


Abstract
Molecular alterations in malignant disease result in the expression or upregulations of various targets that can be used for imaging and treatment with radiopharmaceuticals. This theranostic principle has acquired greater importance in personalized medicine in recent years, particularly in oncology, where advanced tumors can be treated effectively with low side effects. Since the pioneering use of 131I in differentiated thyroid cancer in the 1940s, remarkable achievements in nuclear medicine endoradiotherapy have been demonstrated, mainly in the treatment of neuroendocrine neoplasms by using 177Lu-labeled somatostatin analogs or in the treatment of advanced prostate cancer using prostate-specific membrane antigen–directed radionuclide therapy. Besides that, this review focuses on promising novel radiopharmaceuticals and describes their preclinical and clinical status. Radiolabeled antibodies, such as 131I-omburtamab directed against the B7-H3 protein on the surface of neuroblastoma cells; HuMab-5B1, a 89Zr/177Lu-labeled antibody for the treatment of CA19-9–expressing malignancies; and 177Lu-lilotomab, a CD37 antibody for the treatment of B-cell lymphomas, are being highlighted. The neurotensin receptor ligand 111In/177Lu-3B-227 has demonstrated high potential in imaging and therapy for several malignancies (e.g., pancreatic adenocarcinomas). Targeting of the fibroblast activation protein is currently being explored for different tumor entities using PET imaging with the fibroblast activation protein inhibitor (FAPI) 68Ga-FAPI-04, and the first therapeutic applications of 90Y-FAPI-04 have been applied. After 2 decades of rapid development in theranostics, a variety of new targets are available for further clinical investigation.
Theranostics (also called theragnostics) describes a close connection between diagnostics and consequent therapy. The term theranostic was probably first used in 1998 by John Funkhouser, who developed a test for monitoring the efficacy of a new anticoagulant drug (1). In nuclear medicine the term is increasingly being used specifically for imaging and therapy with the same radiopharmaceutical or 2 very similar radiopharmaceuticals. Of course, this concept is not new in nuclear medicine. It has, rather, been used for decades for the therapy of benign and malignant thyroid diseases (2,3). In recent years, however, theranostics has been successfully applied to a whole range of other malignancies, including neuroendocrine tumors (NETs) and prostate cancer in particular.
The efficacy of the therapy of NETs with radiolabeled analogs of somatostatin was ultimately proven in the NETTER-1 trial (4). This study led to the approval of 177Lu-DOTATATE in the United States and later in Europe (5). In parallel, 68Ga-labeled somatostatin analogs were approved for imaging of NETs and patient selection for peptide receptor radionuclide therapy (PRRT) (6,7). More recently, the prostate-specific membrane antigen (PSMA) has been established as a theranostic target for prostate cancer. Currently, a randomized phase III registration trial is recruiting patients to prove the superiority of 177Lu-labeled PSMA-617 for treatment of metastatic castration-resistant prostate cancer (mCRPC) compared with the standard of care (VISION trial (8)). Various imaging agents targeting PSMA are currently in phase I–III studies, aiming for approval as novel diagnostic tools.
These 2 theranostic approaches, as well as the therapy of osseous metastases of prostate cancer with 223Ra (4,9,10), have unequivocally demonstrated that radionuclide therapy can be applied not only to thyroid cancer but also to other solid tumors. Furthermore, it is now clear that radionuclide therapy not only has a palliative effect but can prolong progression-free and overall survival. Current research in theranostics is addressing new targets but—equally important—the optimization of radiopharmaceutical doses and dose schedules, investigation of combination therapies, and treatment at earlier tumor stages.
Advances in the field of preclinical oncology with a main focus on immunology hold promise to discover new molecular targets with potential future applications in theranostics. Recent developments in theranostics will definitely require adjustments in the training of nuclear medicine physicians. Compared with the current approach, which focuses on knowledge of image acquisition and interpretation as a service to our clinical partners, a strong focus is needed on clinical skills and patient management, especially in the oncologic setting. On the one hand, combined training in nuclear medicine and radiology has become increasingly important for educating imaging specialists (11). However, nuclear medicine needs to strengthen its position as a unique profession in daily, multidisciplinary clinical routine. Therefore, a clear, independent profile emphasizing specific strengths compared with neighboring disciplines (e.g., oncology, radiology, and radiation oncology) needs to be refined by, for example, updated licensing of training programs (12). In addition, nuclear medicine theranostics is currently regarded as an interesting business model by many companies. The recent acquisition of AAA and Endocyte by Novartis can be seen as an indication that economic interest in the development of theranostics will continue to grow (13). The approval of future radionuclide therapies will most likely generate further options, which will broaden the supply of patients with well-tolerated targeted therapies through nuclear medicine.
Because of the constantly expanding knowledge and experience gained by numerous research-active centers worldwide, it is impossible to provide a comprehensive review of new developments in theranostics. This review therefore focuses on theranostic agents that are in clinical use or have started clinical development in prospective studies. Because of space constraints, the review is also limited to solid tumors, although there are promising developments for new radioimmunotherapies of hematologic malignancies, such as CD37-targeted therapy of B-cell lymphomas (14) or CD45-targeted therapy of acute leukemias (15).
CURRENT DEVELOPMENTS IN THERANOSTICS
NETs
After the milestone achievements of the NETTER-1-trial and its major impact on the treatment of NETs using PRRT (4), numerous studies are now under way with the aim of improving molecular therapy in NETs and other somatostatin receptor–expressing tumors. In the following section, we briefly describe some of these ongoing studies.
The international phase III COMPETE study (NCT03049189) compares treatment with 177Lu-DOTATOC and the mammalian target of rapamycin inhibitor everolimus in patients with advanced gastroenteropancreatic NETs. Everolimus has been shown to be effective for the treatment of pancreatic and other NETs in the landmark RADIANT 3 and RADIANT 4 trials and is seen by many as the standard treatment for patients with gastroenteropancreatic NETs who progressed after treatment with somatostatin analogs (16).
In the COMPETE trial, 300 patients will be randomized to receive either 10 mg of everolimus per day or a maximum of 4 cycles of PRRT with 7.5 GBq of 177Lu-DOTATOC at 3-mo intervals. The primary endpoint of the study is progression-free survival, and the secondary endpoint is overall survival. If successful, the COMPETE trial is expected to lead to a broader use of PRRT as the primary treatment of gastroenteropancreatic NETs after failure of somatostatin analogs.
A large phase II clinical trial including more than 600 patients with any somatostatin receptor 2–positive malignancy eligible for PRRT with 177Lu-DOTATATE aims to investigate optimized time intervals between PRRT cycles. Progression-free survival, disease control rate, late toxicity, overall survival, and dosimetry data are being collected in a comparative, 2-armed study design examining an intensive (every 5 wk) versus a nonintensive (every 8–10 wk) protocol of PRRT administration (NCT03454763).
Two parallel phase II multicenter trials are recruiting patients to investigate the combination of PRRT with chemotherapy. In the first study, 177Lu-DOTATATE combined with capecitabine and temozolomide chemotherapy is compared with capecitabine and temozolomide alone in the treatment of low- to intermediate-grade pancreatic NETs. In the second study, PRRT with 177Lu-DOTATATE and capecitabine and temozolomide is tested versus PRRT alone in midgut NETs (NCT02358356).
DOTATATE, DOTATOC, and DOTANOC are receptor agonists that stimulate somatostatin receptors as does the natural ligand somatostatin. This stimulation leads to internalization of the receptor together with the bound ligand. Originally, it was assumed that this internalization was a prerequisite for the long intratumoral retention of radiolabeled somatostatin receptor ligands. In contrast, somatostatin receptor antagonists bind to the somatostatin receptor and block the binding of the natural ligand somatostatin but do not stimulate the receptor and do not cause internalization of the receptor (17).
Nevertheless, these antagonists have a potential advantage over agonists. Somatostatin receptor, like other G protein–coupled receptors, have different conformations, and agonists can bind only to so-called active conformations (17). On the cell surface, however, there are up to 100 times more somatostatin receptors in inactive conformations, and somatostatin receptor antagonists also bind to receptors that are in these inactive states (18). Ginj et al. have been the first to investigate radiolabeled somatostatin receptor antagonists for the imaging and therapy of NETs. In their experimental studies, tumor uptake of antagonists was substantially higher than that of agonists despite the lack of receptor internalization (18). High uptake and unexpectedly long retention of somatostatin receptor antagonists were also observed in small series of patients (19,20).
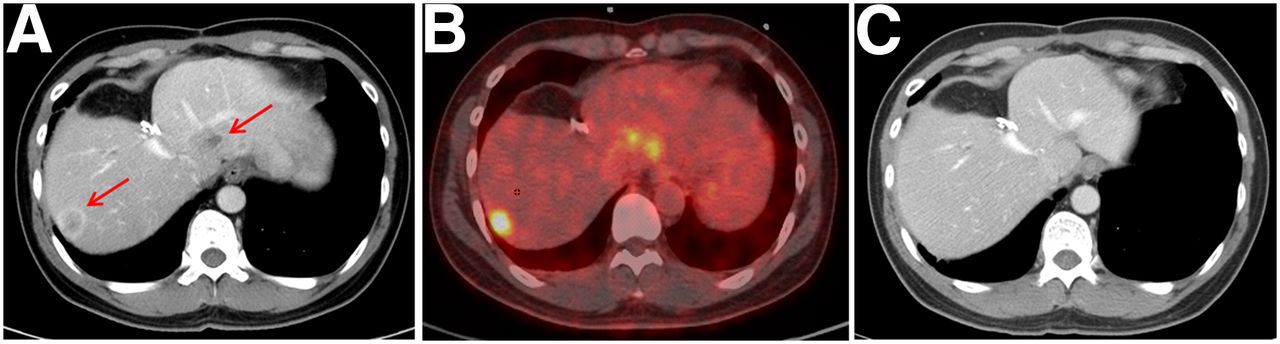
These promising results have led to first diagnostic and therapeutic studies with the antagonists 177Lu-DOTA-JR11 (OPS201) (21) and 68Ga-NODAGA-JR11 (OPS202) (22). In these investigations, PET/CT imaging with 68Ga-NODAGA-JR11 showed a higher image contrast and a higher sensitivity for the detection of metastases of NETs than 68Ga-DOTATOC (22). In a phase I therapeutic study with 68Ga/177Lu-DOTA-JR11, a promising response rate of 37% was found, with a significant decrease in tumor size after only one treatment cycle (Fig. 1). However, the treatment also led to a higher hematotoxicity than observed for somatostatin receptor agonists (21). The safety and efficacy of 177Lu-DOTA-JR11 are being further investigated in ongoing multicenter phase I/II studies (NCT02592707 and NCT03773133).

(A) CT scan of patient with gastric NET showing multiple liver metastases. (B) These metastases display high uptake of 68Ga-DOTA-JR11 on PET/CT. (C) After 1 cycle of 177Lu-DOTA-JR11 (6.6 GBq), most metastases are no longer detectable on CT.
PSMA-Targeting Theranostics
During the last 5 y, radioligand therapy with 177Lu-PSMA has rapidly evolved as a highly promising treatment for patients with mCRPC (Fig. 2). This is perhaps best demonstrated by the fact that it is already recommended by some urologic–oncologic guidelines (23), although no PSMA-targeting radiopharmaceutical has been approved by the Food and Drug Administration or the European Medicines Agency so far.
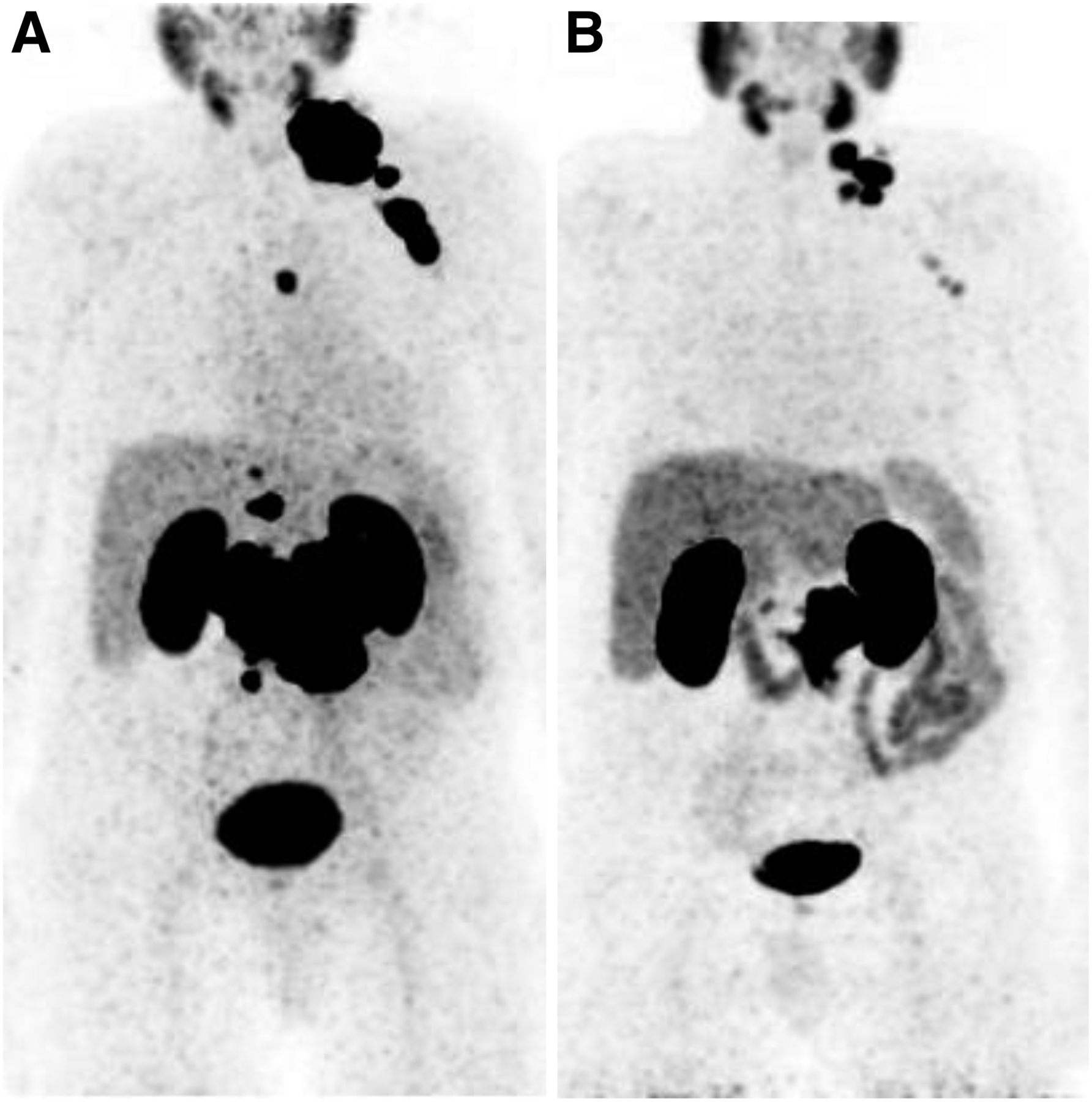
A 77-y-old patient with metastasized castration-refractory prostate cancer (initially cT3a cN1 cM0 G2b, Gleason score of 7). Patient received hormone ablation therapy, local radiation treatment, and several systemic therapies (abiraterone acetate, docetaxel, and enzalutamide). Because of progressive disease, patient was referred for 3 cycles of 177Lu-PSMA therapy. 68Ga-PSMA PET/CT showed PSMA-positive nodal metastases. (A) Maximum-intensity projection. (B) Therapy response after 3 cycles of 177Lu-PSMA. (Reprinted from (59).)
The VISION trial aims for approval of 177Lu-PSMA-617, and enrollment is expected to end in late 2019 (8). The study randomizes 750 patients in a 177Lu-PSMA-617 arm versus a standard-of-care arm in a 2:1 fashion. Its primary co-endpoints are overall survival and progression-free survival. Patients who have had at least one regime of chemotherapy and secondary hormonal manipulation are eligible (NCT03511664).
The TheraP phase II trial compares 177Lu-PSMA-617 with the second-line chemotherapy agent cabazitaxel in mCRPC (24). Two hundred patients with metastatic prostate cancer who have progressed despite hormonal therapy and first-line chemotherapy are randomized to receive either 177Lu-PSMA radionuclide therapy (up to a maximum of 6 cycles of therapy) or cabazitaxel chemotherapy (up to a maximum of 10 cycles of therapy). The study will determine the effects on prostate-specific antigen (PSA) response rate (primary endpoint), pain response, progression-free survival, quality of life, and frequency and severity of adverse events (NCT03392428).
Further advances are expected when PSMA-targeted radioligand therapy is combined with other treatments. The LuPARP study investigates 177Lu-PSMA-617 therapy and olaparib in patients with mCRPC (NCT03874884). It is a phase I, open-label, multicenter study and is designed to evaluate the safety and tolerability of olaparib in combination with 177Lu-PSMA in patients with mCRPC who have previously progressed on a novel androgen receptor–targeted agent (abiraterone or enzalutamide or apalutamide) and have not had prior exposure to platinum agents. Patients will be enrolled in 2 stages: a dose escalation phase followed by an expansion phase. The clinical and translational outcomes from this study are intended to inform the design of future phase II/III clinical trials of this combination. The PRINCE trial is a phase Ib/II study of 177Lu-PSMA-617 therapy (up to 4 doses) in combination with pembrolizumab (up to 35 cycles) for treatment of mCRPC (NCT03658447). Primary outcome measures are adverse events and PSA response.
A different approach to increase the efficacy of PSMA-targeted radioligand therapy is the use of the α-emitter 225Ac. An initial investigation has shown that targeted α-therapy with radiolabeled PSMA inhibitors can induce dramatic responses and that hematologic toxicity is low even in the presence of diffuse osseous and bone marrow metastases (25). However, xerostomia was significantly more severe than for 177Lu-labeled PSMA ligands and became the predominant dose-limiting toxicity. After an initial empiric dose-finding study, Kratochwil et al. used a fixed-dose regimen of 100 kBq/kg of body weight in a larger cohort of patients and found 225Ac-PSMA-617 to have remarkable antitumor activity (26). This study also provided preliminary evidence that responses to targeted α-therapy can be as durable as for other therapies for castration-resistant prostate cancer.
One case series also reported on the use of 225Ac-PSMA-617 radioligand therapy in chemotherapy-naïve patients with advanced metastatic prostate carcinoma. In this earlier state of prostate cancer, a PSA decline of at least 90% was observed in 82% of patients, including 41% of patients with undetectable serum PSA, who remained in remission for 12 mo after therapy (27). The remarkable therapeutic efficacy reported in this study could be achieved with reduced toxicity to the salivary glands due to deescalation of administered activities in subsequent treatment cycles. However, prospective data on the long-term efficacy and toxicity of 225Ac-PSMA-617 radioligand therapy in comparison to chemotherapy are clearly required before 225Ac-PSMA-617 radioligand therapy can be used more broadly in chemotherapy-naïve patients.
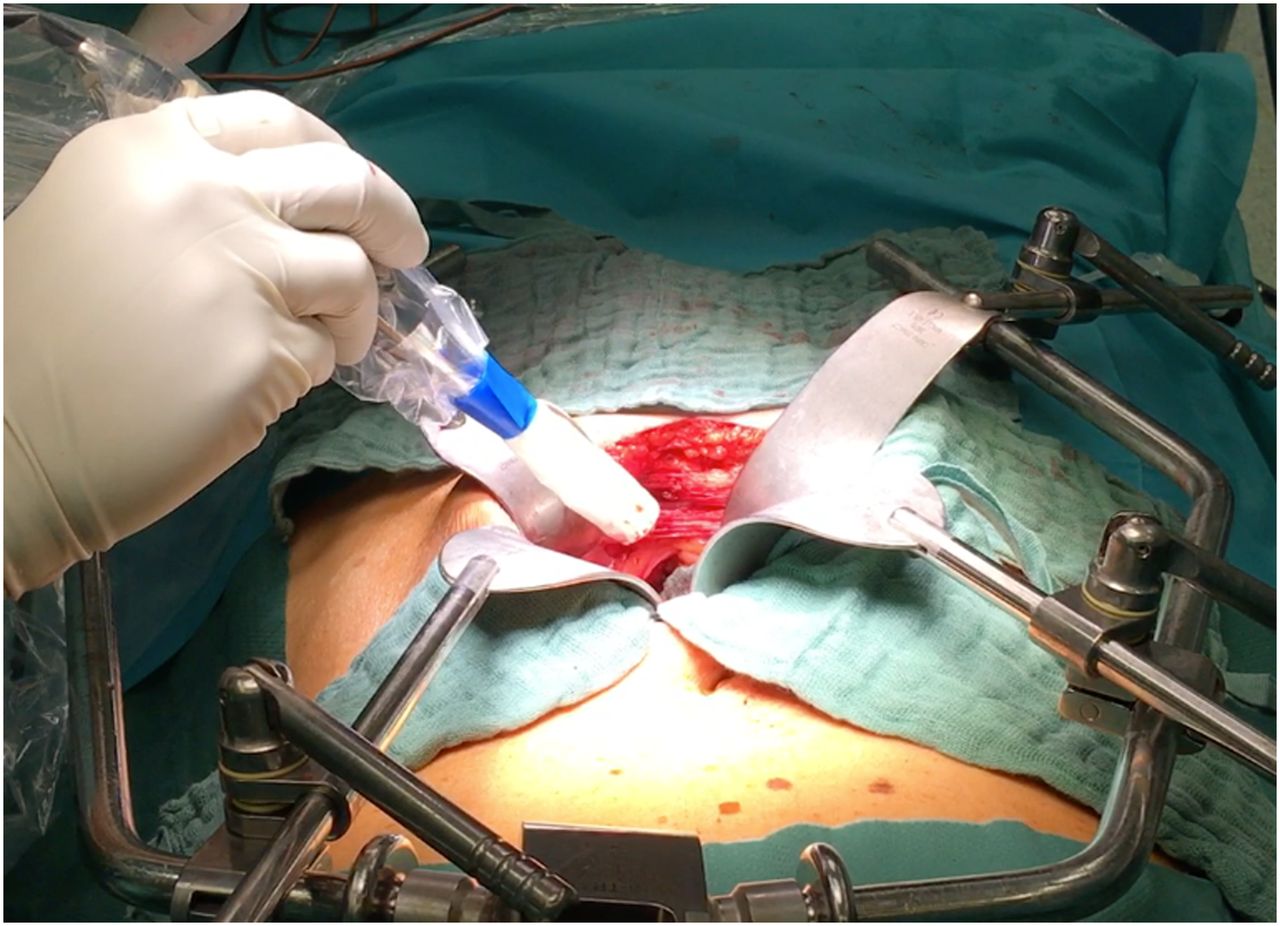
Besides PSMA-targeted radioligand therapy, PSMA-targeted radioguided surgery is an increasingly applied theranostic approach not in advanced but in early prostate cancer recurrence (Fig. 3). It uses preoperative application of γ-emitting PSMA-targeting probes that radiolabel tumor tissue (28–30). The subsequent intraoperative use of a γ-probe facilitates detection of these typically small or atypically localized lesions and improves complete resection of the recurrence. Early reports state superb rates of intraoperative tumor detection and a substantial PSA decline in a high number of patients (29,31).
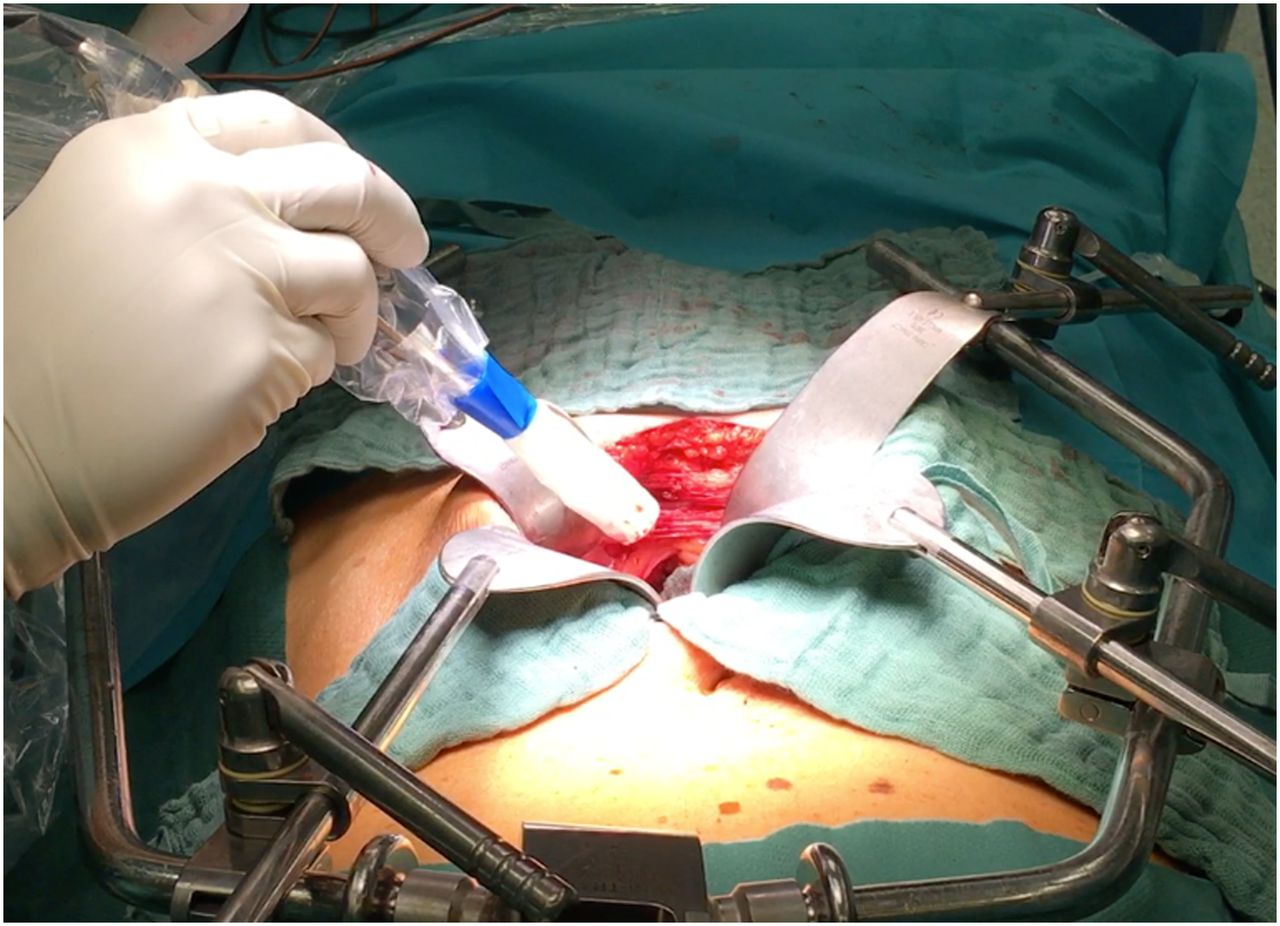
PSMA-targeted radioguided surgery. (Reprinted from (59).)
In a recently published series of 121 patients, a complete biochemical remission (defined as PSA < 0.2 ng/mL after PSMA-targeted radioguided surgery) was achieved in 77 patients (65.8%) (32). The frequency was higher in patients with a preoperative PSA value below the median (76.3% vs. 55.2%, P = 0.018) and a single lesion versus multiple lesions on preoperative PSMA-ligand PET (73.7% vs. 51.2%, P = 0.025). Median biochemical recurrence-free survival was 6.4 mo in the whole patient cohort and 19.8 mo for patients with a complete biochemical response. A significantly longer median biochemical recurrence-free survival was observed in patients with a preoperative PSA value below the median (14.9 vs. 4.4 mo, P = 0.02) and with a single lesion on preoperative PET (14.0 vs. 2.5 mo, P = 0.0007).
PERSPECTIVES ON NOVEL TARGETS AND RADIOPHARMACEUTICALS
FAP/FAPI-04
The fibroblast activation protein (FAP) is a serine proteinase that is highly expressed on the cell surface of activated fibroblasts but not of resting fibroblasts (33). FAP is physiologically expressed in many tissues during embryonic development, but in adults it is expressed only in the context of wound healing, fibrotic processes, and the stroma of many malignancies. In histopathologic studies, FAP-positive cancer-associated fibroblasts were found in over 90% of epithelial tumors. This makes FAP a potential target for imaging and therapy of a large variety of malignancies (34).
Because of these promising characteristics, FAP antibodies, immunoconjugates, chimeric antigen receptor T cells, vaccines, and small-molecule FAP inhibitors (FAPIs) have already been developed (35). In 1994, a high accumulation of the 131I-labeled monoclonal antibody 19F was observed in metastases of colon carcinoma. Despite the limitations of imaging with 131I, metastases with a diameter of 1 cm were detected (36). Nevertheless, imaging with FAP antibodies was not further pursued, probably because of the success of 18F-FDG PET and the logistical challenges and high radiation exposure of imaging with radiolabeled antibodies.
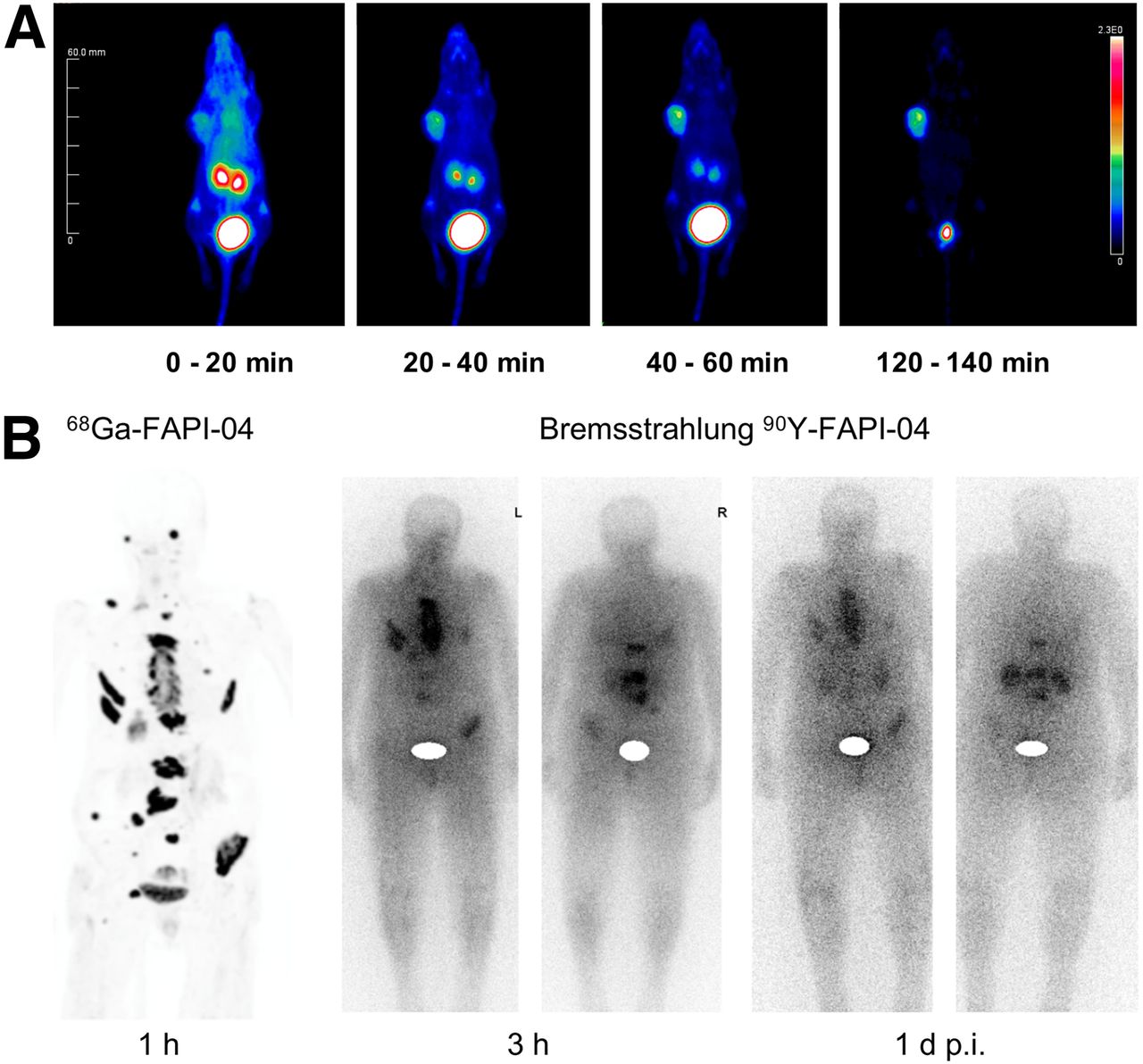
However, in 2018, Haberkorn’s group presented highly promising preclinical and clinical data on radiolabeled, low-molecular-weight FAPIs (35,37,38). These quinoline-based inhibitors were labeled with diagnostic and therapeutic radioisotopes via the chelator DOTA (35). The compound FAPI-04 showed the most favorable properties (low nanomolar affinity to FAP, almost complete internalization of radioactivity bound to FAP, and rapid blood clearance). 68Ga-FAPI-04 has already been used in several patients with metastatic tumors (35,38). These clinical studies confirmed the favorable biodistribution expected from animal models and showed rapid tumor uptake of 68Ga-FAPI-04 with excellent image contrast (Fig. 4A).

Imaging and therapy with inhibitor of FAP. (A) Biodistribution of 68Ga-FAPI-04 in mouse tumor model expressing FAP (soft-tissue sarcoma). Rapid accumulation in tumor tissue and renal clearance without accumulation in normal tissues were observed. (Adapted from (35).) (B) 68Ga-FAPI-04 PET (maximum-intensity projection) and planar Bremsstrahlung images of patient with osseous breast cancer metastases treated with 90Y-FAPI-04. (Reprinted from (35).)
A first therapeutic application of 90Y-FAPI-04 has already been published (Fig. 4B) (35). High accumulation of 90Y-FAPI-04 was shown in a metastasis of a patient with advanced breast cancer. A significant improvement in symptoms was achieved with a single dose of 90Y-FAPI-04. However, FAPI-04 shows a relatively fast clearance from tumor tissue, limiting the achievable radiation dose. Hence, the effectiveness of FAP-directed radionuclide therapy can probably be improved by ligands with longer retention in the tumor tissue.
Neurotensin/177Lu-3BP-227
Neurotensin is a 13-amino-acid neuropeptide that is physiologically found in the adult central nervous system, the gastrointestinal tract, and the myocardium (39,40). Neurotensin interacts with 3 neurotensin receptors (NTSRs): NTSR1, NTSR2, and NTSR3. Neurotensin-producing neurons are widespread in the brain and involved in several neuronal functions such as pain processing, blood pressure regulation, and food intake regulation (41). Outside the brain, neurotensin acts as a hormone with numerous endocrine and paracrine functions, such as regulation of intestinal motility, secretion of the pancreas, and tone of smooth vascular muscles (42).
Neurotensin and NTSRs are also expressed in various tissues during embryogenesis, and their expression is reactivated in several malignancies, such as small cell and non–small cell bronchial carcinomas, colorectal carcinomas, breast carcinomas, and pancreatic carcinomas (40). Binding of neurotensin to NTSR1 can stimulate the proliferation of tumor cells via various signaling pathways such as phospholipase C (43). In addition, the motility and invasiveness of tumor cells can be increased by activating ρ-kinases. For these reasons, neurotensin antagonists such as SR48692 have been developed for tumor therapy.
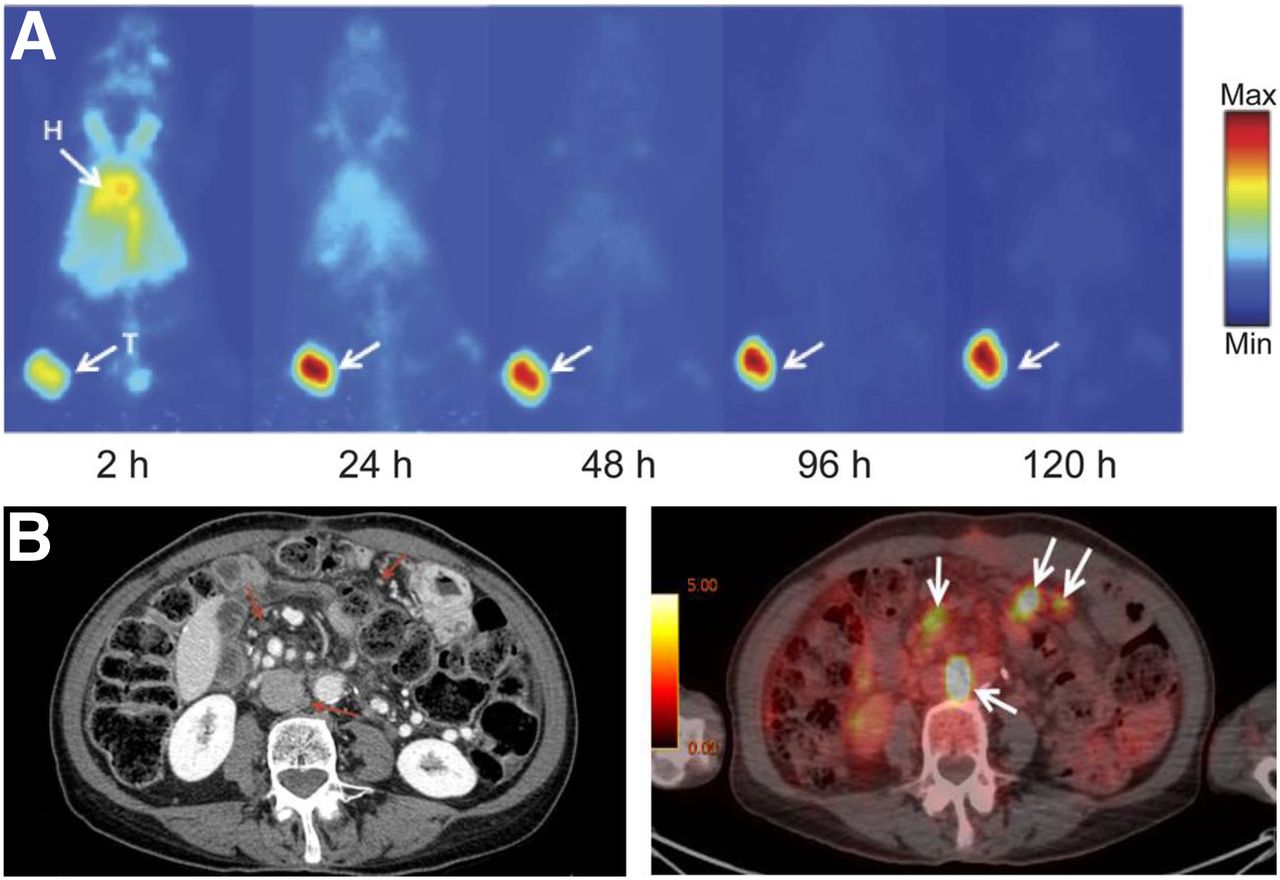
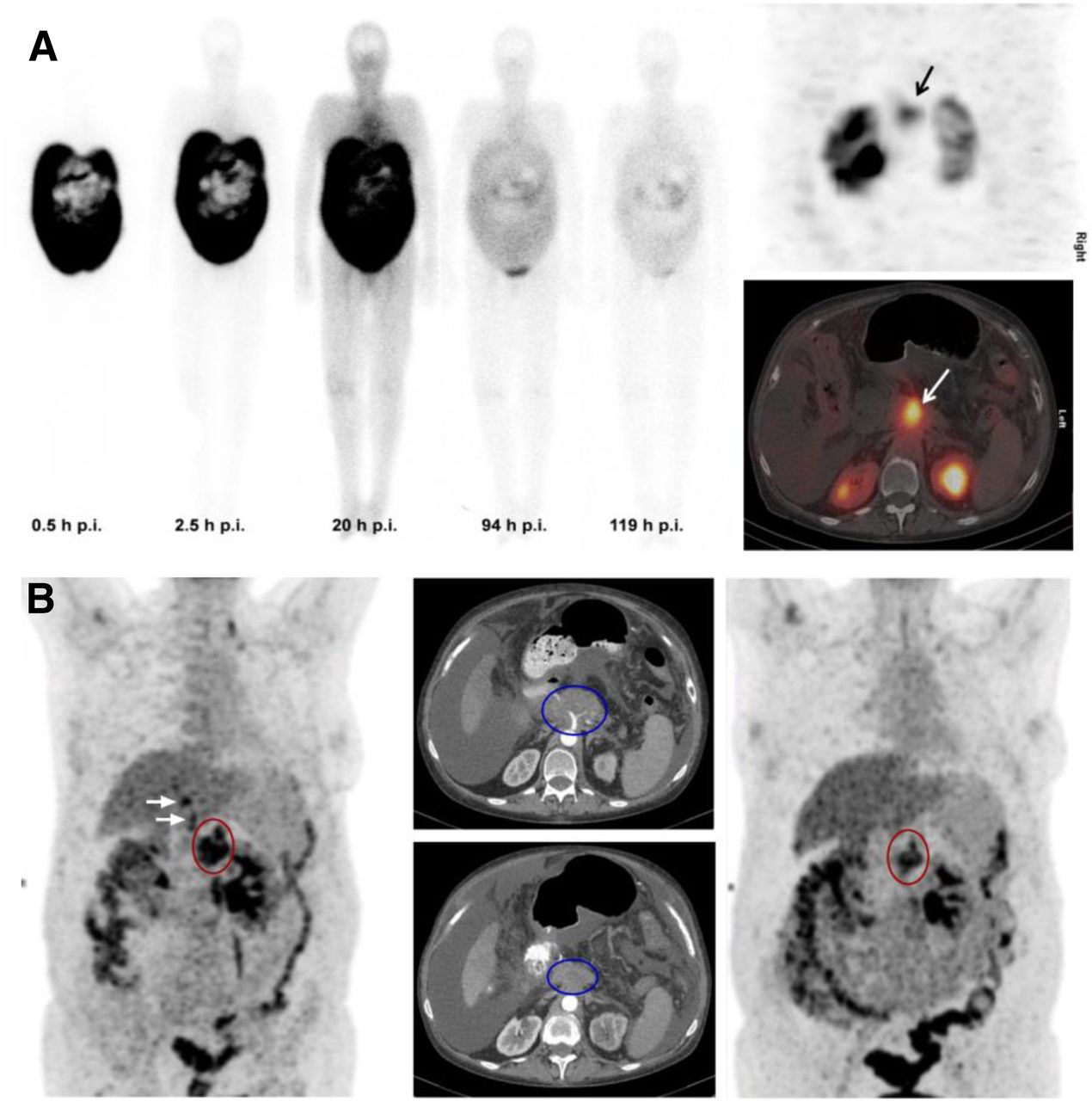
According to autoradiographic studies, the density of NTSR1 on pancreatic adenocarcinoma can be as high as the expression of type 2 somatostatin receptors in NETs (44). Thus, radiolabeled NTSR1 ligands represent an interesting option for radioligand therapy of pancreatic carcinomas. 177Lu-3BP-227 (Fig. 5A) is a highly affine nonpeptide NTSR1 antagonist (45). Preclinical studies on tumor-bearing mice have shown that 177Lu-3BP-227 accumulates in NTSR1-positive tumors with a high target-to-organ ratio compared with kidneys, liver, gastrointestinal tract, and lung (46).

Radionuclide therapy with NTSR1 ligand. (A) Biodistribution of 177Lu-3BP-227 up to 119 h after intraperitoneal application in patient with pancreatic carcinoma and peritoneal carcinosis. SPECT/CT images were taken 96 h after injection. (B) Treatment response of patient after 3 cycles of 177Lu-3BP-227 on 18F-FDG PET/CT imaging. Primary tumor shows decreased metabolic activity on PET (red circles) and size reduction on CT (blue oval). (Reprinted from (47).)
On the basis of these promising data, radioligand therapy with 177Lu-3BP-227 was attempted in 6 patients with advanced pancreatic adenocarcinomas and no other treatment options (47). In 5 of these patients, a significant 177Lu-3BP-227 uptake in tumor tissue could be observed and radioligand therapy was applied. In one of the patients with extensive peritoneal carcinosis, partial remission was achieved after intraperitoneal administration of 177Lu-3BP-227 (Figs. 5A and 5B). The patient survived another 11 mo after therapy (47).
Currently, a phase I/II study is being conducted to treat advanced NTSR1-positive tumors with 177Lu-3BP-227 (NCT03525392). The aim of the phase I study including 30 patients is to perform dosimetry and investigate side effects of 177Lu-3BP-227, as well as to determine the activity level for a phase II study. In phase II, 55 patients with pancreatic carcinoma and 70 patients with colorectal carcinoma will be treated to evaluate tumor response to 177Lu-3BP-227 therapy (NCT03525392).
B7-H3 (CD276)/Omburtamab
B7-H3 is a transmembrane B7 glycoprotein. B7 proteins play a central role in the regulation of the immune response and are important targets for the immunotherapy of malignant tumors. The interactions of B7 proteins on the surface of antigen-presenting cells with receptors from the family of CD28 receptors on the surface of T lymphocytes are crucial signals for T-cell activation (48). For example, the interaction of B7-1 with CD28 leads to T-cell activation, whereas the interaction of B7-1 with CTLA-4 (another protein of the family of CD28 receptors) leads to an inhibition of the immune response.
A CTLA-4 antibody (ipilimumab) used in the treatment of malignant melanomas prevents the binding of CTLA-4 to B7 and can thus induce an immune response against the tumor cells. The proteins PD-L1 and PD-L2 also belong to the B7 protein family. The interaction of these 2 proteins with the PD-1 receptor (a CD28 receptor) on lymphocytes inhibits the immune response. PD-1 and PD-L1 antibodies (pembrolizumab, nivolumab, and atezolizumab) block this interaction and can also trigger an immune response against tumor cells. These so-called checkpoint inhibitors have been approved in recent years for the treatment of several tumor entities such as non–small cell lung cancer, melanoma, head and neck cancer, and others.
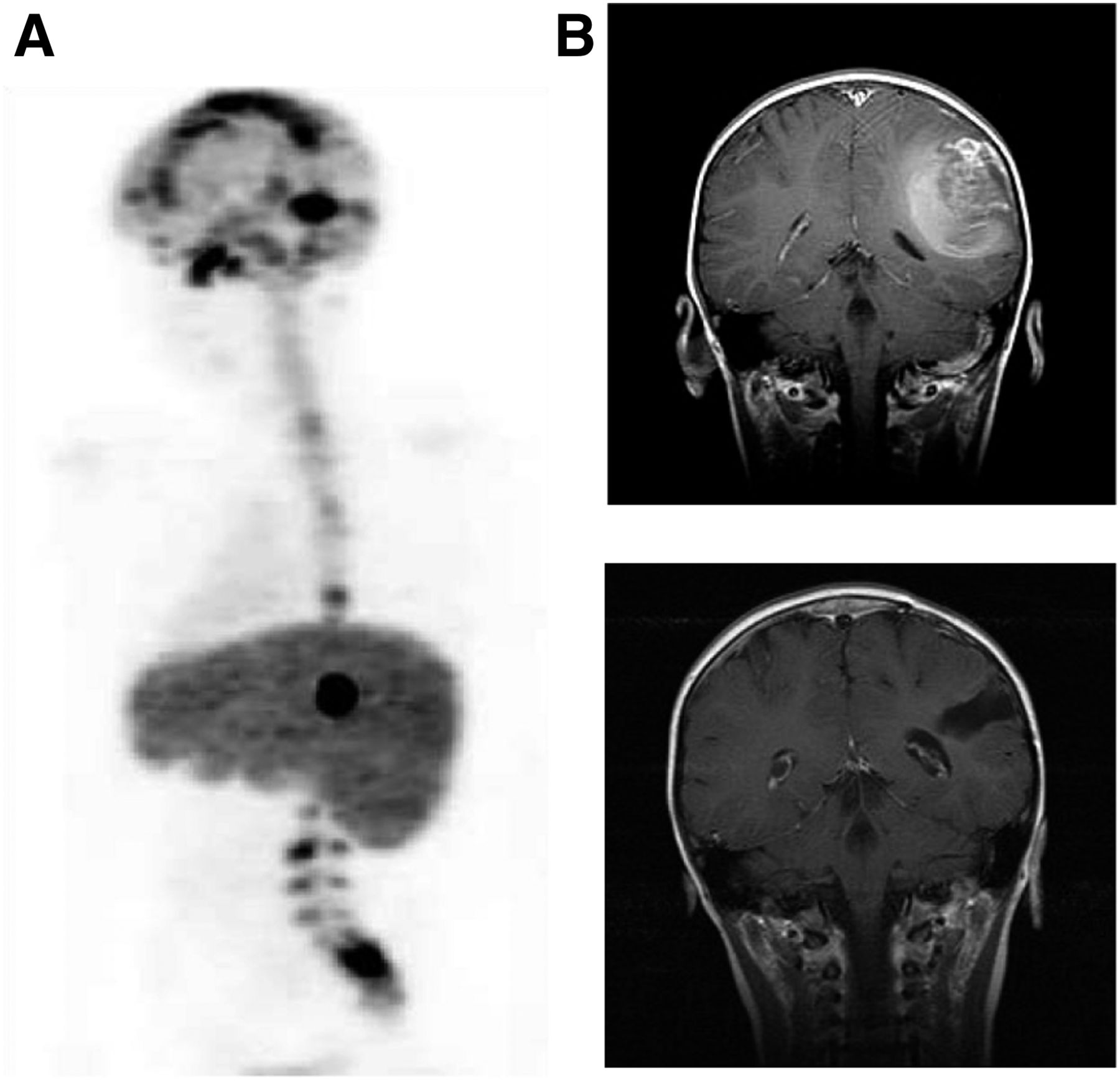
B7-H3 is overexpressed by numerous tumors (including neuroblastomas, melanomas, gliomas, and pancreatic, breast, and ovarian cancers), whereas expression in normal tissues is low (49). High expression of B7-H3 is associated with a poor prognosis in various malignant diseases (48). Omburtamab (8H9) is a murine IgG1 antibody against B7-H3 (49). After labeling with 131I, omburtamab was tested in patients with involvement of the central nervous system by neuroblastomas as well as for intratumoral therapy of brain stem gliomas (Fig. 6) (50–52).
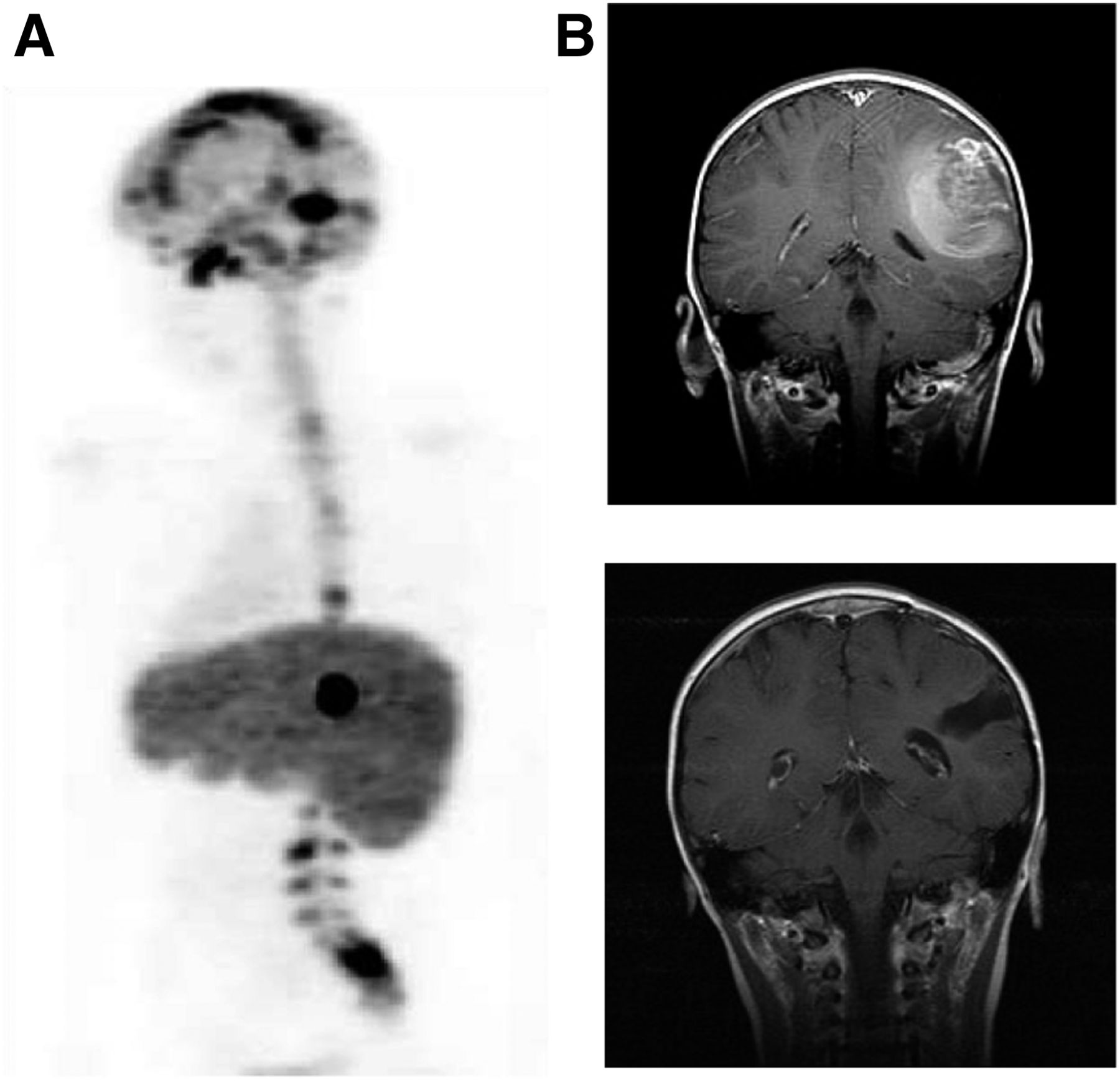
B7-H3 protein used as molecular target in treatment of neuroblastomas with cerebral metastases. (A) Distribution of 131I-labeled B7-H3 antibody omburtamab (8H9) 48 h after injection via Ommaya reservoir. (B) Coronary MRI of patient with recurrent leptomeningeal neuroblastoma before (top) and after (bottom) combined treatment with resection, external radiotherapy, and therapy with omburtamab. Patient showed no evidence of tumor progression more than 68 mo after therapy. (Reprinted with permission of (51).)
In a prospective phase I/II study of 80 patients with neuroblastoma of the central nervous system, median overall survival after intrathecal therapy with 131I-omburtamab was 58 mo and thus almost 10 times longer than reported for existing therapies (external radiotherapy or surgery combined with chemotherapy). Twenty-nine percent of the patients survived for 5 y or more. Therefore, it seems possible to cure a significant fraction of neuroblastoma patients with central nervous system involvement (52), which so far has been almost universally fatal. The rate of central nervous system side effects of intrathecal 131I-omburtamab was low, probably because of the short range of the β-radiation of 131I. An international phase II/III study is currently recruiting patients (NCT03275402).
CA19-9/HuMab-5B1 Antibody
CA19-9 (carbohydrate antigen 19-9 or cancer antigen 19-9 or sialyted Lewis A antigen) is a well-established tumor marker for pancreatic carcinoma (53). CA19-9 is a tetrasaccharide (54) and part of glycoproteins and glycolipids on the surface of tumor cells (53). In addition to pancreatic carcinomas, cholangiocellular, hepatocellular, gastric, colorectal, and breast carcinomas also produce CA19-9. Although CA19-9 is secreted, it is still an interesting target structure for molecular imaging and therapy, as the concentration is significantly higher in tumor tissue than in serum, and a CA19-9 ligand can therefore accumulate in the tumor tissue (55).
CA19-9HuMab-5B1 is a human IgG1 antibody that binds to C19-9 with a high affinity (dissociation constant, 0.14 nM) and is internalized by tumor cells. The binding is specific for C19-9, without cross-reactivity to similar saccharides such as Lewis A, Lewis X, and Lewis Y (56). In preclinical studies (Fig. 7A), an intense uptake of 89Zr-HuMab5B1 was seen in CA19-9–expressing tumors in mice (>100% of the injected activity per gram of tissue), resulting in high image contrast (55). A first clinical study confirmed these promising results in 12 patients with metastatic CA19-9-expressing tumors (57). Primary tumors and metastases in the CA19-9HuMab-5B1 PET/CT imaging showed high SUVs of up to 57 g/mL (Fig. 7B). In addition to the metastases detected by CT, numerous other metastases, for example, in small lymph nodes, were visualized on PET/CT.
Imaging with monoclonal antibody against tetrasaccharide CA19-9. (A) Mouse imaging with CA19-9 antibody 89Zr-5B1. Increasing uptake in tumor tissue is observed up to 120 h after injection. (Reprinted from (55).) (B) Mesenteric lymph node metastases of patient with pancreatic carcinoma. Lymph nodes with size less than 5 mm on CT (red arrows) show intense uptake of 89Zr-5B1 7 d after injection (white arrows). Color scale indicates PET images in SUV (g/mL).
Because of this high uptake, a phase I study on 177Lu-CA19-9HuMab-5B1 therapy was initiated and is currently recruiting patients (NCT02672917). The aim of the study is to determine the maximum tolerated dose of 177Lu-CA19-9HuMab-5B1, as well as the pharmacokinetics and dosimetry of 177Lu-CA19-9HuMab-5B1 (58). Preliminary data on tumor response according to RECIST and CA19-9 changes in serum level will also be registered. The study will escalate the bone marrow dose starting from 0.5 Gy (58).
CONCLUSION
This review has outlined recent developments in nuclear theranostics that have already entered the clinic, as well as currently evolving therapies for new targets. Several new therapeutic approaches based on antibodies, peptidomimetics, and small-molecule compounds have shown promising preclinical and initial clinical results. These new radiopharmaceuticals are directed against specific proteins (B7-H3) or saccharides on the surface of tumor cells (CA19-9) but also against proteins produced by tumor stroma cells (FAP). Some of the radiopharmaceuticals are specific for certain tumor diseases whereas others, such as FAPI-04, are potentially suitable for a variety of tumor entities. Besides new targets, novel dose schedules and combination treatments are being studied clinically. It is therefore likely that targeted radionuclide therapy will become an ever-increasing part of clinical nuclear medicine.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
- © 2019 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication June 4, 2019.
- Accepted for publication June 24, 2019.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- What Is Theranostics?
- What Is Theranostics?
- Intraperitoneal Pretargeted Radioimmunotherapy for Colorectal Peritoneal Carcinomatosis
- Nuclear Medicine Beyond VISION
- Ferronostics: Measuring Tumoral Ferrous Iron with PET to Predict Sensitivity to Iron-Targeted Cancer Therapies
- Mars Shot for Nuclear Medicine, Molecular Imaging, and Molecularly Targeted Radiopharmaceutical Therapy
- The Future of Nuclear Medicine, Molecular Imaging, and Theranostics
- Theranostic Targeting of CUB Domain Containing Protein 1 (CDCP1) in Pancreatic Cancer--Letter
- Digital Solid-State SPECT/CT Quantitation of Absolute 177Lu Radiotracer Concentration: In Vivo and In Vitro Validation
- Driving the Future of Nuclear Medicine