


Abstract
P1510
Introduction: Persistent left superior vena cava (PLSVC) is a rare vascular anomaly. Even though PLSVC is not a frequent vascular anomaly, it is the most common form of thoracic venous congenital anomaly, and its frequency is 0.3-0.5% in the general healthy population. PLSVC usually drains into the right atrium through the coronary sinus, and into the left atrium in the remaining cases. Left atrial drainage is a cause of right-to-left shunt and is mostly accompanied by cardiac anomalies. PLSVC identification may be a key point for patients: while it is usually asymptomatic, it can lead to significant problems such as cardiac arrhythmias, syncope, or cyanosis, and may have a major influence on the vascular interventional or surgical treatment procedure of cardiac anomalies.
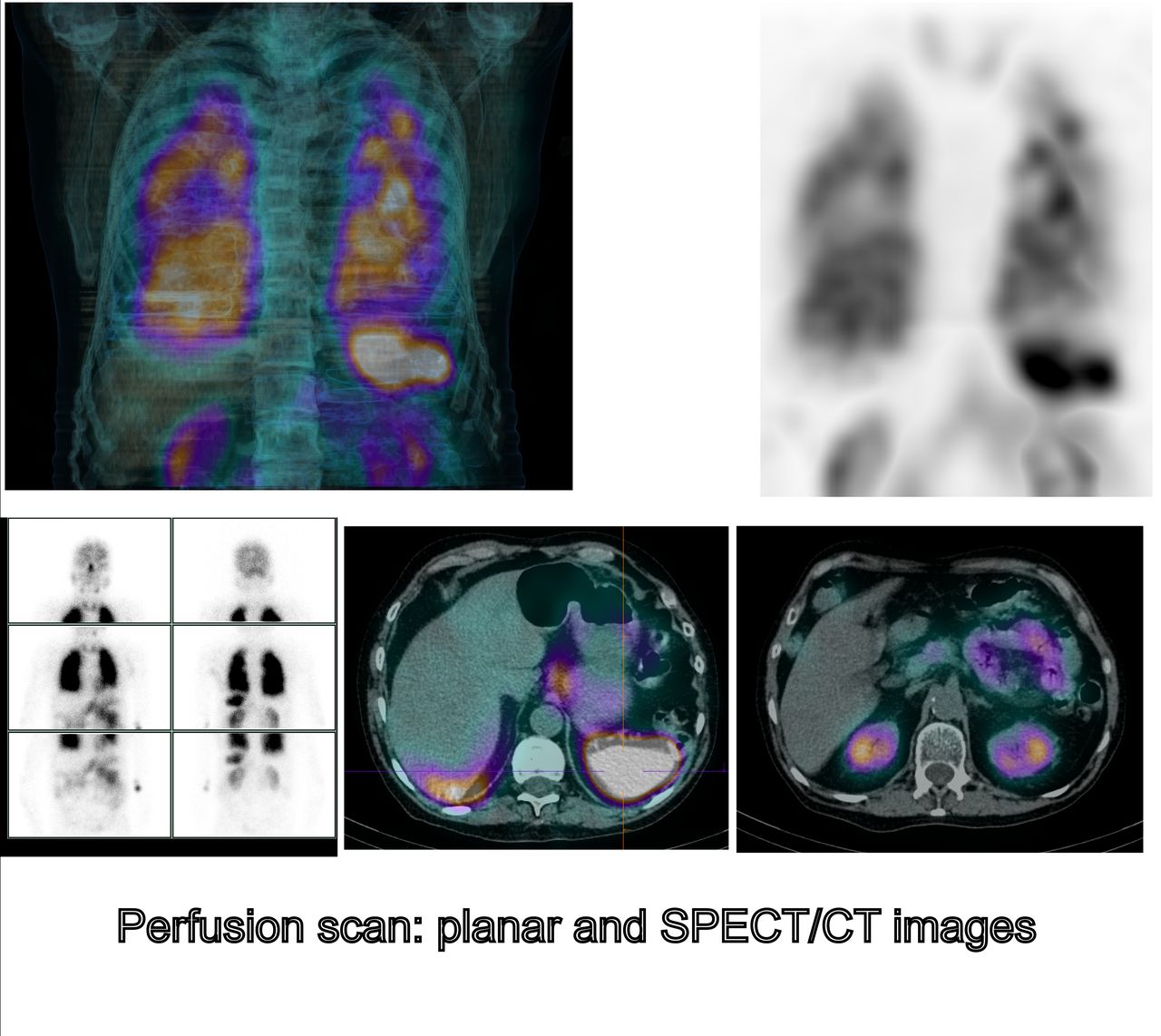
Methods: A 71 year-old patient was addressed to nuclear medicine department to explore a persistant platypnea-orthodeoxia syndrome after occlusion of a patent foramen ovale (PFO) in a context of a COVID-19 infection. The patient underwent a ventilation-perfusion (V/Q) scan with single photon emission computed tomography / computed tomography (SPECT/CT) scan using 99mTc–macroaggregated albumin (MAA) for perfusion and 81mKr for ventilation on a Siemens SYMBIA T2 gamma-camera. 99mTc-MAA were injected at left arm (left antecubital injection). Additional brain, lung, and kidneys perfusion planar images were also performed. Considering the results of the V/Q scan, a contrast-enhanced cardiac helical computed tomography (CHCT) was performed the same day.
Results: The perfusion planar images showed a massive right-to-left shunt (shunt fraction quantification : 30%) with an important pathological increased activity in both brain and kidneys. The perfusion SPECT/CT scan did not found any acute or chronic pulmonary embolism, but visualized extrapulmonary activity, notably in both kidneys, spleen (intense activity), pancreas, stomach, and intestinal tract.Considering that the PFO occlusion was probably effective, a contrast-enhanced CHCT was performed in search of cardiac or vascular anomalies that could explain the massive right-to-left shunt.Contrast-enhanced CHCT showed no sign of pulmonary embolism and a correct position of the PFO closure device, and found a PLSVC with left atrial drainage that could contribute to the patient’s condition. CT scan also showed bilateral areas of ground-glass opacities in a peripheral distribution related to the concurrent COVID-19 infection, that could also contribute to the symptomatology.
Conclusions: PLSVC is a rare vascular anomaly, and its left atrial drainage is atypical. PLSVC identification may be a key point for patients since it may have impact on patient care. Many image findings of PLSVC have been reported, but few mentioned findings in V/Q scan, especially in perfusion SPECT/CT images with a massive right-to-left shunt in case of left atrial drainage site with left antecubital injection of 99mTc–MAA.


In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.