


Abstract
2424
Introduction: Prostate specific membrane antigen (PSMA) is found on prostate cancer cells and is the basis for the theranostic pairing of PSMA-based positron imaging tomography (PET) imaging and 177Lu beta-emitting therapy for PSMA-positive metastatic castration-resistant prostate cancer (mCRPC). PET imaging using or 18F PSMA-11 is performed before treatment to establish eligibility. We aim to evaluate the utility of mid treatment PSMA PET imaging for restaging and informing treatment changes.
Methods: Forty-five patients referred for 177Lu-PSMA-617 therapy who received interim PSMA PET imaging during therapy (between cycles 2 and 3 in 86% of patients) were followed for overall survival. A Medical Image Merge (MIM) post-processing workflow was used to segment tumor burden on baseline and interim PSMA PET based on an absolute standard uptake value (SUV) threshold > 4. Segmented regions of interest were categorized as physiologic or metastatic by two nuclear medicine technology students (NMTS); categorization was reviewed by a board-certified nuclear radiologist. We used conditional change Cox Regression models to evaluate the association between survival and change in SUV max, SUV mean, tumor volume, uptake volume product (UVP, mean * volume), controlled for baseline values. Tumor burden was categorized as stable with <30% change from baseline, or improved/increased with ≥30% change.
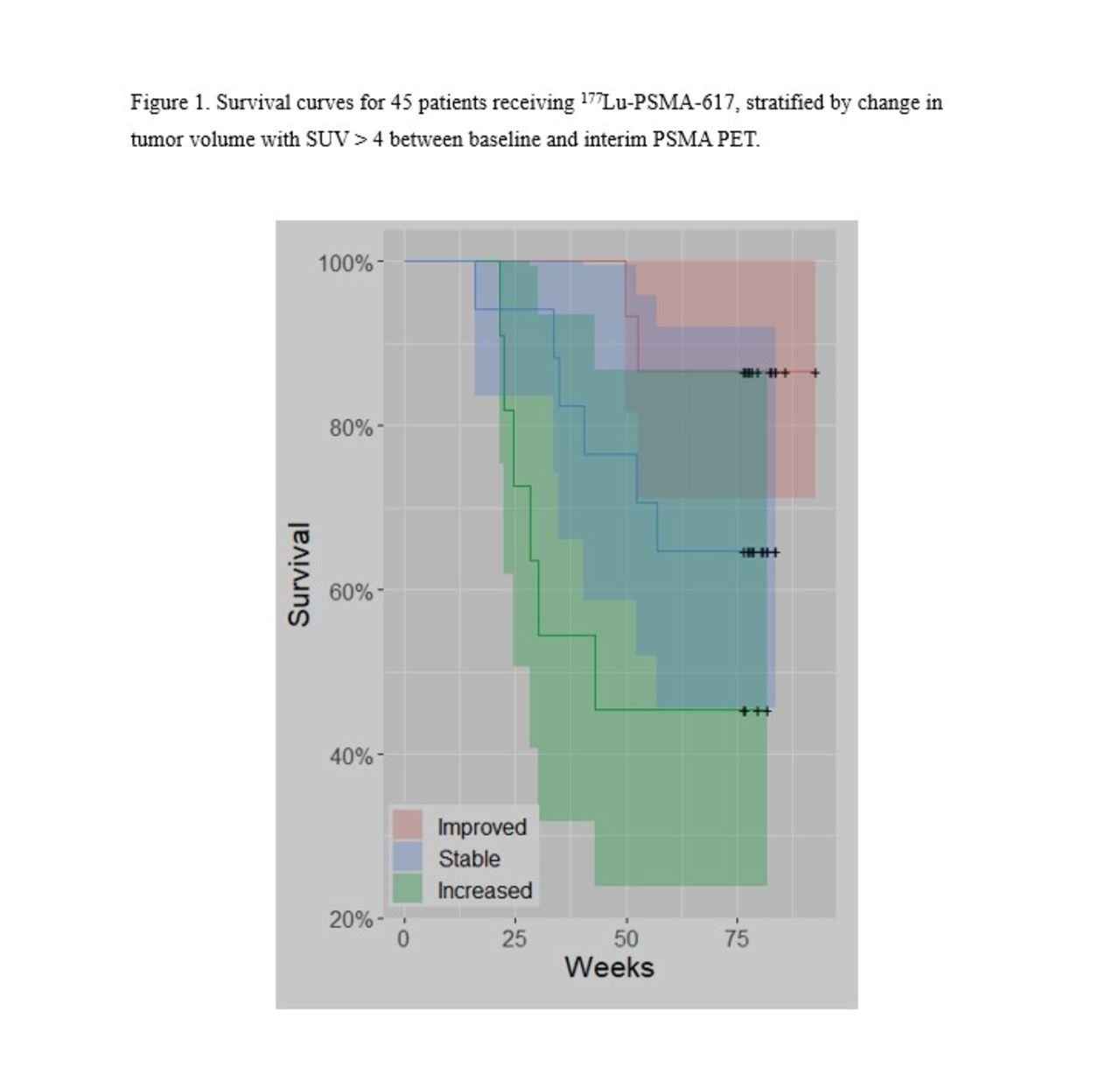
Results: Tumor burden was increased in 27% and decreased in 34% of patients on interim PSMA PET. Increased tumor volume and UVP predicted shortened survival when compared to improving disease (Figure 1, p < 0.01). Change in SUV max or mean did not predict survival. When added to the same model, volume was significant (p=0.021) while mean was not (p=0.36), suggesting the effect of UVP was driven primarily by volume. Patients with stable or improving tumor burden had similar survival outcomes (p=0.17), although median survival was not reached within the currently available follow-up interval in these groups. A one standard deviation increase in tumor volume was associated with a hazard ratio of 2.2 (p=0.002); for UVP, hazard ratio was 2.0 (p=0.002).
Conclusions: Our results suggest interim PSMA PET imaging after 2 cycles of 177Lu-PSMA-617 can detect treatment failure and prognosticate survival, supporting the utility of interim PSMA PET imaging during PSMA-based radionuclide therapy.
We did not observe a significant difference in survival between patients with stable disease vs. partial response, although median survival has not yet been reached in our cohort. While extended follow-up is needed, this early result is encouraging for patients with stable disease.
Our data also supports a growing understanding that tumor volume is more prognostic than intensity of radiotracer uptake on PSMA-based imaging. More work is needed to determine the optimal threshold for segmentation of tumor volume.

In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.