


Abstract
241496
Introduction: The initial staging and subsequent post-therapeutic monitoring of prostate cancer are presently supported by the more accurate Prostate Specific Membrane Antigen (PSMA)-labeled radiopharmaceuticals. These radiotracers are represented by F-18 PSMA, mostly used in the community radiology centers, and by Ga-68 PSMA at institutions possessing a cyclotron. In prostate adenocarcinoma, there is an overexpression of PSMA, a type II transmembrane glycoprotein also known as glutamate carboxypeptidase II in the central nervous system, with a high correlation with the PSA serum levels. However, PSMA is also expressed in endothelial cells of neovasculature from a variety of tumors and non-neoplastic processes. The latter entities include vascular proliferation in the endometrium, and regenerative and reparative conditions such as granulation tissue and scarring. Consequently, radiologists and nuclear medicine physicians may encounter the tracer-avid benign and malignant non-prostatic pathologic processes during the interpretation of PSMA PET/CT imaging.
Methods: 1. To familiarize the viewers with the biodistribution and normal variant features of uptake of PSMA-labelled radiotracers.
2. To present the spectrum of tracer-avid non-prostatic benign and malignant processes mimicking metastasis from prostate cancer.
Results: This poster exhibit has three components:
1. The presentation of normal biodistribution of PSMA-tagged radiopharmaceuticals with potential pitfalls of uptake features from the sympathetic chain ganglion and less frequently from the gallbladder.
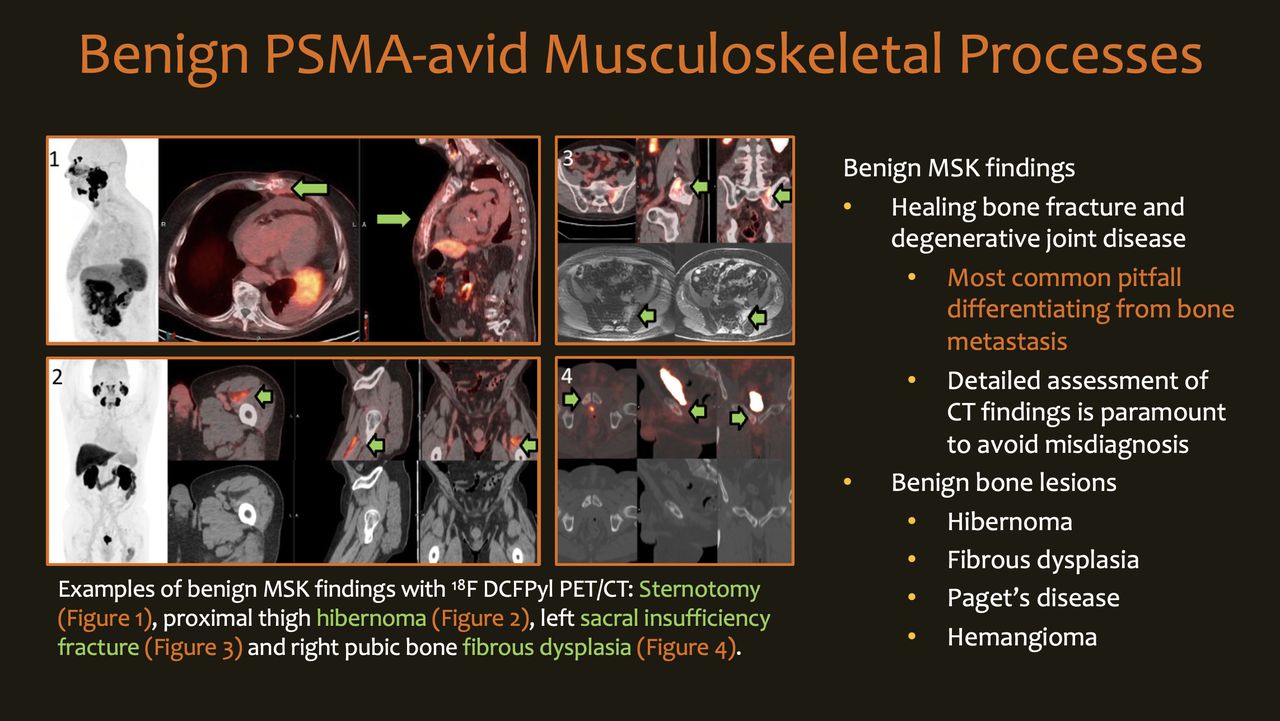
2. The review of benign pathologic entities with PSMA uptake including healing fractures, fibrous dysplasia, hibernoma, splenic hemangiomas, intra-pancreatic spleen, keloids, and inflammation and infection of different organs of the body.
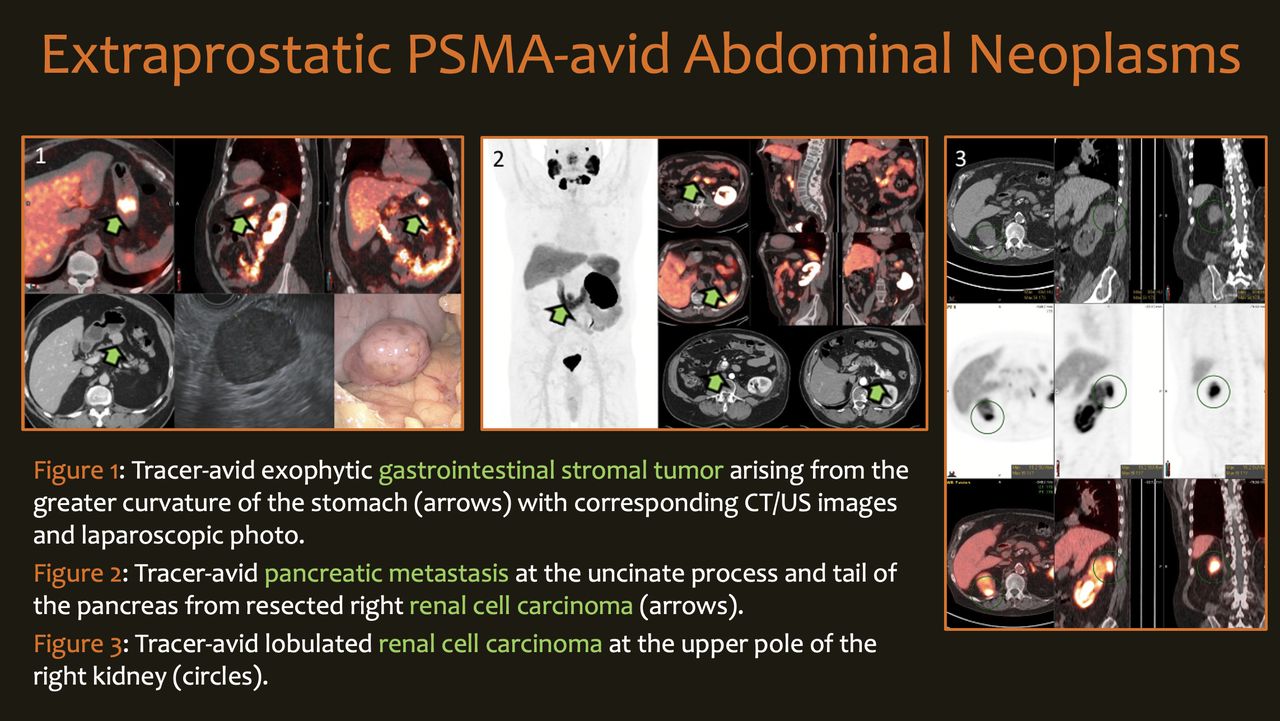
3. The review of malignant processes mimicking metastasis from prostate cancer such as lung cancer, squamous cell carcinoma of the head and neck, glioblastoma, thyroid carcinoma, esophageal carcinoma, gastrointestinal stromal tumor, renal cell carcinoma, colon cancer and multiple myeloma.
Conclusions: The viewers will be familiar with the differential diagnosis of PSMA-avid features on PET/CT based on their location and features as seen using transmission CT/MR and contemporary cross-sectional imaging.


In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.