


Abstract
TS21
Introduction: The linear no-threshold (LNT) dose response curve states radiation workers should be cautious of increases in exposure as it is directly proportional to the probability of adverse effects.1 Currently of all radiation workers monitored for occupational exposure (OE), those who perform PET/CT imaging have exposure rates closer to ALARA limits.5 Theranostics has the potential to add higher OE to Nuclear Medicine Technologists (NMT).4 New therapies use Lutetium 177 (Lu177), a beta emitter with gamma component, to target tumors. Lu177 agents use sequential treatments with dosages around 200mCi per treatment.2,3 It is important to analyze OE patterns when assigning roles in the growing field of theranostics. The purpose of this study is to quantify the OE received by a NMT who is administering Lu177 versus NMTs at the same site who do not administer Lu177. This research is a single site study on OE to NMTs when adding Lu177 therapies to a general NM workload
Methods: The monthly dosimetry reports from 3 different NMT roles during 6/1/2021-6/30/2022 were utilized. These include general NMTs who did not administer Lu177 or PET radiotracers (NMT1); general NMTs who administered Lu177 therapy agents, general NM radiotracers, and not PET radiotracers (NMT2); and a NMT that administered PET radiotracers (NMT3). During this time span, NMT1 or NMT2 handled on average 167 doses/month with 3.7 Ci/month; NMT3 had on average 114 doses/month with 1.2Ci/month. The average exposure for the dominant hand and whole body (WB) was calculated using readings from Mirion TLD ring dosimeters and film badges. The Lu177 doses given each month were compared to the average OE of NMT2. A comparison was made between the NMTs OE, and the impact that individual patient doses had on the NMTs OEs to identify any differences in OE from adding Lu 177 therapies to existing workload.
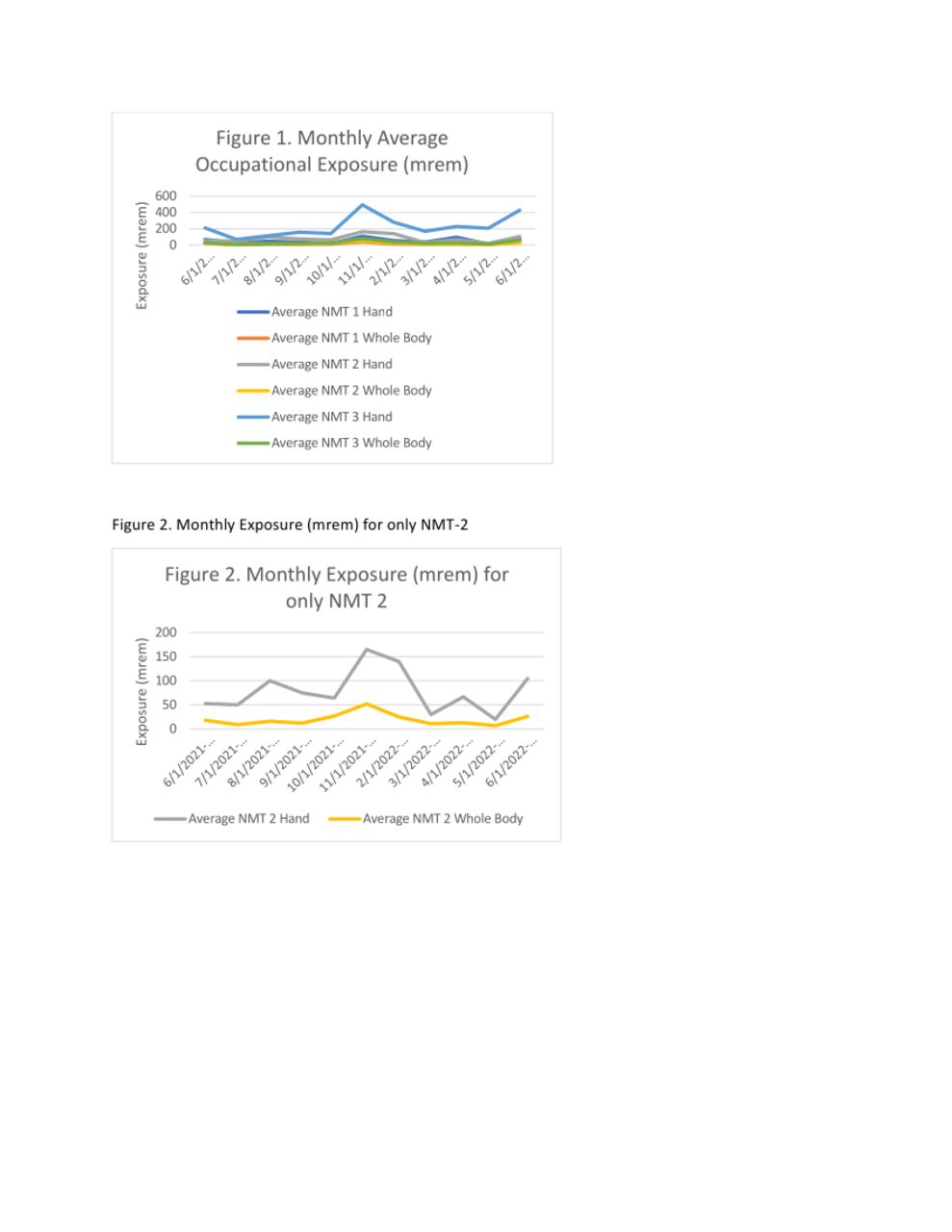
Results: From the dosimetry reports, two NMTs were categorized as NMT1s, one categorized as NMT2, and three NMTs categorized as NMT3 (Table 1). The overall mean radiation exposures were calculated for the WB and dominant hand exposures of the groups. NMT1 had a WB exposure of 18mrem and a hand exposure of 52.5mrem. NMT2 received 19.6mrem and 79mrem to WB and dominant hand respectively. NMT-3 received 31.9mrem WB and 228mrem to the hand (Table 2). The data was organized into monthly averages for each group for hand and WB, and then were compared via graph (Table 3; Fig. 1). The monthly average dose activity that NMT2 administered was compared with the monthly exposure received. NMT2 administered 9 Lu177 doses with a monthly average of 127.7mCi (Table 4; Fig. 2).
Conclusions: When comparing NMT2’s averages to NMT1, a difference was seen in WB exposure, but a larger difference was seen when comparing dominant hand exposure. When comparing both groups to NMT3, NMT3 received a significantly higher OE for both WB and dominant hand (Table 2), which is expected for this role. The monthly averages for each group were also calculated and graphed. The overall trends showed that NMT3>NMT2>NMT1 for both hand and WB OE (Fig. 1). On average, NMTs that perform PET/CT imaging received the highest OE with NMT2 who administered Lu177 therapies having a slightly higher exposure than NMT1 who did not administer these therapy agents. The amount of Lu177 given each month in mCi was compared to NMT2’s monthly averages. This comparison did not indicate a correlation between activity of dose and OE (Table 4; Fig. 2). These results may indicate that in facilities where PET technologist roles are not rotated, it may be beneficial to assign Lu177 administration roles to general NMTs. Gathering additional data from higher Lu177 therapy volume facilities and analyzing workflow, as well as radiation safety practices could help clarify Lu177 administration’s contribution to OE. Further research could explore different ways for departments to rotate roles if they are considering implementing a Lu177 theranostics program.


In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.