


Abstract
241907
Introduction: 99mTc-4BOH is a new radiotracer containing the 4-(hydroxymethyl)phenyl boronate cap. 99mTc-4BOH has shown rapid and stable heart uptake, which is necessary for accurate myocardial blood flow (MBF) quantitation. In this study, we investigated the optimal compartment model and acquisition protocol using dynamic 99mTc-4BOH SPECT for myocardial perfusion imaging in patients.
Methods: Our study included 25 patients with suspected or diagnosed coronary artery disease, each underwent both rest and stress dynamic cardiac 99mTc-4BOH scans on the same day using a Discovery NM 530c CZT SPECT camera (GE, USA). For each patient, in both rest and stress studies, the dynamic SPECT data were acquired for 10 minutes and reconstructed into 22 frames (10×10 s, 5 × 20 s, 6× 60 s, 1 × 40 s). Image-derived input function was created from blood pool by placing a rectangular volume of interest over left ventricular regions and atrium, and was fitted by a 3-term exponential function. Tracer kinetic modeling was performed on the myocardial time activity curve with one-tissue (1T), reversible two-tissue (2T) and irreversible two-tissue (2Ti) compartment models using weighted least squares on PMOD. The Akaike information criterion (AIC) values were calculated to identify the optimal compartment model for 99mTc-4BOH. After the optimal model was selected, the optimal acquisition protocol was also investigated to determine the shortest dynamic scan time. Correlation studies were performed between the kinetic parameters obtained from 10-min dynamic scan (the gold standard) and those obtained from different scan times (8, 6, 5 minutes, respectively).
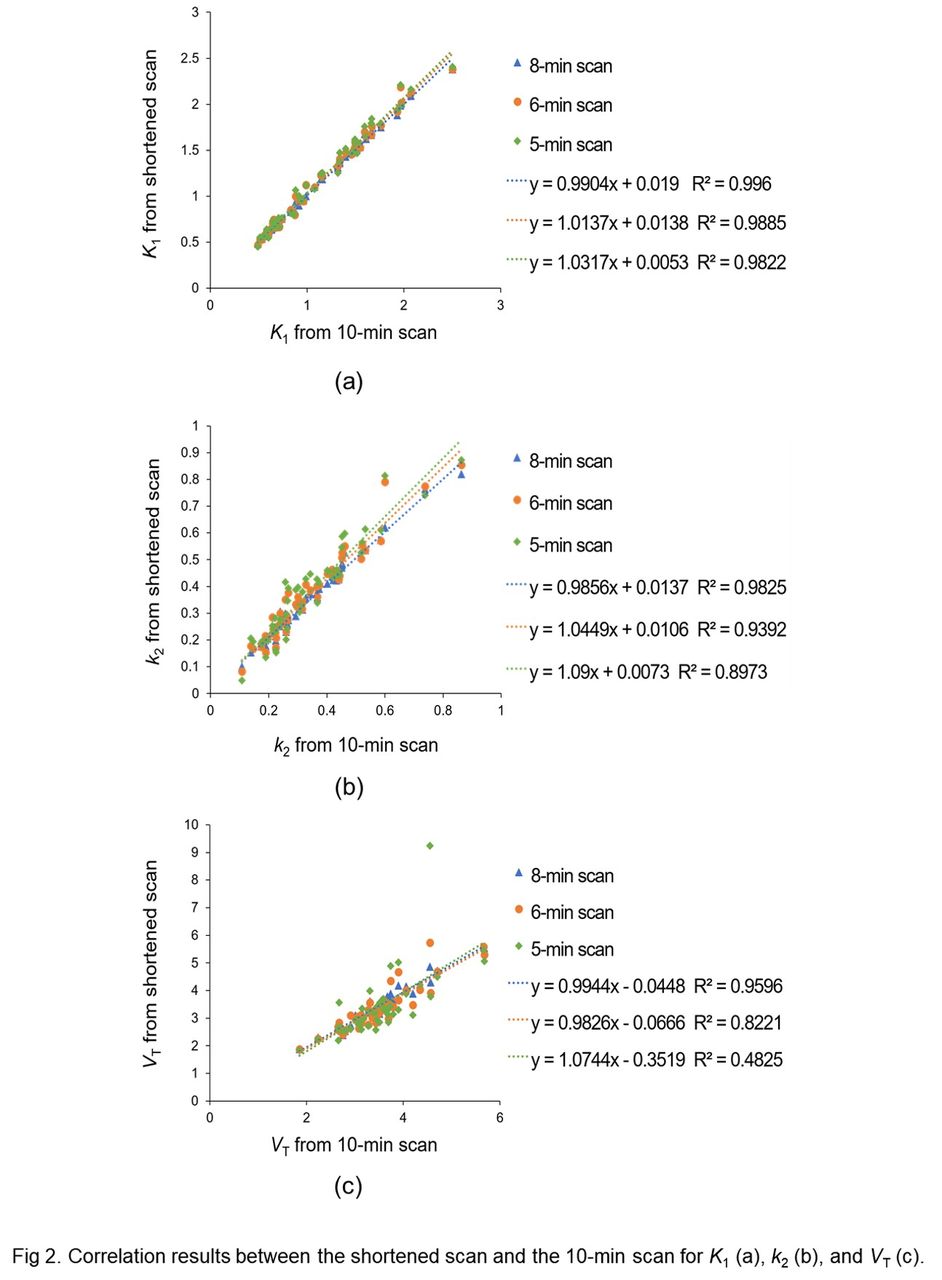
Results: For the rest and stress studies of all the 25 patients (50 studies in total), the AIC values obtained from tracer kinetic modeling using 1T, 2T and 2Ti models were 177.1±18.0, 173.4±13.3, and 174.8±15.3. Though the AIC difference was significant between 1T and 2T (p = 0.02), and between 1T and 2Ti (p = 0.02), the differences among the three AIC mean values were small. Meanwhile, the estimations for the kinetic parameters were more stable and reliable with 1T than those with 2T and 2Ti. With 1T model, the relative standard errors of the estimates for both K1 and k2 across all the studies were within 13%. With 2T model, the relative standard errors were larger than 50% in 15 studies for K1, in 20 studies for k2, in 27 studies for k3, and in 22 studies for k4. With 2Ti model, the relative standard errors were larger than 50% in 28 studies for k3. Based on these observations, 1T was selected as the optimal compartment model for 99mTc-4BOH. Using 1T model, the R2 values obtained from the correlation studies between 10-min dynamic scan (the gold standard) and 8-min scan were 0.996 for K1, 0.983 for k2, and 0.960 for VT; while the R2 values between 10-min dynamic scan and 6-min scan were 0.989 for K1, 0.939 for k2, and 0.822 for VT; while the R2 values between 10-min dynamic scan and 5-min scan were 0.982 for K1, 0.897 for k2, and 0.483 for VT. These results indicated that the dynamic acquisition time for 99mTc-4BOH can be shortened to 8 minutes when all the kinetic parameters (K1, k2 and VT) are of interest, while the dynamic acquisition time can further be shortened to 5 minutes when only the kinetic parameter of K1 is of interest for myocardial perfusion imaging.
Conclusions: In this work, the feasibility study of dynamic 99mTc-4BOH SPECT was performed for myocardial perfusion imaging in patients. 1T can be selected as the optimal compartment model for 99mTc-4BOH. A 5-min dynamic scan could be enough to obtain reliable K1 value for myocardial perfusion imaging.


In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.