


Abstract
242299
Introduction: Head motion in brain PET studies degrades image quality and affects tracer distribution estimation. The NeuroEXPLORER (NX), a next-generation brain PET system, includes a UIH markerless motion tracking system (UMT) [1], which captures subject’s facial surface in real-time at a 30 Hz frame rate. UMT generates head motion information by registering each captured facial surface, expressed as a series of rigid transformations and utilized in event-by-event motion-corrected reconstruction. Furthermore, NX's extended axial field of view substantially improves sensitivity, facilitating the extraction of image-derived input functions (IDIF) from the carotid arteries (CA). Precise motion correction (MC) is also crucial, particularly for the lower face and neck areas, which encompass the CA. In this study, we apply a quality control method, i.e., motion-corrected centroid-of-distribution (MCCOD) [2], to evaluate the efficacy of UMT's MC across the brain, face, and neck regions.
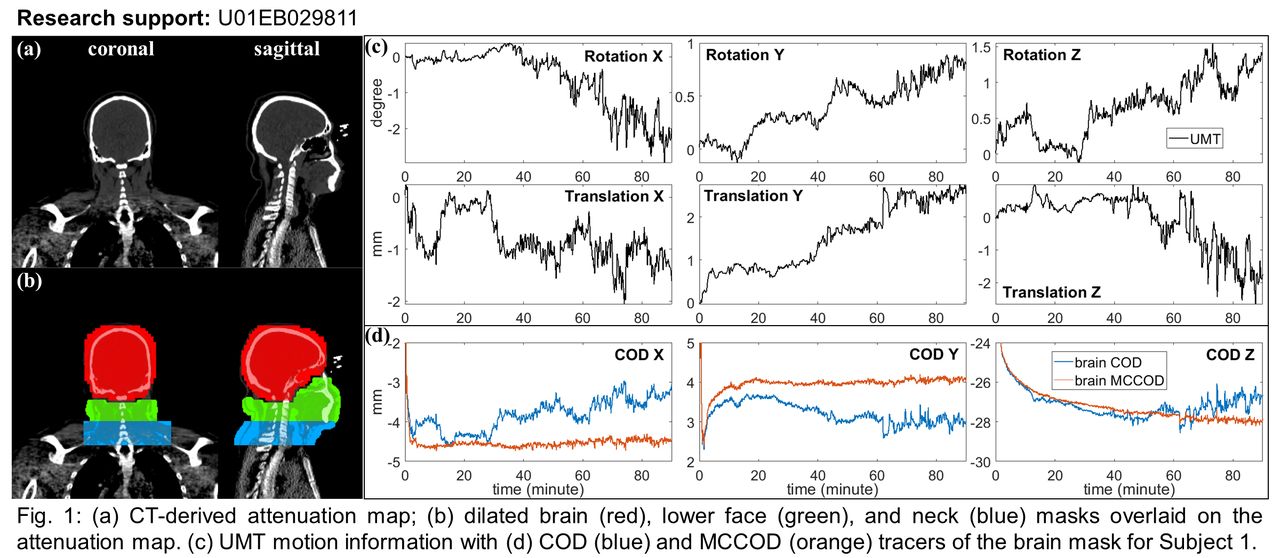
Methods: To generate MCCOD, we back-project each motion-corrected line-of-response (LOR) to the center of its TOF bin. For every 1 second, all the back-projected LORs form a "point cloud" image (PCI), serving as a surrogate of the tracer distribution after MC. A binary mask is then applied, and the centroid of the masked PCI is computed for each second to yield the MCCOD tracers. LORs are corrected for scanner geometric sensitivity. For delineating three regions of interest (ROI), i.e., brain, lower face, and neck, a deep learning model was trained to segment the brain from CT-derived attenuation maps (μ-maps) (Fig. 1a). The resulting binary brain mask undergoes dilation using morphological filtering operations (Fig. 1b, red) to encompass the entire range of head movement. The lower face and neck include the internal carotid arteries (ICA) and common carotid arteries (CCA), respectively. The neck mask is manually delineated based on the anatomical structure of the cervical vertebrae (C5-C7) and subsequently dilated (Fig. 1b, blue). The lower face mask is identified by subtracting the dilated brain mask from the cropped μ-map above the neck region, followed by its dilation (Fig. 1b, green). COD for each mask, i.e., without MC, is computed for comparative purposes. This method was applied to two 18F-FDG studies and one 18F-FE-PE2I study.
Results: The COD trace (Fig. 1d, blue) closely mirrored the recorded UMT data (Fig. 1c) of Subject 1. The relatively flat MCCOD (Fig. 1d, orange) suggests accurate MC in the brain. Subject 2 and 3 presented pronounced motions, particularly impacting the face and neck ROIs. Fig. 2a-c show MCCOD (orange) and COD (blue) tracers for three subjects. MCCODs of face and neck masks revealed large residual motions during 60-90 min. Fig. 2d-e illustrate non-MC and MC reconstructions of Subject 2 at 50-70 min post-injection. In the MC image (Fig. 2d, right), the enhanced delineation of gray matter signifies effective MC. Conversely, the blurring of CCA in the MC image (Fig. 2e, right), as compared to the non-MC image (Fig. 2e, left), indicates poorer MC. Quantitative analysis involved extracting SUV for ICA and CCA ROIs from both non-MC and MC images. The average SUV in MC is decreased by 14% for ICA and 19% for CCA compared to non-MC. This SUV reduction in the MC image suggests an activity underestimation in CA.
Conclusions: MCCOD has demonstrated its efficacy in assessing the quality of MC by UMT. The results indicate accurate MC in the brain region. However, in the lower face and neck regions, corrupted MCCODs and the observed decrease in CA quantification highlight inaccuracies in MC. The residual motions noted in MCCODs for these regions are most likely due to non-rigid motion, which is not corrected with the current UMT data. Future research aims to rectify the residual motion in the lower face and neck areas, employing MCCOD for further evaluations.


In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.