


Abstract
P346
Introduction: Radiohybrid (rh) ligands to the prostate-specific membrane antigen (PSMA) are a novel group of theranostic agents with favorable properties compared with the conventional vectors used in radioligand therapy (RLT). We compared one of these radiopharmaceuticals, 177Lu-rhPSMA-10.1 (rh10), with 177Lu-PSMA I&T (I&T) in patients with advanced, metastatic castration-resistant prostate cancer (mCRPC) scheduled for RLT. As the use of RLT moves earlier in the prostate cancer timeline, minimizing the dose to the kidney becomes more clinically important due to the longer life expectancy of patients. Additionally, delivering higher tumor absorbed radiation doses may permit improved clinical outcomes.
Methods: Four patients (P1-P4) with advanced, histologically proven mCRPC were evaluated. All patients were scheduled for RLT based on the decision of the local multidisciplinary tumor team. Pre-therapeutically, all patients were administered with (1.06 ± 0.05) GBq rh10 as well as with (1.09 ± 0.02) GBq I&T within two subsequent weeks. For dosimetric assessment, whole-body planar scintigraphy was acquired after 5 min, 4h, 1d, 2d, and 7d. In addition, tomographic single photon emission/computed tomography (SPECT/CT) images were acquired over the thorax and the abdomen, 4h, 1d, 2d, and 7d post injection. Dosimetry of the whole body and salivary glands was based on the evaluation of the counts in whole-body planar imaging. Uptake data for dosimetry of the kidneys, the liver, the spleen and the bone marrow as well as up to four tumor lesions were based on the activity in volumes drawn in SPECT/CT images. Doses were calculated using OLINDA/EXM v. 1.0. In addition, for each patient the therapeutic index (TI) as ratio between mean dose of the metastases and mean dose of the kidneys was calculated.
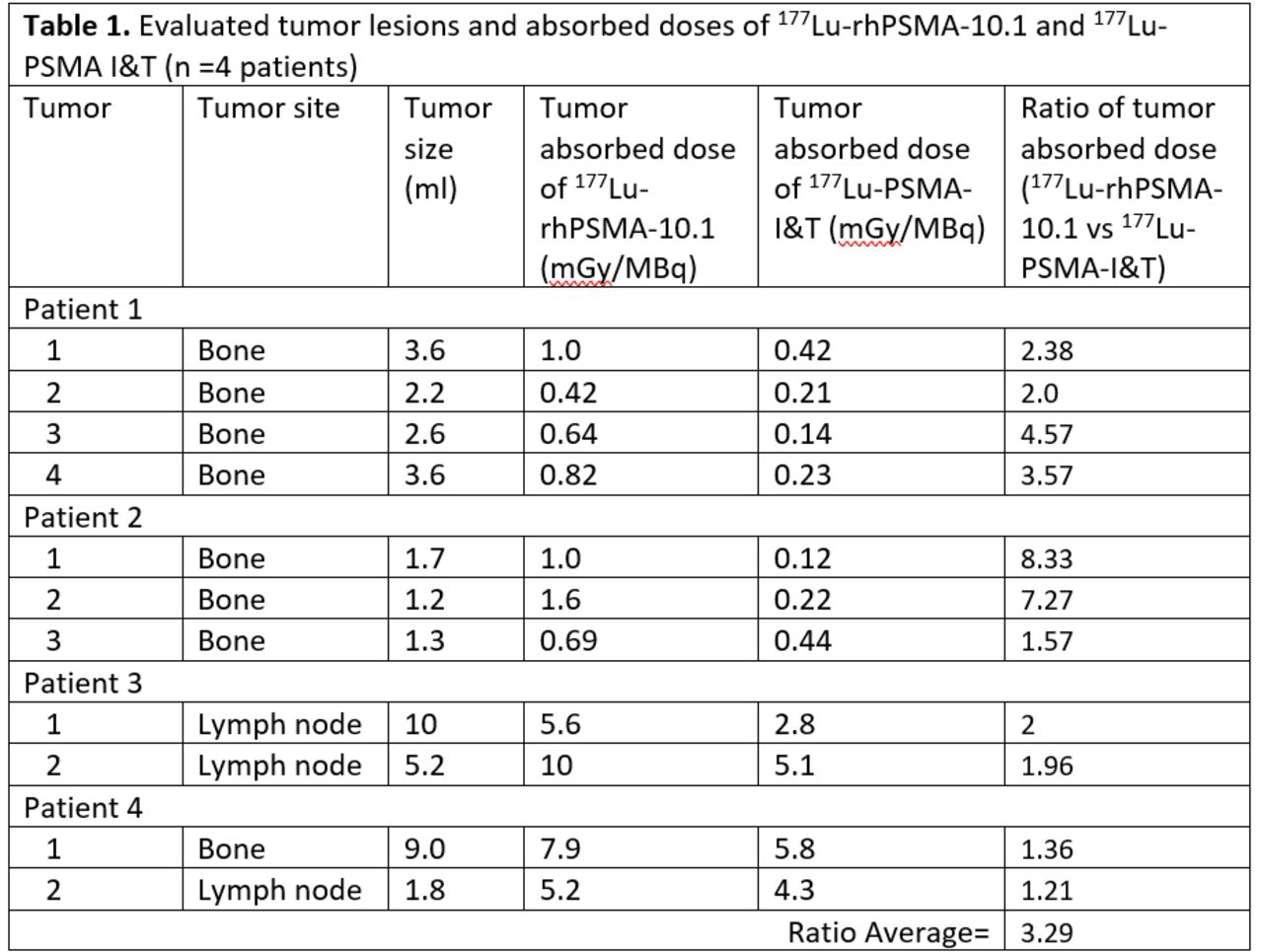
Results: The effective whole-body dose was found to be (0.038 ± 0.008) Sv/GBq for rh10 and thus higher than for I&T (0.022 ± 0.005) Sv/GBq, mainly due to 50% higher dose to the kidneys with (0.69 ± 0.30) Gy/GBq for rh10 vs. (0.46 ± 0.11) Gy/GBq for I&T. Bone marrow doses were (0.07 ± 0.06) Gy/GBq for rh10 vs. (0.04 ± 0.04) Gy/GBq for I&T, while doses to the salivary glands were (0.43 ± 0.18) Gy/GBq for rh10 vs. (0.13 ± 0.04) Gy/GBq for I&T. Tumor doses were significantly higher with rh10 than I&T. Across each evaluated lesion, rh10 delivered an average of 3.3 times (1.2-8.3) higher tumor absorbed radiation dose (Table 1). Consequently, the TI was higher for rh10 compared with I&T (P1 43%, P2 213%, P3 70%, P4 6.4%) in all cases.
Conclusions: Using the radiohybrid PSMA-ligand rh10 can significantly increase the tumor absorbed dose and improve the TI. An improved TI gives the option of maximizing tumor absorbed doses, or, in earlier disease reducing the radiation exposure to normal organs while still achieving an effective tumor dose. Careful assessment of kidney and salivary gland organ function in prospective clinical trials is necessary.

In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.