. Survival proportions at 12 mo ranged from 37% to 59% for 90Y radioembolization as monotherapy and from 43% to 74% for 90Y radioembolization combined with chemotherapy. Conclusion: In the studies included in this systematic review, approximately 50% of salvage patients with colorectal cancer liver metastases survive more than 12 mo after treatment with 90Y radioembolization, either as monotherapy or in combination with chemotherapy. Heterogeneity between studies has unfortunately prohibited pooling of data. Future research will discern the precise role of 90Y radioembolization in general clinical practice in comparison with chemotherapy.
Colorectal cancer is the third most commonly diagnosed type of cancer worldwide in men and the second in women, with the highest incidence rates in the Western world. It is also the third most common cause of cancer death (1). Approximately 50% of patients present with metastases to the liver either at diagnosis or during follow-up, and liver metastases account for a large proportion of morbidity and mortality in patients.
A small proportion of patients with colorectal cancer liver metastases (CRCLM) has a chance of long-term survival through surgical resection (2). Patients with unresectable lesions are treated with systemic chemotherapy. Currently, several effective systemic treatment lines are available. Chemotherapeutic agents include fluoropyrimidine, irinotecan, and oxaliplatin, which can be used sequentially or as combination therapy (i.e., FOLFOX [folinic acid, fluorouracil, and oxaliplatin] or FOLFIRI [folinic acid, fluorouracil, and irinotecan hydrochloride]). Furthermore, monoclonal antibodies have been developed (bevacizumab, cetuximab, and panitumumab) that can be administered as monotherapy or in combination with chemotherapy (3–5). However, some patients do not respond to the currently available systemic treatments or need to stop because of severe comorbidities, and more therapeutic options are warranted.
Over the past decade, image-guided catheter-based or intraarterial techniques have emerged for locoregional treatment of the entire liver. The rationale for intraarterial treatment of liver tumors is that malignant intrahepatic lesions derive their blood supply almost entirely from the hepatic artery (99%), as opposed to healthy liver tissue, which depends mainly on the portal vein for its blood supply (80% portal vein and 20% hepatic artery). Thus, agents that are delivered intraarterially to the liver are preferentially directed to malignant tissue, resulting in local tumor control and fewer systemic side effects, compared with agents that are administered systemically (2). Different types of intraarterial treatments can be distinguished, such as transarterial or bland embolization, transarterial chemoembolization, and intraarterial radioembolization (2,6). Intraarterial radioembolization with 90Y microspheres (90Y radioembolization) is a technique for treatment of patients with unresectable primary or secondary liver tumors, of which metastatic colorectal cancer is a large group (6–8). Microspheres with a diameter of 30–40 μm are embedded with the radioisotope 90Y, delivered to the liver via a catheter in the hepatic artery, and lodge at the arteriolar level inside the tumors, where a high dose of β radiation will be delivered with a mean tissue penetration depth of 2.5 mm.
Currently, although many researchers have studied radioembolization in the salvage setting for CRCLM patients, there is no consensus on the exact role of 90Y radioembolization in this patient population. Questions still remain on precisely which patients should be considered for treatment and whether concomitant chemotherapy should be used. In this paper, we present a comprehensive overview of published studies and discuss reported outcomes of radioembolization for CRCLM.
MATERIALS AND METHODS
Search Strategy and Study Selection
This systematic review was conducted according to the PRISMA guidelines (Preferred Reporting Items of Systematic Reviews and Meta-Analyses). A literature search was performed in PubMed (Medline), Excerpta Medica (EMBASE), and the Cochrane Library from December 2001 to September 2012. The search was limited to articles published after December 2001, because by that time, radioembolization treatment was standardized and the first larger trial had been published. An extensive search query was created with several synonyms for “colorectal cancer,” “liver metastases,” and “yttrium-90 radioembolization” and adapted for the various databases (complete search syntax is available as supplemental material at http://jnm.snmjournals.org). No limits were used. Additional publications were retrieved by cross-referencing.
After this search, 3 independent readers selected publications that were considered relevant on the basis of titles or abstracts. An overview of inclusion and exclusion criteria for study selection is presented in Table 1. Publications regarding fewer than 10 patients were termed case series and excluded. Conference abstracts without full-text publications were excluded. In a second selection round, full-text articles selected on the basis of titles and abstracts were reviewed in more detail. Consensus on study selection was reached in a group discussion.
Inclusion and Exclusion Criteria for Article Selection
Data Extraction and Critical Appraisal
The following data were extracted from the selected articles: study design, treatment details (i.e., either 90Y radioembolization as monotherapy or 90Y radioembolization in combination with chemotherapy, type of microspheres and administered activity, criterion for eligibility of liver disease), patient characteristics (i.e., number and age of patients, status of liver and extrahepatic disease, hepatic function, previous systemic therapies, performance score), and outcome measures (i.e., tumor response and survival). The choice of extracted patient characteristics was based on previously published data on prognostic factors for response and survival of patients (9–12). For randomized controlled trials or nonrandomized comparative studies, only the data of patients treated with 90Y radioembolization were extracted. In mixed cohorts (i.e., comprising patients with various tumor types), only data for patients with CRCLM were extracted. Data are presented separately for 90Y radioembolization as monotherapy and 90Y radioembolization combined with chemotherapy.
Quality of the included publications was assessed using a list of items taken from the STROBE statement (Strengthening the Reporting of Observational Studies in Epidemiology) (13). The selected items were deemed important for reporting on patient population and tumor response and for assessing comparability between studies. This critical appraisal attempts not to question the validity or reliability of the actual data content within the studies but to evaluate the method and extent of available data reporting and presentation.
Statistical Methods
To present comprehensibly comparable data, survival proportions at 12 mo after treatment were computed for all included studies reporting overall survival. These proportions were either determined from the Kaplan–Meier graph if present or estimated with a negative exponential survival distribution and the reported median overall survival. This latter is done by assuming that survival at time t is given by  , where λ can be found by inserting the median overall survival (
, where λ can be found by inserting the median overall survival ( ) and calculating
) and calculating  . With this λ, one can calculate the corresponding survival proportion at t = 12 mo (14).
. With this λ, one can calculate the corresponding survival proportion at t = 12 mo (14).
RESULTS
Study Description and Critical Appraisal
The systematic search yielded 246 potentially relevant studies (Fig. 1). Using inclusion and exclusion criteria, consensus was reached that 107 articles were to be assessed in full text. Subsequently, 81 studies were excluded from the analysis, leaving 26 publications with relevant information on tumor response and survival of patients treated with 90Y radioembolization for CRCLM. Cross-referencing did not yield any additional relevant articles.
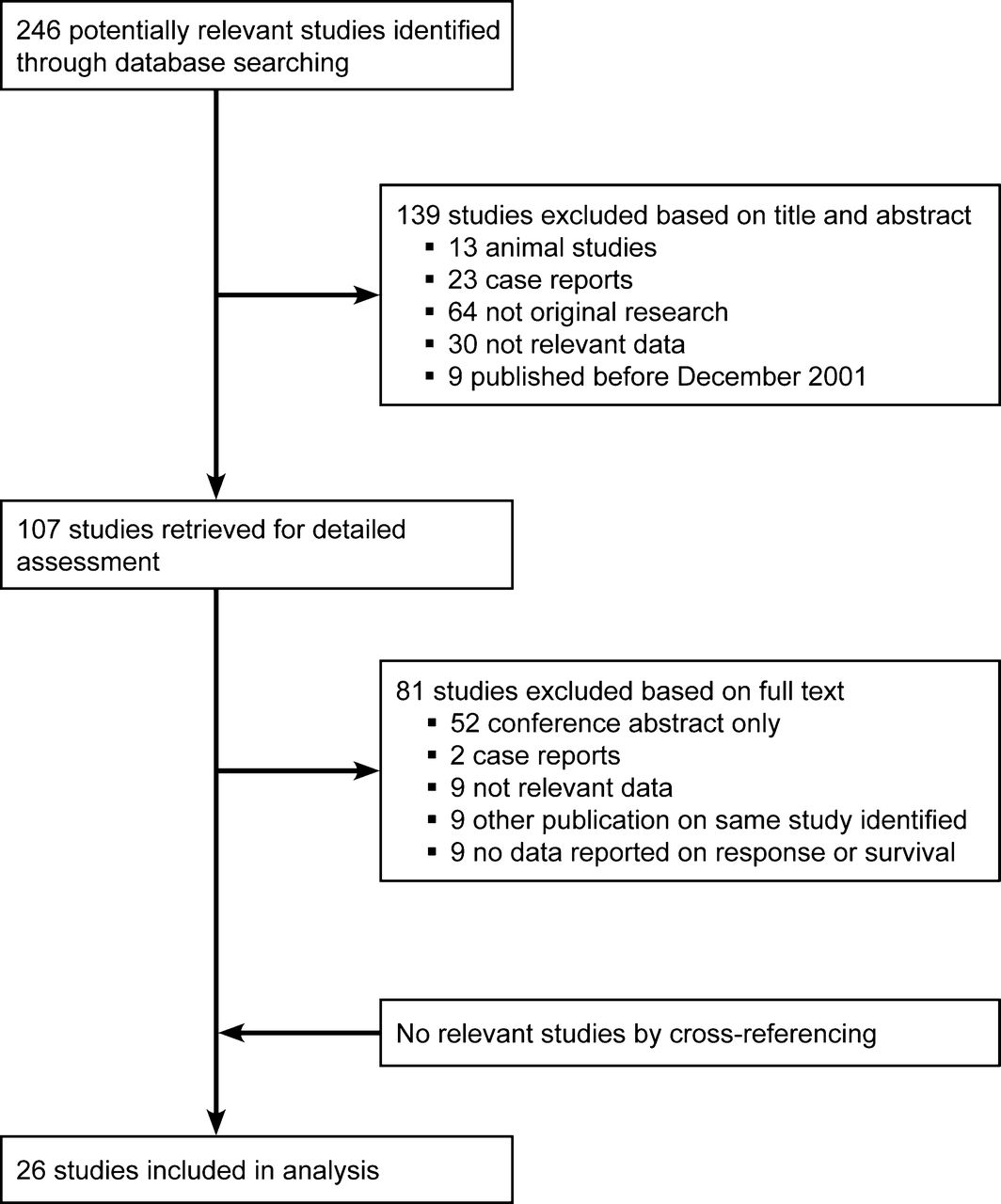
Flowchart depicting selection of relevant publications.
Among the selected studies reporting on 90Y radioembolization as monotherapy were 3 phase 2 trials (7,15,16), 2 prospective cohort studies (12,17), and 8 retrospective cohort studies (9,18–24), involving a total of 901 patients (Supplemental Table 1). All studies had included patients with unresectable and chemorefractory liver lesions (i.e., salvage patients), and most studies included patients with liver-dominant disease, that is, the studies accepted patients with minor extrahepatic disease for treatment. Reported proportions of included patients with extrahepatic disease ranged from 10% to 78%.
Among the studies reporting on 90Y radioembolization treatment in combination with chemotherapy (either systemic or intrahepatic) were 3 randomized controlled trials (25–27), 2 phase 1 trials (28,29), 2 prospective studies (10,30), and 5 retrospective studies (31–35) (Supplemental Table 2). One study design was not unequivocally defined (36). The total number of included patients was 472. Large variation existed in administered chemotherapeutic agents between the studies, such as floxuridine, fluorouracil/leucovorin, FOLFOX, and irinotecan. Furthermore, 3 studies have used intrahepatic infusion of the chemotherapeutic agent as opposed to systemic administration.
The results of the critical appraisal show that incompleteness of data reporting is relatively common (Supplemental Table 3). Furthermore, heterogeneity in response assessment with respect to incorporation of extrahepatic lesions becomes apparent.
Tumor Response
For 90Y radioembolization as monotherapy, tumor response rates were reported in 10 studies with a total of 545 patients. Response rates (defined as complete response and partial response) ranged from 18% to 46%. Disease control rates (i.e., complete response, partial response, and stable disease) ranged from 29% to 90%. Progression-free survival was reported in 6 studies and ranged from 3.9 to 9.2 mo.
For 90Y radioembolization treatment combined with chemotherapy, responses were reported in 11 studies with a total of 388 patients. Response rates ranged from 8% to 90%. Disease control rates ranged from 59% to 100%.
Critical appraisal showed large heterogeneity in (reporting on) response assessment (Supplemental Table 3). Therefore, we decided not to calculate a pooled estimate for response rates.
Survival Statistics
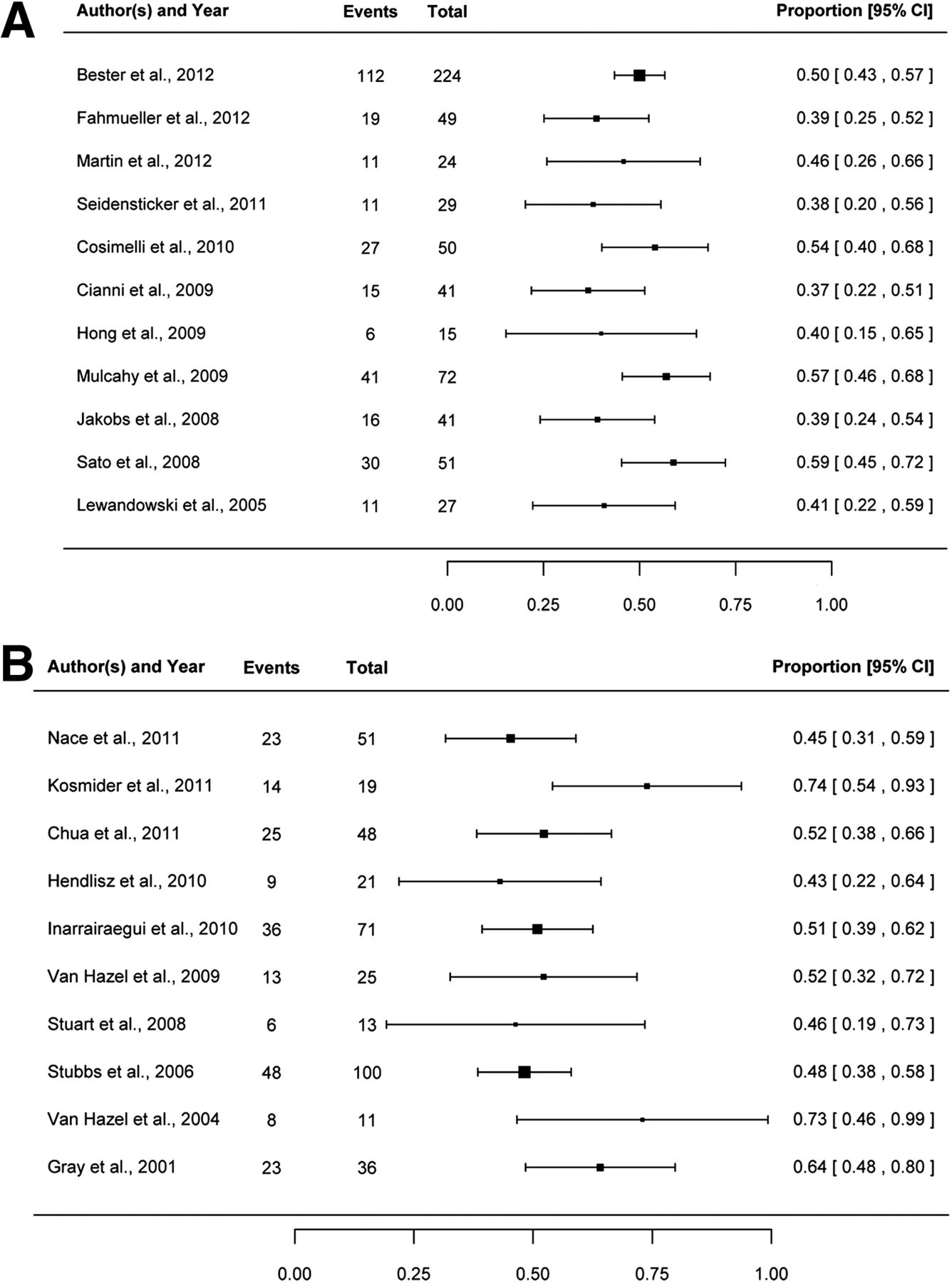
For 90Y radioembolization as monotherapy, overall survival was reported in 12 studies. However, Kennedy et al. (23) reported only survival data for responders and nonresponders separately, whereas the other papers stated the survival for the entire cohort of CRCLM patients, which ranged from 8.3 to 15.2 mo (Supplemental Table 1). Survival proportions at 12 mo after treatment ranged from 37% to 59% (Fig. 2A).

Survival proportions at 12 mo after treatment for studies on 90Y radioembolization as monotherapy (A) and 90Y radioembolization in combination with chemotherapy (B).
For 90Y radioembolization in combination with chemotherapy, overall survival was reported in 10 studies and ranged from 10.0 to 29.4 mo (Supplemental Table 2). Survival proportions at 12 mo after treatment ranged from 43% to 74% (Fig. 2B).
DISCUSSION
From the studies included in this systematic review, survival proportions of approximately 50% at 12 mo after treatment were found. Therefore, in this group of salvage CRCLM patients, who otherwise have no regular treatment options and a life expectancy of less than 6 mo, 90Y radioembolization seems to be a hopeful treatment option (3,4).
90Y radioembolization is an emerging treatment for CRCLM and is performed as monotherapy or with concomitant chemotherapy. Over the past few decades, multiple phase 1 and 2 trials, randomized clinical trials, cohort studies, and several reviews have been published on 90Y radioembolization. However, the reviews focused mainly on technical details concerning the angiographic procedures, did not focus primarily on liver metastases of colorectal cancer, or assessed only a selection of the available evidence (6,8,37,38). In the present systematic review, we aimed to provide a comprehensive overview of all currently available data on tumor response and survival after 90Y radioembolization for salvage patients with CRCLM.
To evaluate treatment outcome based on multiple studies, comparability of studies and patient populations is needed. International guidelines have stated widely accepted inclusion and exclusion criteria for treatment with 90Y radioembolization (39). These guidelines do, however, leave substantial room for subjectivity due to several poorly defined or relative contraindications (such as the amount of extrahepatic disease). Any relative contraindications must be evaluated per individual patient, leading to large inter- and intrainstitute variability in patient selection. Recently, Salem et al. published a paper focusing on research-reporting standards in the field of radioembolization (40). This paper encourages researchers to use standardized terminology in order to facilitate comparability between studies and correspondence between authors. During the selection process and data extraction for this systematic review, large heterogeneity in inclusion criteria and in patient populations and response assessment methods became apparent. This problem is also reflected in the critical appraisal (Supplemental Table 3).
Heterogeneity in patient populations arises in several aspects. First, heterogeneity in the definition of tolerable amount of extrahepatic disease for treatment exists. A widely accepted selection criterion for 90Y radioembolization is the presence of unresectable, liver-dominant tumors. However, no consensus on the definition of liver dominance and acceptable tumor load outside the liver is currently available from the literature, even though the presence of extrahepatic disease has been shown to influence treatment outcome and survival (10,12,30,32,36). Nevertheless, sometimes details on the criterion for liver-dominant disease cannot be extracted from articles or only the rather general comment is made that “patients with extrahepatic disease not deemed clinically relevant were accepted for treatment.” Yet in 3 articles on 90Y radioembolization as monotherapy and 4 on combination treatment with chemotherapy, the applied definition of liver-dominant disease was specified, either in terms of number (10,15), amount (size or percentage) (31), or localization of acceptable extrahepatic lesions (18,27,32). Hendlisz et al. did not accept any extrahepatic disease (i.e., treated disease limited to the liver only) (25), and Seidensticker et al. accepted patients with nonprogressive extrahepatic deposits for treatment (9).
Second, acceptable intrahepatic tumor burden is generally advised to be no more than 70% of the liver. Previous studies have confirmed the prognostic value of liver involvement for treatment outcome (12,16). Of the articles in this review, some have included only patients with a tumor burden of less than 50% (9,15), whereas others have accepted larger liver involvements. For example, one quarter of patients described in the study by Cianni et al. had more than 50% liver involvement (20).
Third, patient performance status has also been demonstrated to have prognostic value for the outcome of 90Y radioembolization (12,30). Only half the articles that qualified for inclusion in this review reported patient performance scores. Most studies included mainly patients with a World Health Organization performance score of 0. However, in the study by Stubbs et al., for example, 50% of patients had a performance score greater than 0 (36).
Last, the prognostic value of previous systemic treatments has not been the focus of much research until now, although some studies indicate influence of prior therapies and response to prior therapies on current treatment outcome (18). However, knowledge of previous systemic treatments of included patients is important. On one hand, heavily pretreated patients generally have more advanced disease and will possibly benefit less from 90Y radioembolization treatment. On the other hand, patients who have not yet received all standard available systemic treatment regimes may do so after 90Y radioembolization, thereby obscuring the survival benefit of 90Y radioembolization. To be able to compare studies, information on specific chemotherapeutic agents and number of treatments is needed. However, definitions for “a line” of chemotherapy may vary across institutions. Critical appraisal of reported previous systemic treatments (Supplemental Table 3) showed that approximately half the studies did not report, or only incompletely reported, previous systemic treatments.
Most studies on 90Y radioembolization as monotherapy in this review have treated patients who had received a median of 3 or more previous systemic treatments. Mulcahy et al. treated a relatively large number of patients who received two or fewer lines of previous systemic therapy (12). For the studies on 90Y radioembolization in combination with chemotherapy, previous treatments of patients were obviously related to the study inclusion criterion with respect to the concomitant treatment (Supplemental Table 2).
Besides heterogeneity in patient populations, heterogeneity in response assessment also exists between selected studies for this review. Imaging response to treatment is almost always scored with RECIST (Response Evaluation Criteria in Solid Tumors) or World Health Organization criteria. However, not always can the precise use of these criteria (with respect to application to the liver only, target lesions only, or whole body) be deduced from the article, even though this determination is of pivotal importance for the interpretation of treatment results. Some authors do state explicitly that, for example, criteria are used only for hepatic lesions and do not take extrahepatic disease into account (7,16,25).
Second, for accurate interpretation of reported tumor responses, information on other parameters of response assessment is crucial. These include interval between follow-up scans, total duration of follow-up, and interval for reported response. An often-used interval for determining response is at 3 mo after treatment (16,22,23,29,31,36), although earlier outcome assessments have also been described (15,20,30). Some authors report patient’s best response (12,25–27,32), and especially in these cases, total follow-up duration is of interest. Without information on sampling interval and follow-up duration, comparison of responses between studies becomes complicated. In addition, number of patients lost to follow-up is important, including a statement on the handling of this parameter (e.g., calculating worst-case scenario by considering patients lost to follow-up as having progressive disease) (17).
Because of the heterogeneity in response assessment, we did not find it helpful to calculate a pooled estimate for the response rate. There may even be a need for new response criteria specifically designed for locoregional therapies, in which some tumors either are not treated simultaneously or are not treated at all, when considering extrahepatic disease localizations.
Given the heterogeneities in patient populations and reporting of results, pooling of data was not appropriate and only descriptive comparisons can be made. With respect to tumor responses for 90Y radioembolization as monotherapy, the lowest response rate was reported by Fahmueller et al. (disease control rate of 29%) (17), and the highest response rate was reported by Kennedy et al. (disease control rate of 90%) (23). Response was measured with PET/CT in the former study and with CT and RECIST criteria in the latter, potentially explaining in part the differences in response. For 90Y radioembolization in combination with chemotherapy, the lowest response rate was reported by Lim et al. (disease control rate of 59%) (30), and the highest response rates were reported by Van Hazel et al. and Sharma et al. (26,29) (both had a disease control rate of 100%). However, these last 2 studies are relatively small (11 and 20 patients, respectively). The largest study is by Stubbs et al. (36), with 100 included patients and measuring disease control rate at 3 mo. However, a rather large proportion of patients was lost to follow-up at that moment (20/100 patients). Thus, disease control was confirmed at the 3-mo follow-up in only 75 of 100 patients. Furthermore, response and progression in this study were respectively defined as decrease and increase of lesion size, without the specific percentages as are used in RECIST.
When survival data were compared for 90Y radioembolization as monotherapy, the shortest overall survival was reported by Seidensticker et al. (8.3 mo) (9) and the longest overall survival was reported by Sato et al. (15.2 mo) (7). Comparison of these 2 studies is difficult. One used resin-based spheres and the other glass-based spheres of which the median administered activity was not reported. Seidensticker et al. included a relatively large percentage of patients with extrahepatic disease. Unfortunately, details on this cannot be extracted from the other paper. For 90Y radioembolization in combination with chemotherapy, the shortest overall survival was reported by Hendlisz et al. (10.0 mo) (25) and the longest overall survival was reported by Van Hazel et al. and Kosmider et al. (both 29.4 mo) (26,32). Reasons for these differences are not readily apparent, other than the fact that these were all relatively small studies (21, 11, and 19 patients, respectively). The largest cohort in this group of articles is by Stubbs et al., with 100 patients, reporting an overall survival of 11 mo (36).
To enable comparison of the survival statistics of the individual studies, survival proportions at 12 mo after treatment were determined, either through measurements from a Kaplan–Meier plot or through calculations presuming exponential survival distributions. In our opinion, survival at 12 mo is clinically valuable information in the described patient populations. Because most median survivals were close to 12 mo, we also feel that any errors due to the assumption of exponential decay are small.
At present, 90Y radioembolization is provided mainly to patients with progressive disease after first-line (fluoropyrimidine-based) and second-line (irinotecan-based) chemotherapy. Possible third-line systemic treatment consists of monoclonal antibodies (i.e., panitumumab or cetuximab). Van Cutsem et al. conducted a randomized controlled trial for panitumumab versus best supportive care and reported an overall survival for both groups of approximately 6 mo (3). In a randomized controlled trial on cetuximab versus best supportive care, Jonker et al. demonstrated that cetuximab significantly improved overall survival compared with best supportive care alone (6.1 vs. 4.6 mo, respectively) (4). Included patients in these studies were similar to those deemed eligible for 90Y radioembolization, withstanding their potential extrahepatic disease load, since treatment with monoclonal antibodies is systemic. With that in mind, the results of this review show that, in the appropriately selected patient (with liver-dominant disease, acceptable disease burden, and preserved hepatic function and performance status), longer overall survival can be expected after 90Y radioembolization than with current third-line systemic treatment options.
CONCLUSION
In this review we showed that approximately 50% of salvage patients with CRCLM survive more than 12 mo after treatment with 90Y radioembolization. Paucity of data and heterogeneity between studies in the published literature have unfortunately made it difficult to perform a metaanalysis. In future studies, parameters on characteristics of included patients, treatment, safety and follow-up should clearly be documented and reported, enabling more thorough comparison and pooling of treatment outcomes. Furthermore, there is an urgent need for more high-quality randomized comparisons. Currently, 3 randomized controlled trials are recruiting, comparing either first-line chemotherapy (SIRFLOX [FOLFOX Plus SIR-Spheres Microspheres Versus FOLFOX Alone in Patients with Liver Mets from Primary Colorectal Cancer] and FOXFIRE [FOLFOX6m Plus SIRSpheres Microspheres vs FOLFOX6m Alone in Patients with Liver Mets from Primary Colorectal Cancer]) or second-line chemotherapy (EPOCH [Efficacy Evaluation of TheraSphere Following Failed First Line Chemotherapy in Metastatic Colorectal Cancer]) alone with combination treatment with radioembolization. These results have to be awaited to determine the exact place of 90Y radioembolization in general clinical practice in comparison with chemotherapy for patients with CRCLM.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Sep. 26, 2013.
- © 2013 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication January 8, 2013.
- Accepted for publication May 24, 2013.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Liver Function Changes After Technetium-99m-Macroaggregated Albumin Administration and Their Predictive Value Regarding Hepatotoxicity in Patients Undergoing Yttrium-90-Radioembolization
- Efficacy of Radioembolization with 166Ho-Microspheres in Salvage Patients with Liver Metastases: A Phase 2 Study
- Insights into the Dose-Response Relationship of Radioembolization with Resin 90Y-Microspheres: A Prospective Cohort Study in Patients with Colorectal Cancer Liver Metastases