


Abstract
P369
Introduction: Predictive biomarkers derived from FDG PET/CT have the potential to enhance individualized treatment selection and optimize outcomes in patients with relapsed/refractory diffuse large B cell lymphoma (DLBCL). Metabolic tumor volume (MTV) has already been shown to be a strong independent prognostic factor in DLBCL. Here, we investigated the effect of lesion dissemination (Dmax) on treatment response and time-to-event outcomes in patients with relapsed/refractory DLBCL treated with Loncastuximab Tesirine in a clinical trial cohort.
Methods: In this post-hoc analysis, we reviewed screening baseline PET/CT images of patients enrolled in the LOTIS-2 trial (NCT03589469). Dmax was calculated as the maximum distance between FDG avid lesions that were farthest apart. The maximum SUV of the lesion with the highest metabolic activity was classified as SUVmax. Both parameters were calculated by a single experienced nuclear medicine radiologist using the Hermes Affinity Viewer. We tested if these quantitative PET metrics as continuous or binary variables could predict treatment response, progression-free survival (PFS) and overall survival (OS). Wilcoxon rank-sum test was used to evaluate associations between PET metrics and treatment response. For PFS and OS, we determined cutpoints of PET metrics for risk-stratification using the outcome-oriented method by Contal and O’Quigley. Internal validation based on bootstrapping was performed to evaluate predictive performance of the identified cutpoints by using Cox univariable models. Integrated area under the ROC curve at all event times (AUC) was used as the prediction metric. Optimism was calculated as the average difference between AUC on bootstrapped samples and AUC on original data. Optimism-corrected AUC (ocAUC) was calculated as the final prediction metric to account for model overfitting.
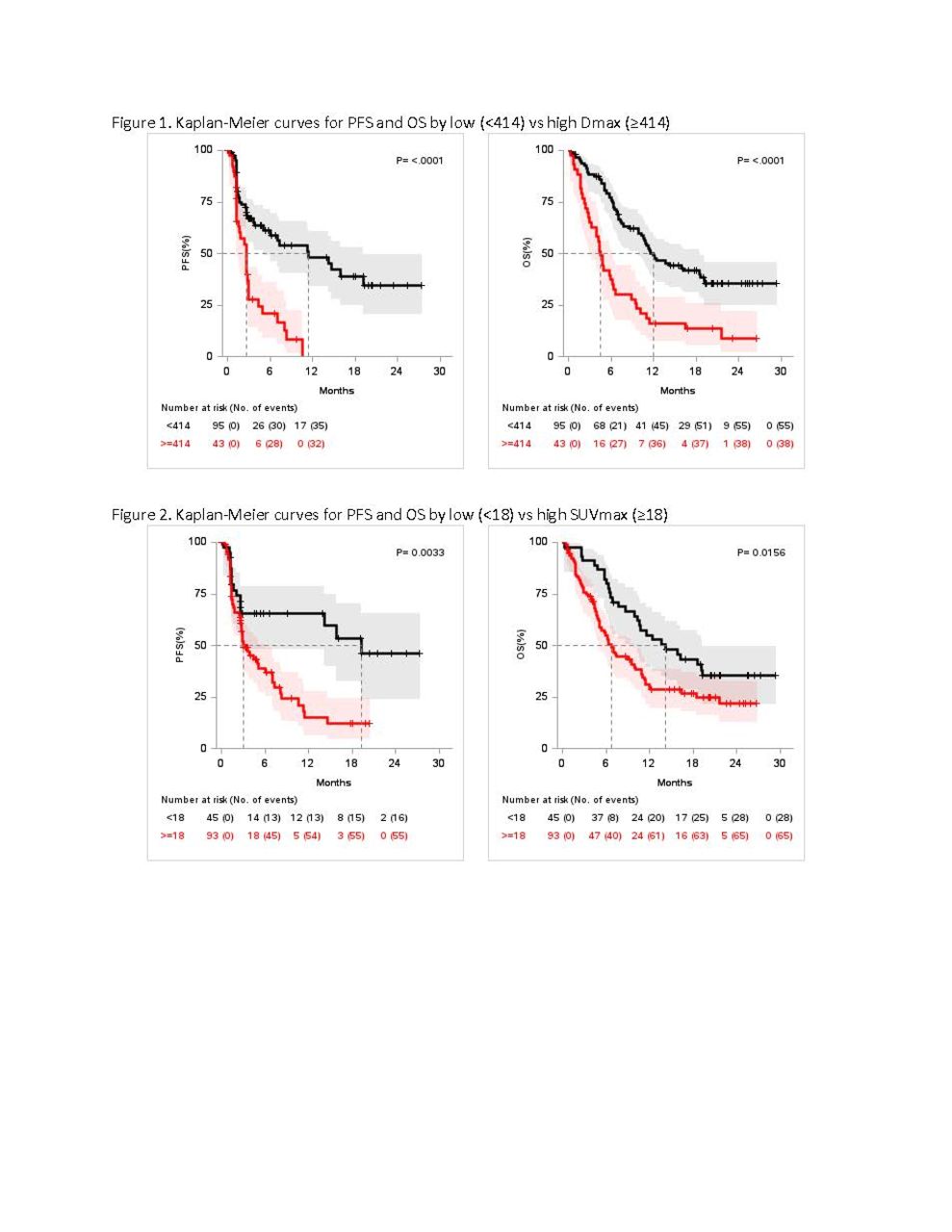
Results: 138 (95%) of the 145 patients enrolled in the LOTIS-2 trial were available for review. The median age in this patient cohort was 65 years, and the median Dmax and SUVmax were 268.15 and 24.4, respectively. First, we analyzed associations of these metrics with treatment response. Significantly lower Dmax values were observed in patients with complete or partial metabolic response (CMR/PMR; median=209.7) than in those with no metabolic response (NMR), disease progression (PD), or not evaluable (NE) (NMR/PD/NE; median=322.7) (P=0.035). On the other hand, lower SUVmax values were observed in patients with CMR (median=17.5) compared to those failing to achieve CMR (PMR/NMR/PD/NE; median=26) (P= 0.003). We then evaluated prognostic value of these metrics in association with PFS and OS (Figure 1 and 2). The optimal cutpoints of Dmax and SUVmax for PFS were 414 mm and 18, respectively, and the same cutpoints were used for OS. In univariable analysis, shorter PFS and OS were observed in patients with Dmax ≥414 mm (PFS: HR=3.02, 95%CI: 1.85-4.94, P<.001, ocAUC=0.646 & OS: HR=2.62, 95%CI: 1.73-3.99, P<.001, ocAUC=0.660), and in those with SUVmax ≥18 (PFS: HR=2.30, 95%CI: 1.30-4.07, P=0.004, ocAUC=0.598 & OS: HR=1.72, 95%CI: 1.10-2.69, P=0.017, ocAUC=0.615).
Conclusions: The present analysis demonstrates that lesion dissemination can be a valuable imaging biomarker derived from FDG PET/CT in patients with relapsed/refractory DLBCL treated with Loncastuximab Tesirine. Future studies are needed to establish predictive models incorporating Dmax and other imaging biomarkers for individualized treatment planning.

In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.