


Abstract
241574
Introduction: An aetiological link between gastro-oesophageal reflux disease (GORD) and respiratory disease has been purported but not established. The pulmonary manifestations of GORD and management of these have not been closely investigated. Chronic micro-aspiration leading to airway irritation, lung injury and respiratory tree remodelling may be implicated in the pathophysiology and progression of lung fibrosis and bronchiectasis.
A new scintigraphic technique incorporating SPECT/ CT has shown that patients with severe GORD also demonstrate pulmonary micro-aspiration (PMA) of refluxate. We hypothesise that sites of PMA correlate with the anatomical distribution of changes such as fibrosis, scarring, bronchiectasis and ground glass changes on high-resolution CT (HRCT).
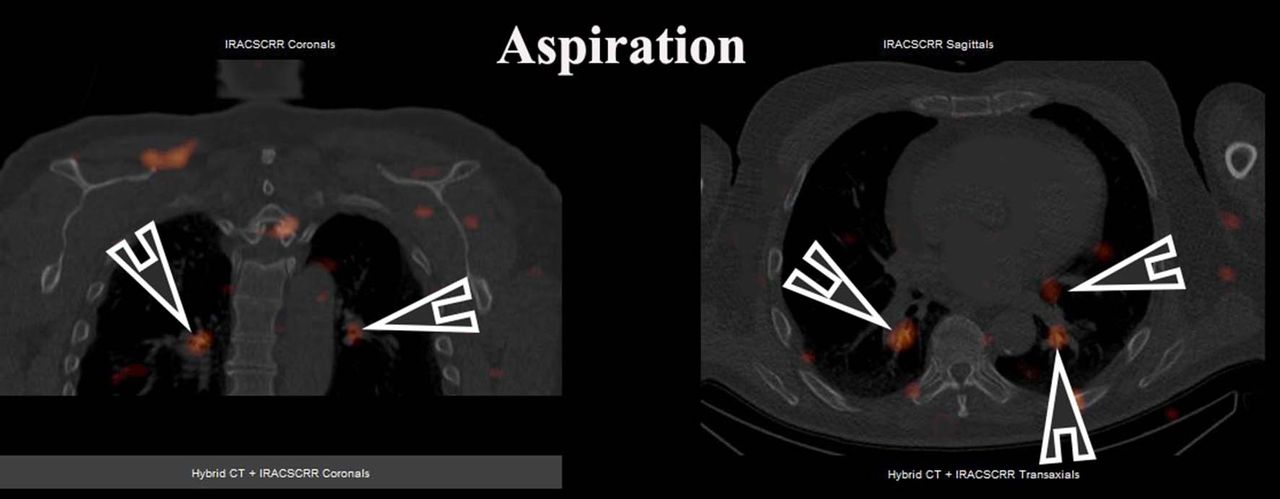
Methods: Retrospective data was obtained from patients who underwent oesophageal scintigraphic reflux studies at a single nuclear medicine imaging centre to evaluate the possibility of significant GORD or extra-oesophageal symptoms. Patients were scanned after the administration of oral 99m-Technetium Fyton with early planar dynamic and delayed SPECT/ CT images of the lungs to evaluate GORD and PMA.
Results: Evidence of PMA was found in 113 patients and 34 of these patients also underwent HRCT. Of these, 21 patients demonstrated CT changes indicative of pulmonary disease (14 female, 7 males, Mean age 69.0 years). Eleven showed evidence of pulmonary fibrosis or scarring, 10 showed evidence of bronchiectasis and 5 showed evidence of ground glass changes (1 demonstrated both fibrosis and ground glass change, 2 demonstrated both scarring and bronchiectasis and 1 demonstrated both bronchiectasis and ground glass change). All 21 patients had full column GOR in both upright and supine positions with evidence of PMA in the lungs. In the patients demonstrating fibrosis and scarring of the lungs, 10 of 11 showed CT findings with anatomical correlation to the site of PMA. Bronchiectasis was found co-located in 9 of 10 patients. The 13 other patients had normal reports in 5 and the remainder had other pulmonary pathology such as atelectasis, emphysematous changes or evidence of lung nodules.
Conclusions: The provisional results from this study<s> </s>demonstrate a probable relationship between GORD and a spectrum of respiratory diseases such as fibrosis and bronchiectasis. Whilst a causal association between these pathologies has not been proven, these findings indicate that the current clinical paradigm of GORD and respiratory disease being two separate entities should be re-evaluated.

In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.