


Abstract
242323
Introduction: While rare, malignancy identified during pregnancy presents a very difficult situation to manage, requiring the interaction of obstetric and oncological experts to evaluate the choice of surgical, radiotherapy and chemotherapy treatments and compatibility with pregnancy at different gestational ages. Therefore, appropriate staging is essential to these management decisions. Positron emission tomography (PET) has become a mandatory component in initial/relapse staging and therapeutic monitoring for many cancers, however in the pregnant population the use of radiological modalities can be anxiety provoking for many physicians. Here we present our experience with use of PET in the management of maternal malignancy in pregnancy.
Methods: Retrospective chart review of pregnant patients receiving a PET -CT or -MRI for malignancy during pregnancy.
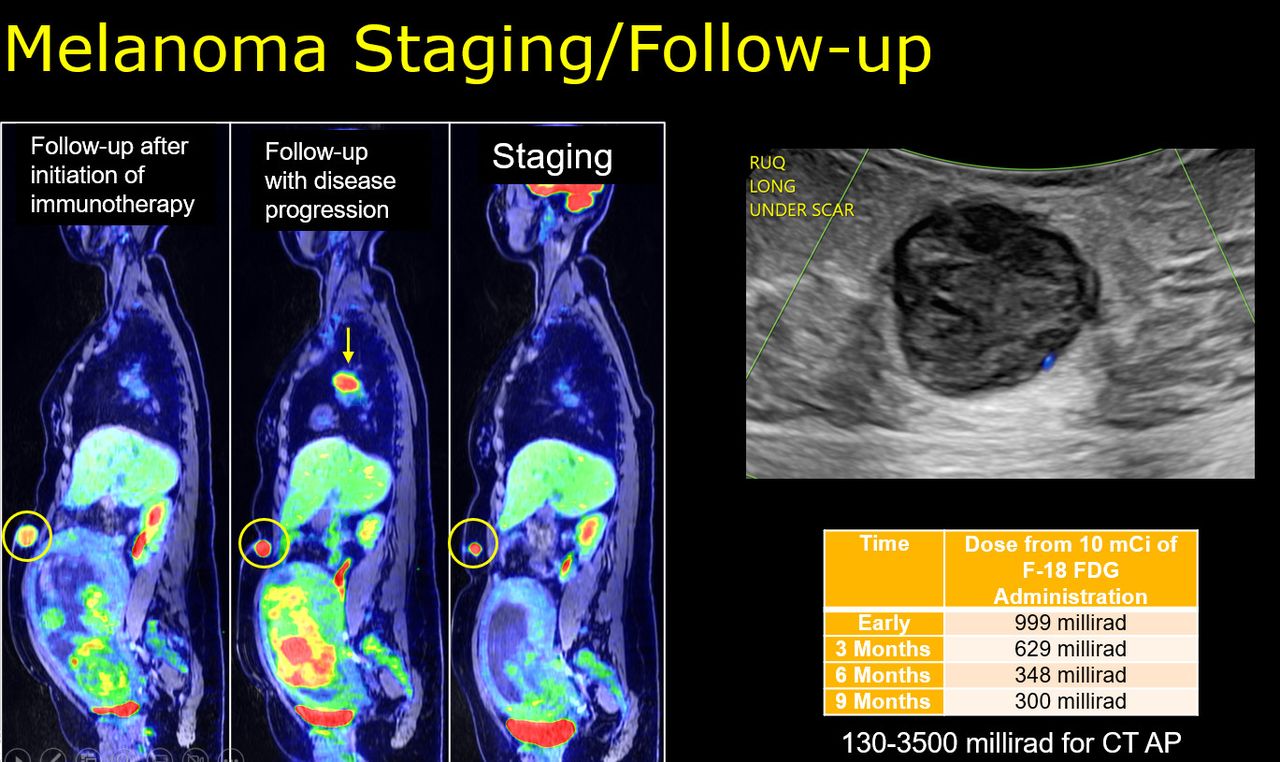
Results: In total, five cases were identified who underwent PET for malignancy during their pregnancy with management decisions by a multidisciplinary review including radiation safety, oncology, surgery, radiology, and obstetrics. Three underwent CT and two underwent MRI for anatomic co-registration and attenuation correction. PET/CT patients only had a single PET during pregnancy while the PET/MR patients each had 3 PET/MRs during pregnancy (initial staging and two subsequent for therapeutic evaluation). Malignancies included melanoma, sarcoma, pregnancy-associated breast cancer, anal squamous cell carcinoma and thymoma. Four patients were found to have malignancies during their pregnancy while the last patient became pregnant during malignancy work-up. For all cases, PET imaging played a critical role in management decisions. This included initial staging evaluation for determination of metastatic disease versus locoregional disease with three patients identified to have locoregional disease allowing for resection during pregnancy with one undergoing adjuvant therapy during the pregnancy and two with distant metastatic disease allowing for initiation of systemic therapy during pregnancy with subsequent PET/MRs for evaluation of therapeutic response. One patient was found to have progressive disease requiring change in systemic therapies. Only one patient elected to terminate the very early pregnancy, while the remaining four underwent induced term vaginal births or schedule cesarean sections. For PET/MR, the estimated absorbed dose to the fetus was calculated as 999 mrads in early pregnancy, 629 mrads at 3 months gestation, 348 mrads at 6 months, and 300 mrads at 9 months (Figure).
Example case (Figure): 34 year old G1 with history of melanoma found to have a hypoechoic mass in the anterior subcutaneous abdomen on fetal anatomic ultrasound. This was subsequently biopsied and confirmed to be a melanoma recurrence. A staging PET/MR at 22w1d demonstrated an avid recurrence in anterior subcutaneous abdomen with distant metastatic disease and elected to proceed with observation. Subsequent PET/MR showed progression of the metastases including a right hilar lymph node. The patient was then initiated on vemurafenib with subsequent PET/MR showing response to therapy. Vemurafenib was held 4 days prior to an uncomplicated cesarean section. Follow up PET/CT two weeks after birth, demonstrated marked progression of the metastatic disease highlighting the aggressive nature of this patient’s disease and how potential delay in management could have been devastating. Subsequently, the patient’s disease has been well managed with nivolumab.
Conclusions: Here we present five cases of PET in pregnancy, highlighting the critical role of PET in the evaluation of the mother’s malignancy while balancing fetal safety.

In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.