


Abstract
241118
Introduction: Psoriatic arthritis (PsA) is a heterogeneous disease that may affect one or multiple clinical domains, that include peripheral arthritis, enthesitis, dactylitis, spondyloarthritis, and nail and skin. Clinical examination alone is not adequately sensitive, especially with the complex anatomical accessibility of these domains. Other imaging modalities like MRI and ultrasound, though having more established diagnostic criteria, may not provide a comprehensive total-body evaluation, essential to evaluate these domains. We aimed to explore the capabilities of the total-body PET/CT (TB-PET/CT) for providing quantitative, domain-specific evaluation of the inflammatory burden in PsA.
Methods: Twenty-four participants (median age: 47.8, range: 28.3-77.4 years) with PsA underwent low-dose TB-PET/CT scans using 78.8±4.7 MBq [18F]FDG. Single bed acquisition was obtained for 20 minutes, starting at 40min post-injection. Scans were assessed qualitatively (on a four-point ordinal scale, 0-3, with score 2 considered positive) and quantitatively for any finding scored 1 or more (using rSUVmax, measured as SUVmax of the finding, normalized by ascending aorta blood pool SUVmean). PET evaluations included 68 joints, 38 entheses, 20 nails, spine and sacroiliac joints, and dactylitis. Rheumatologic examination was performed independently prior to the scan and included disease activity in psoriatic arthritis (DAPSA) evaluation of the 68 joints, Leeds Enthesitis Index (LEI), and Nail Psoriasis Severity Index (NAPSI), in addition to clinical evaluation of inflammatory back pain and evaluation of dactylitis using Leeds Dactylitis Index (LDI).
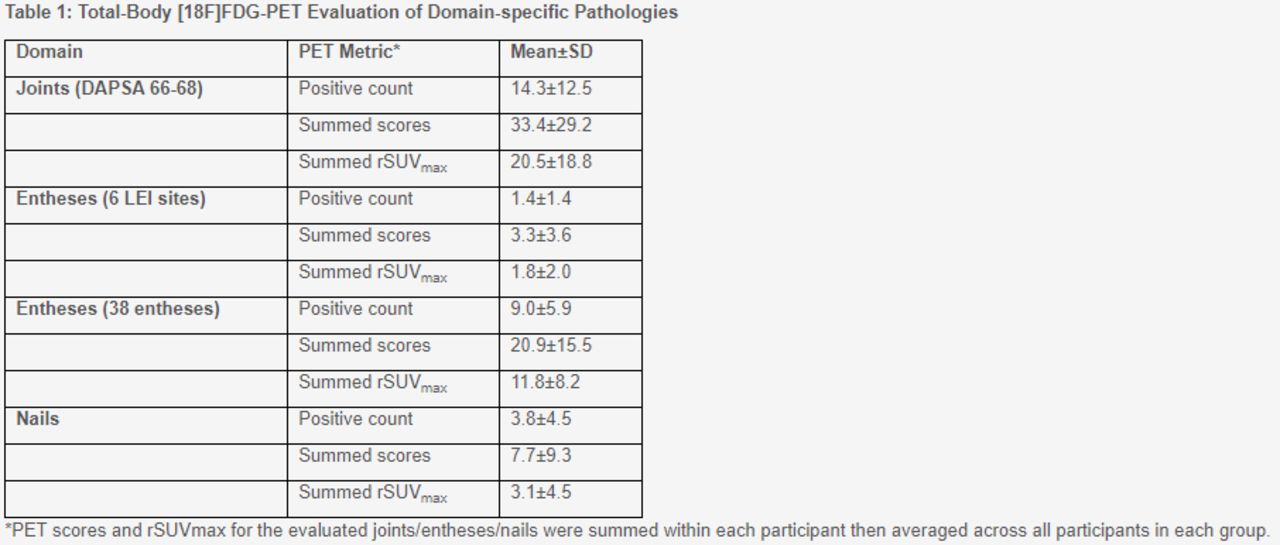
Results: Joint involvement and enthesitis were noted in all patients. Findings included distal interphalangeal joint and extensor tendon involvement (Figure 1). Other features (Figure 2) included nail matrix pathology (n=14), spinal involvement (n=18), active sacroiliitis (n=4) and dactylitis (n=3). There was a high concordance between TB-PET measures and the domain-specific clinical assessment of joint (75%), entheseal (78%) and nail (72%) pathologies. TB-PET was positive for an additional 16% joints, 20% entheses and 13% nails that were negative on clinical assessments (Figure 1). The majority of joints that exhibited clinical positivity but were PET-negative showed tenderness without any swelling (136/149 [91%]). Quantification of the different PET metrics is demonstrated in Table 1.
Table 1: Total-Body [18F]FDG-PET Evaluation of Domain-specific Pathologies
*PET scores and rSUVmax for the evaluated joints/entheses/nails were summed within each participant then averaged across all participants in each group.
Conclusions: TB-PET/CT identified domain pathologies in PsA patients, some of which were occult on clinical examination and could represent a promising quantitative tool for in vivo comprehensive evaluation of total inflammatory burden of PsA, towards early PsA disease assessment or monitoring/stratification of therapeutic response.



In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.