


Abstract
P94
Introduction: Waldenström macroglobulinemia(WM), an indolent B-cell lymphoma, is preceded by a precursory asymptomatic stage known as smoldering WM(sWM). Sometimes it is challenging to differentiate WM from sWM according to symptoms.We wonder whether 68Ga-pentixafor PET/CT targeted at CXCR4 can differentiate sWM from WM.
Methods: This is a retrospective study. 68Ga-pentixafor PET/CT was performed at baseline. Semi-quantitative parameters of tumor burden were measured as total lesion volume (TLV, the sum of the volumes of all CXCR4 positive tumor lesions) and total lesions uptake(TLU, the sum of individual TLV multiplied by its mean SUV).
Results: Clinical characteristics
37 patients with newly diagnosed WM and 11 sWM patients(35 M and 13 F; 64.3±10.7y) were analyzed in the present study. The clinical characteristics were compared between patients with WM and sWM(Table 1). Patients with WM had significantly lower levels of Hb and albumin than sWM patients did. β2-MG, IgM and M protein in WM patients were significantly higher than those in sWM patients. No significant difference was found in other laboratory examination results between patients with WM and patients with sWM.
68Ga-pentixafor PET/CT presentation
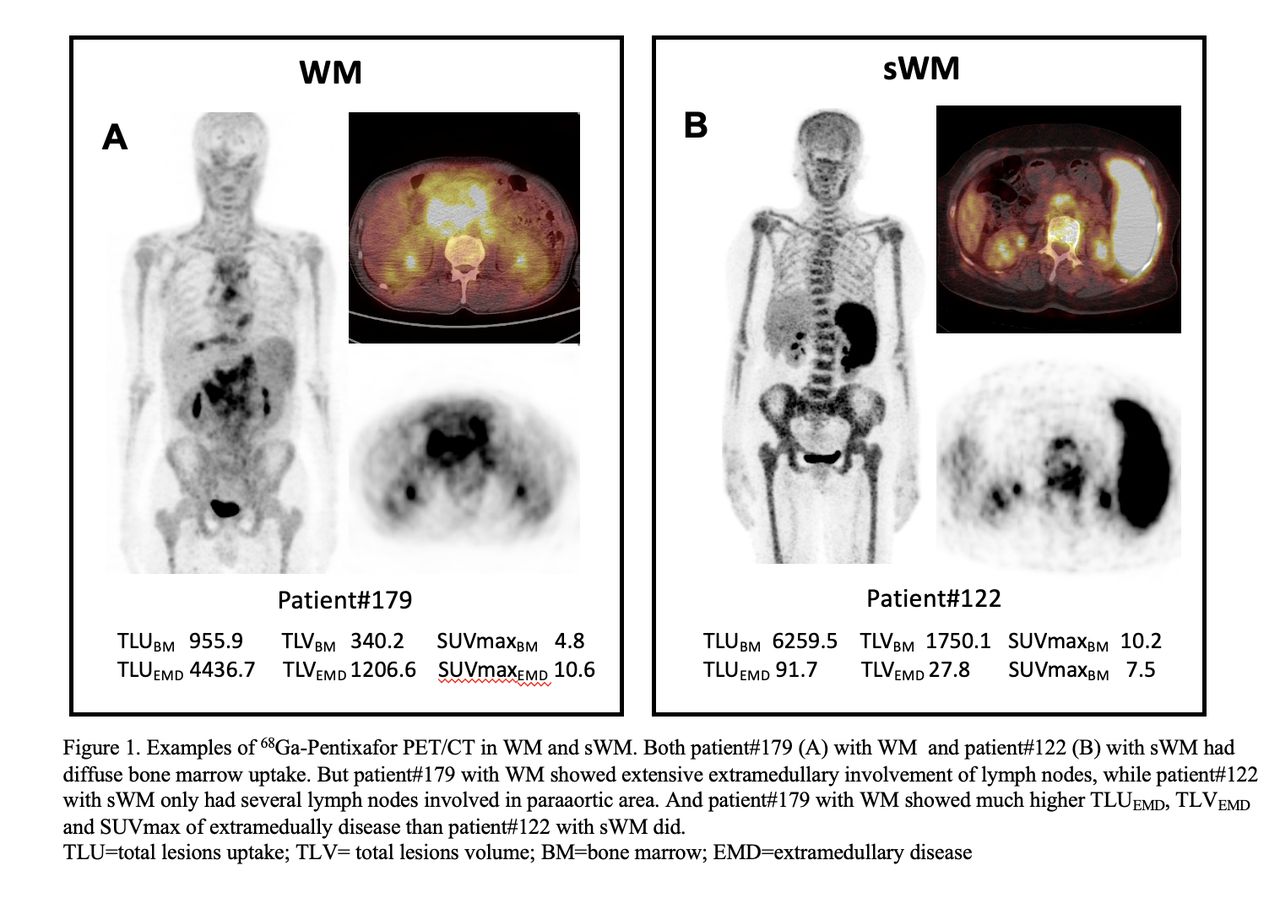
Bone marrow(BM) is the predominant site of involvement in WM and sWM, which was confirmed by BM aspiration and biopsy in all patients. The recruited patients showed diffuse BM uptake in 68Ga-pentixafor PET/CT (SUVmax, 7.4±3.8;range, 2.0-21.3). 7/37(18.9%) WM patients showed heterogeneous distribution of BM disease in 68Ga-pentixafor PET/CT, while other WM and sWM patients had evenly distributed BM uptake of 68Ga-pentixafor. The difference of SUVmax of BM, TLVBM and TLUBM between WM and sWM patients were not significant(Table 2).
Lymph node(LN) involvement was the most common extramedullary disease(EMD), detected in 29/48(60.4%) patients. 22 patients had involvement in more than 3 LN regions. The shortest diameter of the largest LN in each patient was 20.2±10.4mm(range, 5.0-42.0mm), with an SUVmax of 8.8±3.7(range, 3.7-18.8) in the hottest LN. When comparing WM and sWM patients, there was no significant difference of the incidence of LN involvement(64.9%[24/37] vs. 45.5%[5/11], P=0.304), however, patients with WM had more LN regions involved (median number of involved LN regions, 8 vs.1, P=0.000), significantly higher incidence of involvement in more than 3 LN regions(59.5%[22/37] vs. 0%, P=0.000), and larger LN than sWM patients(the median shortest diameter of the largest node[mm], 19.0 vs. 9.0, P=0.004)(Table 2).
Splenomegaly was detected in 13 patients. The incidence of splenomegaly in patients with WM and sWM did not differ significantly(27.0%[10/37] vs. 27.3% [3/11], P=1.00), and the vertical length of the spleen was not significantly different either(median vertical length[mm], 10.6 vs. 9.4, P=0.54).
11 patients with WM had other EMD shown in 68Ga-pentixafor PET/CT, including paramedullary disease, dura mater, liver, spinal nerve roots, pleura, pancreas and kidney. None of the sWM patients had EMD other than LN involvement or splenomegaly. Comparing the quantitative indexes in 68Ga-pentixafor PET/CT, WM patients showed significantly higher TLUEMD, TLVEMD and SUVmax of EMD than sWM patients did(P<0.05, Table 2).
Follow-up
Follow up data was available in 47/48 patients(median follow up time, 26.6 months). For patients with WM, 35/37(94.6%) patients received treatment against WM after baseline PET/CT. The overall response rate was 90.0%(27/30). The median progression free survival was 50.1months(95%CI, 28.2 to 51.5 months).For patients with sWM, 8/11(72.7%) patients remained asymptomatic and did not require treatment until the last visit. The remaining 3 sWM patients developed symptoms after 14.9-39.9 months after PET scan, and treatment against WM was initiated.
Conclusions: Comparing to WM, sWM presented with less LN regions involved, smaller LN and no extranodal involvement on 68Ga-pentixafor PET/CT which could be used to differentiate these two groups.



In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.