


Abstract
242407
Introduction: Long COVID is often associated with neurological symptoms, such as fatigue and cognitive impairment. Recent hypotheses propose a potential link between these symptoms and dysfunction in the glymphatic system, a brain waste clearance pathway in which cerebrospinal fluid (CSF) dynamics play a pivotal role. Various COVID-19-related factors, including inflammatory responses, blood-brain barrier disruption, and neurovascular changes, may impact the glymphatic system and CSF flow directly or indirectly. Notably, CSF clearance has been investigated by a dynamic PET study using 18F-THK5117 in the context of Alzheimer’s Disease. This study aims to investigate the impact of neurological long COVID on CSF clearance using dynamic 18F-FEPPA PET imaging, providing insights into potential glymphatic system dysfunction.
Methods: 18F-FEPPA PET/MR Data from nine subjects (3 HAB [high affinity binder], 6 MAB [mixed affinity binder]) diagnosed with neurological long COVID (LC group) and thirteen controls (4 HAB, 9 MAB) scanned before the COVID-19 outbreak (CTL group) were included in this study. All data were collected on a simultaneous PET/MR scanner (Siemens Biogrph mMR) with listmode acquisition. MPRAGE images were also used for brain parcellation. In this study, the regions of interest (ROIs) were the two lateral ventricles and the whole brain. Comparative analysis between the CTL and LC groups focused on the time interval from 3.5 min to 12.5 min which was based on the current timing frames. The following was studied: whole brain SUVmean, lateral ventricle CSF (vCSF) SUVmean, and the vCSF clearance rate defined as (SUVmean at 3.5min – SUVmean at 12.5min) / (SUVmean at 3.5min).
Results: Results are summarized in Figure 1. The LC and CTL groups had similar whole brain and vCSF tracer SUV at all specific time points, 3.5min, 5min, 8min, and 12.5min (all p-values > 0.5). However, the LC group demonstrated a close to zero and slightly negative vCSF clearance rate (mean = -0.016), in contrast to the positive clearance rate observed in the CTL group (mean = 0.1), and the difference was found to be significant (P = 0.001). Similar results were observed when using MABs only to rule out potential bias introduced by the genotypes.
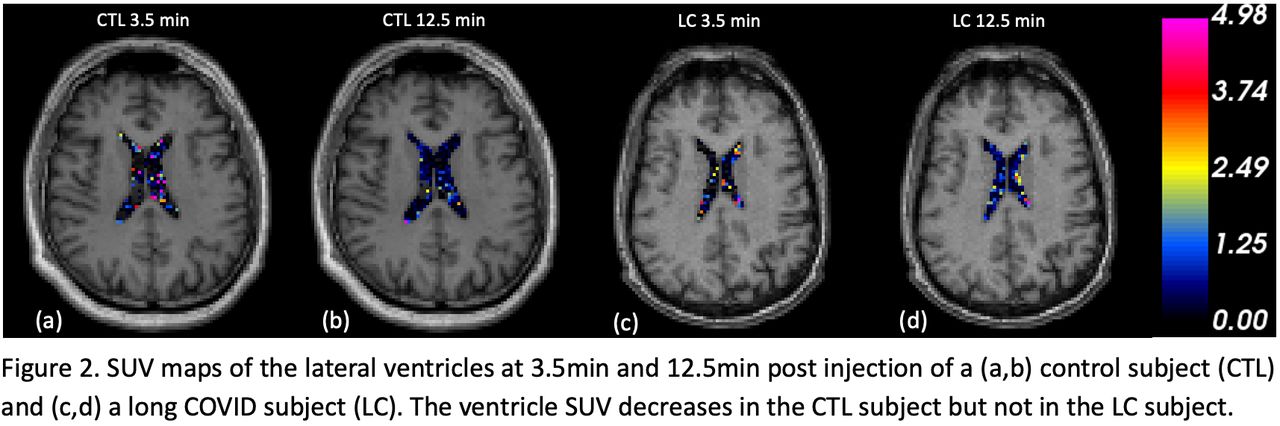
Figure 2 illustrates a representative subject from each group, highlighting the difference in vCSF clearance rates. A subject in the CTL group showed a reduction in vCSF SUV from 3.5min (Figure 2a) to 12.5min (Figure 2b), while the subject in the LC group did not show a perceivable reduction in vCSF SUV (Figure 2c,d).
Conclusions: Discussion
The reduced ventricle tracer clearance rate observed in the LC group suggests potential impairment in CSF clearance/outflow mechanisms, which could in turn contribute to glymphatic system congestion. This congestion may lead to the accumulation of toxic substances in the central nervous system and cause tauopathy, influencing neurological symptoms in long COVID patients.
Other alternative hypotheses for the observed changes include: COVID-19 is known to disrupt the blood-brain / blood-CSF barriers, which could impact tracer dynamics in the CSF; COVID-19 can induce systemic and neurological inflammatory responses, which might affect the glymphatic system's functionality or the metabolism or distribution of radiotracers in the brain. However, the whole-brain SUV was not found to be different in the two groups.
The precise mechanism of the observed reduction in CSF clearance and its dynamic interplay with the glymphatic system requires further investigation.
Conclusion
Our study demonstrates reduced lateral ventricle 18F-FEPPA CSF clearance in long COVID patients. This preliminary result provides potential evidence of glymphatic system dysfunction associated with neurological long COVID and may imply tauopathy in patients. Future research is warranted for a more comprehensive understanding of the underlying mechanism.






{kind=link}
{kind=link}