


Abstract
241782
Introduction: • Mention the role of Target to background ratio(TBR) in atherosclerosis FDG-PET Imaging.
• Evaluate the accuracy of the TBR correction method in FDG-PET imaging for atherosclerosis.
• Exploring alternative quantitative approaches to TBR for atherosclerosis assessment using FDG-PET imaging
Methods: Utilizing PubMed, Scopus, and Web of Science, this review comprehensively surveyed existing literature on the use and challenges of target-to-background ratio (TBR) in FDG-PET imaging for atherosclerosis. Studies focusing on the quantification methods, particularly the accuracy and reliability of TBR correction, were analyzed. The results of these studies were synthesized to address limitations and potential areas for future investigation.
Results: The introduction of Target to Background Ratio (TBR) for PET imaging of atherosclerosis presented a promising approach to isolate and quantify inflammation activity within arterial wall plaques. By calculating the ratio of the signal intensity of an atherosclerotic plaque to the surrounding background tissue, TBR aimed to correct for confounding residual tracer amounts circulating post-injection, enhancing lesion detectability, quantifying plaque inflammation, and aiding risk stratification.
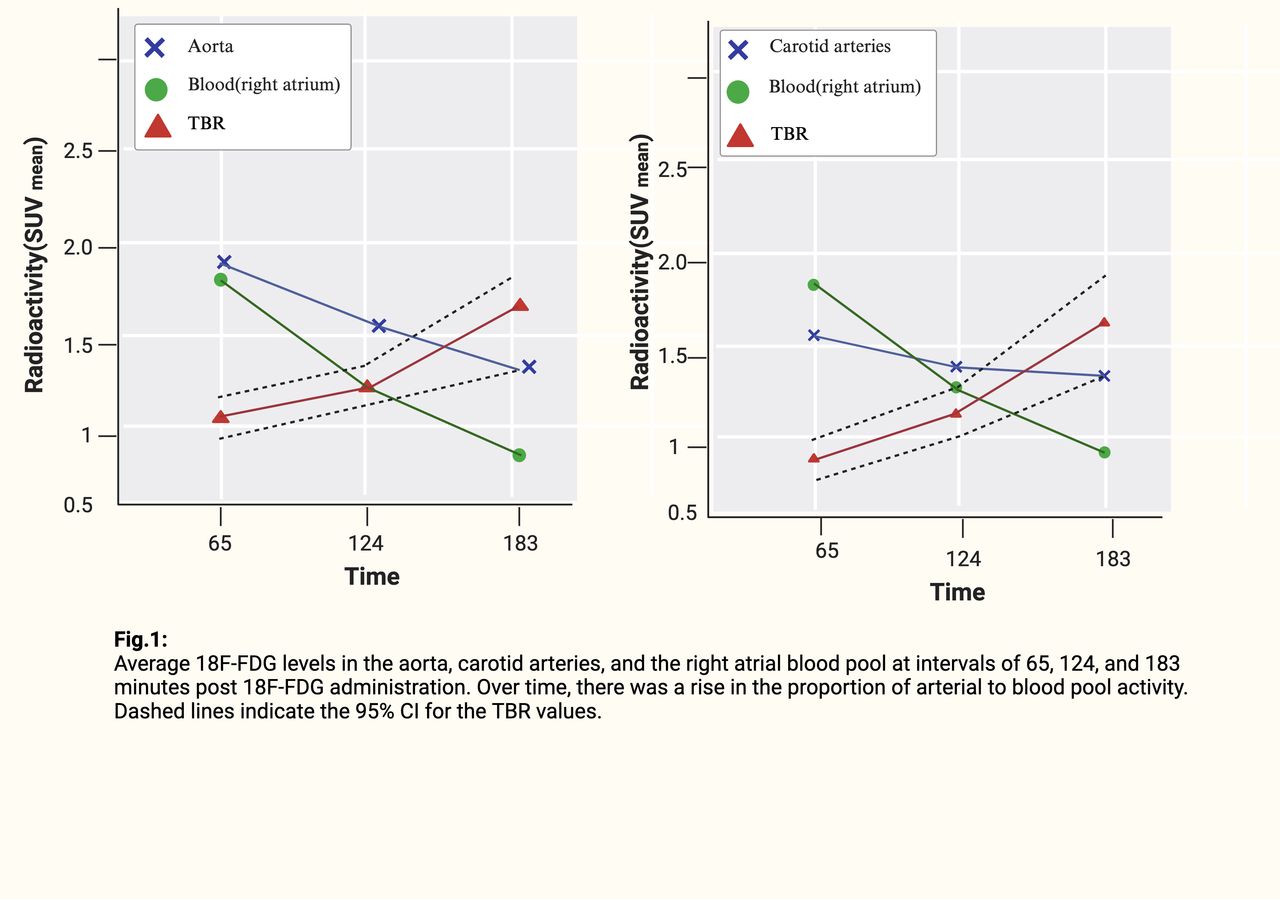
However, the accuracy of the TBR method in FDG-PET imaging depends on several variables that need to be accounted for. Studies tell us that the scan timing 1 to 3 hours after injection shows inconsistent TBR values, casting doubt on their ability to measure plaque inflammation precisely. Optimal imaging time is 3-4 hours post-injection when FDG clearance diminish the need for TBR correction. This temporal dependency introduces considerable variability and potential for quantification errors. Another challenge that presents variations in plaque quantification is the nonspecific nature of FDG; uptake in the heart and smooth muscles of the arterial wall precludes plaque detection in the coronary arteries, posing false positive errors. Additionally, the small size of target arteries hinders accurate blood pool activity measurement, the denominator in TBR calculation. This method may inadvertently amplify errors rather than isolate the artery wall signal, conflicting with TBR's premise of correcting for blood activity, particularly considering known partial volume effect behaviors in PET imaging.
In light of these limitations, the utilization of plaque-specific tracers like 18F-sodium fluoride offers a more promising avenue. This tracer effectively sidesteps spillover issues and cardiac muscle interference, facilitating a more direct and interference-free quantification process in the full arterial system. With its rapid clearance from circulation, the need for problematic blood pool measurement is avoided, presenting a significant advantage over the conventional FDG tracers.
Consequently, a departure from the application of problematic TBR corrections becomes apparent, as evolving PET techniques may circumvent the constraints that necessitate such inaccurate workarounds. This shift in perspective reinforces arguments against relying on TBR measures for precise plaque quantification, urging the inflammation imaging community to acknowledge and embrace this evolving mindset. The next logical step involves the collaborative development of improved FDG-PET methodologies and next-generation platforms for atherosclerosis assessment, capitalizing on the advancements offered by alternative tracers and PET technologies.
Conclusions: There is a growing consensus for reevaluating the use of TBR in PET imaging, advocating for methodologies that address these accuracy and practicality concerns, thereby guiding future research and clinical practices towards more reliable diagnostic techniques.

In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.