


Abstract
Paragangliomas are neuroendocrine tumors expressing somatostatinergic receptors and, thus, may be imaged by somatostatin receptor scintigraphy (SRS). The purpose of the study was to assess the contribution of SRS in the management of paraganglioma of the head and neck. Methods: 111In-Pentetreotide (148 MBq) was intravenously administered to 3 groups of patients. Group A consisted of 9 patients with tumors of the head and neck that did not exhibit typical radiologic features of paragangliomas and required further diagnostic evaluation. Group B consisted of 28 patients with known paragangliomas or paraganglioma metastatic lymph node who required staging and assessment of multicentricity. Group C consisted of 5 asymptomatic relatives of affected individuals who required screening. All patients underwent clinical, laboratory, radiologic, and audiovestibular evaluation. Results: In group A (n = 9), SRS was positive in 6 cases, 4 paragangliomas and 2 meningiomas, and negative in 3 patients in whom the initial diagnosis of paraganglioma was excluded. In group B (n = 28), SRS was strongly positive in all of the 34 head and neck masses diagnosed on conventional imaging to be paragangliomas; it localized 1 primary malignant paraganglioma and revealed 9 unexpected foci. In group C (n = 5), SRS was positive in 3 of the 5 relatives, CT or MR scan confirming the diagnosis of paraganglioma in all cases. Conclusion: Because of very high sensitivity in detecting paraganglioma, SRS should be included in a multiple-step strategy for patients’ management. It could be useful in ruling out the diagnosis of schwannoma, but its major advantage may involve patients’ staging. Once biologic genetic testing of affected patients’ relatives evidenced the predisposing mutation, SRS could be proposed to identify individuals who express the disease.
Paragangliomas of the head and neck are very rare tumors (about 1 in 30,000 head and neck tumors) (1). Because these tumors are poorly accessible and highly vascularized, diagnostic biopsy is impracticable due to the risk of significant bleeding and injury to adjacent neurovascular structures. Thus, the diagnosis relies usually on both suggestive clinical and radiologic signs. Tympanic paragangliomas are easily identified early by pulsatile tinnitus and the presence of a reddish retrotympanic mass. Similarly, carotid body paragangliomas are suspected by a laterocervical mass. In both cases, conventional imaging (i.e., CT and MR scans) can confirm the clinical suspicion by demonstrating a hypervascularized lesion confined to the middle ear or the carotid body area. Conversely, diagnosis of jugular foramen or vagal paragangliomas is more challenging. Revealing symptoms are late and consist of neurologic (lower cranial) deficits or otologic symptoms. CT and MR scans provide highly suggestive information, including hypervascularization or bony erosion. However, in some instances, the radiologic data are not conclusive and other tumor types such as meningioma, schwannoma, or metastasis may be considered. Arteriography may further narrow the differential diagnosis but the risk of neurologic complications limits its use, thereby making a noninvasive diagnostic method all the more appealing.
Just as in other neuroendocrine tumors, paragangliomas overexpress somatostatin receptors (sst) (2,3) and, as such, may be evidenced by somatostatin receptor scintigraphy (SRS) (3–8). SRS has been used to stage the tumor (8,9) at other paraganglioma sites or neoplasms. These associated tumors may influence the therapeutic management. Such evaluation is not easily done by conventional imaging modalities, which are usually limited to the site of the primary tumor. Furthermore, paragangliomas are inherited in 10%–50% of cases (10,11), and recent genetic studies have identified mutations involved in this disease (12). Thus, SRS could be of great interest in screening asymptomatic patients. By revealing early small paragangliomas, it could lead to early and potentially less morbid treatments.
The purpose of the study, in a series of 42 patients, was to evaluate the clinical impact of SRS (a) in confirming the diagnosis of paraganglioma in a group of patients with clinically suspected paraganglioma but nonconclusive conventional imaging and (b) in staging patients considered to have head or neck paragangliomas on the basis of conventional imaging. We then proposed a multiple-step strategy in the pretherapeutic management of head or neck tumors. Moreover, we evaluated SRS in screening asymptomatic relatives of paraganglioma patients.
MATERIALS AND METHODS
Inclusion Criteria
Consecutive patients were included in the Department of Nuclear Medicine, Lariboisière Hospital, between July 2001 and February 2003:
Group A consisted of patients with head or neck masses suspected clinically to be paragangliomas that could not be confirmed by conventional imaging—that is, discordant CT and MR scan results. SRS was performed to confirm the diagnosis of paraganglioma; group B consisted of patients with either known primary or metastatic paragangliomas who were referred for staging or assessment of multicentricity; group C consisted of asymptomatic relatives of at least 2 previously diagnosed individuals.
Exclusion Criteria
Patients unwilling to participate, nursing mothers, and women susceptible to pregnancy were excluded.
Conventional Imaging Criteria for Positive Diagnosis of Paraganglioma
The typical CT appearance of a paraganglioma is a well-defined soft-tissue mass with intense enhancement after intravenous administration of contrast material. CT is excellent for evaluating the temporal bone. Progressive growth of the tumor produces the typical moth-eaten pattern of erosion of the bone.
The MRI appearance of paragangliomas typically exhibits a signal isointensity relative to muscle with standard spin-echo T1 sequences and a high signal intensity with T2 sequences. Multiple serpentine and punctuated areas of signal void characterize the typical paraganglioma with all MR sequences and are believed to represent flow voids in the larger intratumoral vessels.
As with CT, a homogeneous and intense pattern of enhancement is noted after the intravenous administration of contrast material. MR angiography may be useful in defining the flow-related enhancement of feeding vessels in paragangliomas.
Angiography displays a typical hypervascularized mass with enlarged feeding arteries, intense tumor blush, and early draining veins.
SRS Data Acquisition
111In-Pentetreotide (148 MBq) was intravenously administered. Planar images of the neck, head (anterior, posterior, and lateral views), chest, and abdomen (anterior and posterior views) were obtained 24 h after injection, with a double-head, large-field-of-view gamma camera (HELIX; Elscint) fitted with medium-energy, parallel-hole collimators. The photopeak was centered over 173 keV with a window width of 20%. Acquisition parameters were 128 × 128 word matrix, 15 min per view. Tracer uptake by the tumor was visually evaluated as previously reported (13): Tumor uptake was compared with uptake in the skull, defining a 4-step grading, ranging from 0 (nonvisualization of tumor activity) to 3 (uptake clearly greater than skull uptake, dominating the image).
RESULTS
Population
Forty-two patients were included (22 females, 20 males): 9 in group A, 28 in group B, and 5 in group C. Characteristics of the population are summarized in Tables 1, 2, and 3. Data of some of these patients have been previously published (7).
Characteristics of Group A Patients
Characteristics of Group B Patients
Characteristics of Group C Patients
In group A (Table 1), SRS was positive in 6 patients, all localizations demonstrating an intense uptake (grade 3): Paraganglioma was confirmed in 4 patients. In 2 patients, arteriography did not reveal the typical pattern of paraganglioma but, rather, suggested meningioma: One patient underwent surgery and histology confirmed this diagnosis. In the last 3 patients, SRS was negative and the diagnosis of paraganglioma was excluded on the basis of repeated conventional imaging during follow-up in 1 patient (A8) and on histology after surgery in 2 patients (A6 and A9).
In group B (Table 2), SRS demonstrated an intense uptake in the 34 known head or neck masses previously diagnosed as paraganglioma on conventional imaging. In patient B28, referred for staging of a metastatic paraganglioma cervical lymph node, SRS revealed tracer uptake only in the retrostyloid space, suggesting that a vagal paraganglioma in this location was the primary tumor. SRS was positive in 9 unexpected locations (Fig. 1), 6 with a grade 3 uptake, 2 with a grade 2 uptake, and 1 with a grade 1 uptake. In patient B9, SRS missed 1 of the 2 skull locations that were displayed on 99mTc-hydroxymethylene diphosphonate (HMDP) bone scintigraphy (Fig. 2).

Discovery of abdominal site by SRS (black arrow), confirmed by CT scan (white arrow) in patient B9.
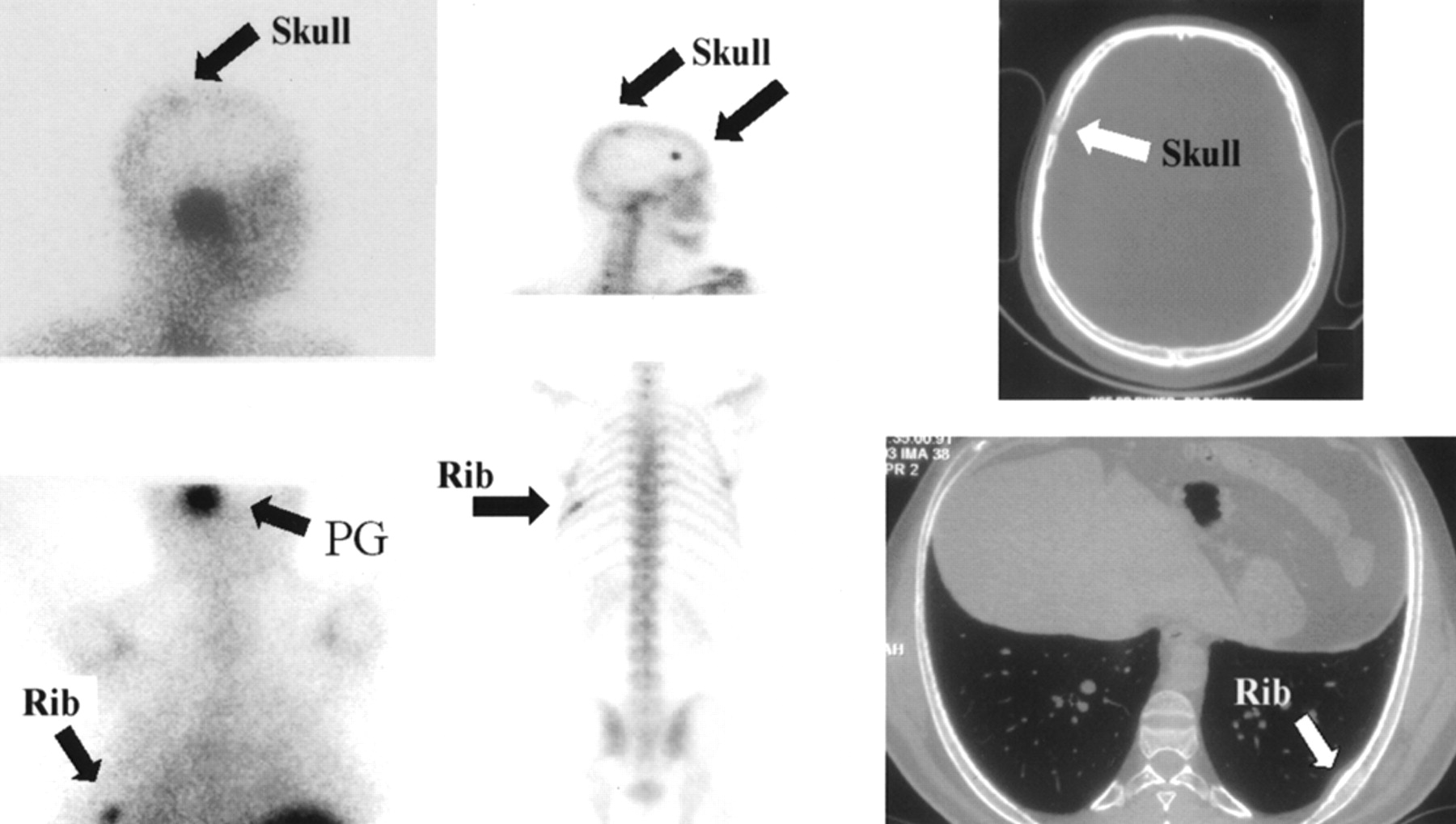
Bone locations in patient B9. Left column: SRS data. (Top) One skull location (black arrow). (Bottom) One rib location (black arrow). PG = paraganglioma. Middle column: 99mTc-hydroxymethylene diphosphonate bone scintigraphy data. (Top) Skull locations (black arrow). (Bottom) Rib location (black arrow). Right column: CT scan data. (Top) Head CT scan (white arrow). (Bottom) Thoracic CT scan (white arrow).
In group C (Table 3), 3 of the 5 relatives of affected individuals displayed intense bilateral uptake in the carotid body areas. Conventional imaging (CT or MR scan) supported the diagnosis of paraganglioma in all 3 cases.
Among all patients, 8 had undergone surgery previously for paragangliomas. In those patients, SRS showed no evidence of any local recurrence.
Only 1 patient (B14) had a functional paraganglioma.
Influence of SRS on Patient Management
Management was changed in 4 patients after SRS. In patient B8, the finding of a hot spot in the thyroid area led to an inconclusive fine-needle aspiration biopsy; an oncocytic adenoma was diagnosed on the surgical specimen. In patients B14 and B27, the discovery of thoracic lesions led the medical staff to start a medical therapy with octreotide. In patient B9, the discovery of skull and rib hot spots led to the performance of 99mTc-HMDP bone scintigraphy, which confirmed the 2 bone locations displayed by SRS and revealed a second skull location. This patient staging led to start a discussion about internal radiotherapy. Patient C4 has undergone surgery.
DISCUSSION
Paragangliomas of the head and neck develop from neural crests and are located in 4 main areas: the tympanic cavity along the course of Jacobson’s nerve, the dome of the jugular bulb in the foramen jugulare, the plexiform ganglion of the vagal nerve, and the carotid body. The literature shows that authors refer to these tumors under various terms, such as glomus tumors, because they were believed to arise from specialized pericytes of blood vessel origin similar to glomus tumors found in the skin, or chemodectomas, because the carotid body was considered as a chemoreceptor. Other terms, such as glomerulocytoma, nonchromaffin tumors, and receptoma, are also found in the literature, adding to the confusion in nomenclature.
Currently, all of these tumors should be referred to as paragangliomas and further delineated by their anatomic sites of origin—that is, tympanic paraganglioma, jugular paraganglioma, vagal paraganglioma, and carotid body paraganglioma.
Diagnosis of paraganglioma usually relies on both suggestive clinical and conventional imaging (CT and MR scan) signs. However, particularly for skull base locations, symptomatology and radiologic data are not always conclusive and another tumor type may be considered. For instance, in areas where paragangliomas usually develop, the most frequent tumors are meningiomas, which are hypervascularized tumors, and schwannomas, which conversely are poorly vascularized. Both are more frequent than paragangliomas. Two different methods may contribute to defining the diagnosis: (a) arteriography, based on vascular characteristics of the lesion. However, its use is limited by the risk of neurologic complications; and (b) SRS, a noninvasive method, based on the intrinsic characteristic of some tumors, such as paragangliomas (2–8) and meningiomas (2,14–16), which may overexpress somatostatin receptors (sst). Thus, SRS excludes schwannomas that do not express sst (15,17) and, thereby, could avoid unnecessary arteriography (2 patients in our series). SRS cannot differentiate paraganglioma from meningioma, as demonstrated by our data, where all head or neck paragangliomas (n = 45) and meningiomas (n = 2) were both visualized by SRS. This distinction cannot be made by 123I-metaiodobenzylguanidine (123I-MIBG) scintigraphy because 123I-MIBG uptake is not constant in paragangliomas (6). Therefore, a negative 123I-MIBG result could not be properly interpreted and cannot be helpful in differentiating paraganglioma from meningioma.
The distinction between meningioma and paraganglioma can then be made by arteriography. SRS could limit the use of arteriography to patients who intend to undergo surgery and require an embolization procedure for these hypervascularized tumors.
Therefore, SRS could be proposed as the first diagnostic step after CT or MRI as proposed in Figure 3. The high sensitivity of SRS reported by other studies supports this proposal. Reubi et al. (3) reported that all paragangliomas expressed sst in vitro. Kwekkeboom et al. (4) confirmed, in a slightly smaller clinical series than ours, the very high sensitivity of SRS for the diagnosis of paraganglioma. Schmidt et al. (8) also reported the use of SRS in a series of 19 patients, 11 of whom had a proven paraganglioma. The goal of including SRS at this step is to reduce the practice of arteriography.

Management of patients with suspected head or neck paraganglioma.
However, the major advantage of SRS is to improve the ability to stage the patient tumor. As in other neuroendocrine tumors, head and neck paragangliomas are frequently associated with other paraganglioma sites or neoplasms, which may express sst. Multicentricity appears in approximately 10% of sporadic paragangliomas and in 30%–40% of familial paragangliomas (10,11,18,19). Multiple paragangliomas are usually located in the head and neck area but may be thoracic or abdominal (adrenal or extraadrenal) (20,21). In our series, SRS revealed 1 cervical, 4 thoracic, and 1 abdominal unsuspected focus. Paragangliomas may be associated with other tumor types, such as astrocytomas (22), thyroid carcinomas (18,23), and parathyroid adenomas (24). They may be part of multiple endocrine neoplasm type II (25), associated with medullary thyroid carcinoma, hyperparathyroidism, and pheochromocytoma. Spector et al. (26), in a series of 95 patients with paragangliomas, showed a 7% incidence of associated neoplasms. These associated tumors may express somatostatinergic receptors (2,17,27,28) and, therefore, be detected by SRS. One patient in our study had an oncocytic adenoma revealed by SRS. Malignancy has been reported in 6% of carotid body paragangliomas (29), 5% of jugulotympanic tumors (30), and 10%–19% of vagal tumors (31,32). The only criterion of malignancy is the presence of metastasis (33). In 1 of our patients (B28), SRS detected the primary lesion after a metastatic cervical lymph node was diagnosed and, in 1 other (B9), SRS revealed bone metastasis.
In our population, considering groups A and B with respect to the flow diagram proposed in Figure 3, arteriography was avoided for the 2 patients with schwannoma, resulting in a cost savings of 950 Euros (∼$1,100). Conversely, the systematic addition of SRS led to an added cost of 10,465 Euros (∼$11,897). This procedure allowed the detection of unknown localizations in 3 patients, contraindicating the surgical removal of the primary lesion (about 6,000 Euros [∼$6,821] per patient), thus resulting in better patient management.
SRS has been recommended as a modality to detect local recurrence or residual tumor after surgery (4), which may occur in 15%–30% of paragangliomas (34,35). In these surgical patients, radiologic differentiation between tumor and scar tissue may be difficult. In 7 patients of our study who previously underwent surgery for paraganglioma and for whom tumor resection had been considered to be complete, SRS did not visualize any enhancement suggestive of residual tumor in the surgical area. Therefore, SRS may be helpful to confirm the completeness of tumor removal.
All head and neck paragangliomas had high tracer uptake and, thus, SRS imaging was clearly demonstrative even on planar images, using a relatively low injected dose. Complementary SPECT acquisition, which was not performed in our series, could enhance tumor localization, but tumor localization has been accurately achieved before SRS by CT and MRI. This very high SRS uptake allows for diagnosis of tumors with a volume as small as 0.2 cm3.
SRS may have a very important impact in cases of inherited disease. In our study, SRS found 3 affected patients of the 5 asymptomatic relatives. According to the literature, paragangliomas are inherited in 10%–50% of cases (10,11). The variability of this reported incidence is due to different criteria used for the familial inquiries. Because mutations involved in this disease have now been characterized (12), it is possible to biologically identify mutant patients who are predisposed to clinically express the disease. Because the penetrance of the mutation is variable, SRS should be performed in this subset of patients, biologically selected, to detect those who express the disease. As an illustration of the variability of the mutation’s penetrance, an asymptomatic 46-y-old patient (C3), who was necessarily affected by the mutation because his mother and his 2 sons were themselves affected, had negative SRS.
It must be emphasized that hereditary paragangliomas are often multicentric and frequently located in the carotid body area (10,18). Therefore, staging of these patients is particularly important to exhaustively detect all tumor sites. It could be expected that management of such asymptomatic (and still limited lesions) would lead to less iatrogenic complications in their treatment. In terms of dosimetry, SRS is equivalent to a thoracic or abdominal CT scan. We propose here a multiple-step strategy for familial investigation (Fig. 4).

Familial inquiry.
In the future, patient management might be slightly different. First, angio-MRI might limit the use of arteriography but would not diminish the importance of SRS in patient staging or in screening of asymptomatic relatives. PET imaging may have future implications for the management of these patients (36) despite the fact that 18F-FDG uptake was reported to be low or absent in some neuroendocrine tumors (37). Other tracers with higher affinity for sst than 18F-FDG could probably be developed in the future. As an illustration, the clinical impact of 68Ga-labeled 1,4,7,10-tetraazacyclododecane-N,N′,N″,N‴-tetraacetic-acid-d-Phe1-Tyr3-octreotide has been reported in carcinoid tumor (38) and in meningiomas (39). The potential interest of the tracer is not the differentiation between paraganglioma and meningioma (both are supposed to demonstrate a similar uptake) but is to offer a high spatial resolution, a better localization (particularly when data are acquired with hybrid PET/CT systems), and a better uptake quantification. This latter point could be particularly relevant clinically if external or internal radiotherapy is discussed.
CONCLUSION
Paragangliomas are neuroendocrine tumors that may be difficult to diagnose and can be completely asymptomatic. SRS demonstrated a very high sensitivity in detecting paragangliomas and might be included in a multiple-step diagnosis strategy. Furthermore, because multiple tumor sites or association with other tumors is frequent, exhaustive staging by SRS should be performed before therapy. Once the diagnosis of paraganglioma is confirmed in a patient, familial investigation should be performed. The use of SRS could be extended to relatives of affected patients who biologically express the involved mutation.
Footnotes
Received Apr. 11, 2003; revision accepted Jul. 22, 2003.
For correspondence or reprints contact: Michèle Duet, MD, Service de Médecine Nucléaire, Hôpital Lariboisière, 2 rue Ambroise Paré, 75010 Paris, France.
E-mail: michele.duet{at}lrb.ap-hop-paris.fr
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Molecular and Therapeutic Advances in the Diagnosis and Management of Malignant Pheochromocytomas and Paragangliomas
- Modern Nuclear Imaging for Paragangliomas: Beyond SPECT
- The SNM Practice Guideline for Somatostatin Receptor Scintigraphy 2.0
- Expression of somatostatin receptors, dopamine D2 receptors, noradrenaline transporters, and vesicular monoamine transporters in 52 pheochromocytomas and paragangliomas
- Somatostatin receptor-based imaging and therapy of gastroenteropancreatic neuroendocrine tumors
- Comparison of 6-18F-Fluorodopamine PET with 123I-Metaiodobenzylguanidine and 111In-Pentetreotide Scintigraphy in Localization of Nonmetastatic and Metastatic Pheochromocytoma
- 111In-Octreotide Is Superior to 123I-Metaiodobenzylguanidine for Scintigraphic Detection of Head and Neck Paragangliomas
- Plasma Cell Problems: CASE 3. Plasmacytoma Mimicking a Paraganglioma of the Skull Base: Diagnostic Value of Somatostatin Receptor Scintigraphy