


Abstract
P153
Introduction: Juvenile xanthogranuloma(JXG) is a benign proliferative disease of histiocytes derived from dermal dendritic cells [1]. It is usually found in early childhood, which mainly occurs in two forms which include papules and nodules. Although the cutaneous JXG is often self-limited, systemic JXG is quite aggressive with serious complications. So it is necessary to define the ranges and extent of systemic JXG lesions by an effective imaging technology. 18F-FDG PET/CT is proved to be a useful imaging method for detection malignant tumors with high glucose metabolism. It also can detect inflammatory cells and reveal metabolically active histiocytosis that were not identified with conventional imaging technology. Here, we report a case of systemic JXG evaluated lesion content and therapy response using 18F-FDG PET/CT.
Methods: A 9-year-old buy was diagnosed with JXG of the right upper limb. After resection, chest CT found more lesions. In order to make sure lesion extent of whole body and guide therapy, He received 18F-FDG PET/CT examination
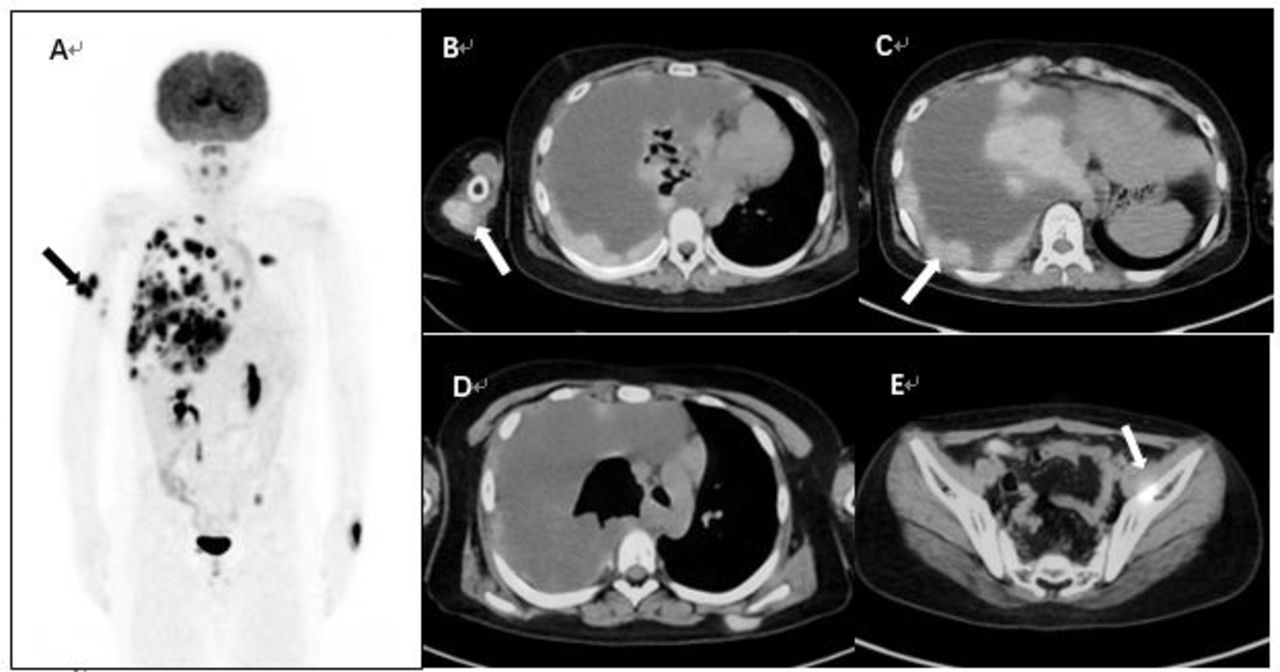
Results: We found multiple high FDG uptake lesions were seen in the right upper limb, and SUVmax was 13.3(Fig 1A, B, arrow). Right pleura was thickening with high FDG concentration, and SUVmax was 27.7 (Figure 1C, arrow). A small subcutaneous nodule(0.9cm) with increased FDG uptake could be seen at the level of the left scapula, SUVmax was 3.9(Figure 1D, arrow)。Finally, we considered all of above lesions were JXG involvement. This boy underwent pleural biopsy after the first PET/ CT scan. Pathological results showed that this lesion is JXG. PET / CT imaging was performed again after 2 cycles of chemotherapy. Compared with first PET/CT scan, Multiple high FDG uptake lesions were still seen in the right upper limb, and FDG uptake was increased, SUVmax:15.8 ((Figure 2A, arrow). Right pleura was thickening and FDG uptake was slight lower, SUVmax:23.3 (Figure 2B, arrow). The subcutaneous nodule at the level of the level of the left scapula was larger with a diameter of 2.5cm. And the FDG uptake was significantly higher, SUVmax: 14.4 (Figure 2 C, arrow). There was a new lesion with high FDG uptake in left iliac muscle, SUVmax was 6.4. Systemic JXG is rare and involves many organs, like liver, spleen, pancreas, gastrointestinal tract, and central nervous system. Compared with conventional imaging, 18F-FDG PET/CT is advantageous for whole-body monitoring and staging of histiocytosis and evaluating response to therapy, because it could detect increased metabolic activity in histiocytosis. Here are some reports show that18F-FDG PET/CT is helpful to fine systemic JXG involvement and monitor therapy response. In these study, Lesion involvement pattern are different. One report found JXG is mainly involved peritoneal surfaces and lymph nodes . Another report show involvement pattern is bone,soft tissue,lung and lymph node. In our case, we find all of the lesions have high FDG uptake and mainly involved pleural and subcutaneous soft tissue, and there was different metabolic response of lesions after chemical therapy. The reduction of FDG uptake was in pleura, but increasing of FDG uptake is in subcutaneous nodule. Besides JXG, FDG uptake also has been demonstrated in other histiocytosis, such as Rosai-Dorfman disease and Erdheim-Chester disease. But it is difficult to differential of JXG from other histiocytosis just depend on imaging modalities, because of the uptake of FDG is nonspecific. Familiarity with uptake patterns and imaging features, in conjunction with clinical manifestations, aids in accurate diagnosis of histiocytosis.
Conclusions: This report showed 18F-FDG PET/CT imaging characters of systemic JXG which mainly involved pleural and subcutaneous, meanwhile observed the different metabolic response change after chemical therapy. It suggests that FDG PET/CT not only can observe the extent of lesions, but also might play a role in monitoring therapy response in patients with systemic JXG.


In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.