


Abstract
P1406
Introduction: Neuroinflammation has been implicated in the pathophysiology of neuropsychiatric disease. People living with HIV (PLWH) have high rates of comorbid psychiatric disorders, including substance use disorders and depression. Additionally, because standard of care antiretroviral therapy (ART) does not cross the blood-brain barrier, the CNS represents a potential disease reservoir. Multiple studies have used TSPO-focused tracers to measure neuroinflammation in PLWH with varied results. Our group recently published promising results showing elevated neuroinflammation in Parkinson's disease using PET [F-18]-6-(2-fluoro-propyl)-4-methylpyridin-2-amine) ([F-18]NOS) imaging which targets the inducible isoform of nitric oxide synthase (iNOS). The goal of this study was to use [F-18]NOS PET brain imaging to measure neuroinflammation in HIV+ individuals without comorbid neuropsychiatric disease or potentially confounding medications.
Methods: Fourteen individuals, 8 healthy controls (HCs) and 6 HIV+ individuals, ages 18-60, underwent [F-18]NOS PET brain imaging. HIV+ subjects were on stable ART, had a viral load equal to or less than 200 cells/mm3, had a CD4+ count > 200 cells/mm3 with one year of screening per medical record review, and were taking no systemic medications with anti-inflammatory effects per study team review. Before radiotracer administration, a radial arterial line was placed for dynamic blood sampling and radiometabolite determination. 60 minutes of dynamic PET imaging on a Philips Ingenuity PET/CT scanner was initiated prior to intravenous administration of 3.5-6.5 mCi in the upper extremity opposite the arterial line. Before PET imaging, subjects underwent MRI brain imaging, including a T1 1mm isotropic sequence for co-registration with and segmentation of the PET brain data. Blood samples also were collected to measure peripheral markers of inflammation. Using an AAL template, regional TACs were fitted using each individual's arterial metabolite-corrected input function. Three studies (1 HC and 2 HIV+) were eliminated from the data set due to problematic curve fitting of arterial-line metabolites, leaving 7 HCs and 4 HIV+ subjects. Eleven volumes of interest (VOIs) were analyzed: amygdala, cerebellum, frontal lobes, parietal lobes, temporal lobes, occipital lobes, caudate, putamen, thalamus, and hippocampus.
A one-tissue compartment model of reversible radiotracer uptake with fixed blood volume was used to estimate delivery of tracer to tissue (K1), flux from tissue to blood (k2), and total volume of distribution (VT). A two-tailed t-test was used to assess group differences. Non-parametric Kruskal-Wallis tests were used to assess group differences in peripheral markers of inflammation.
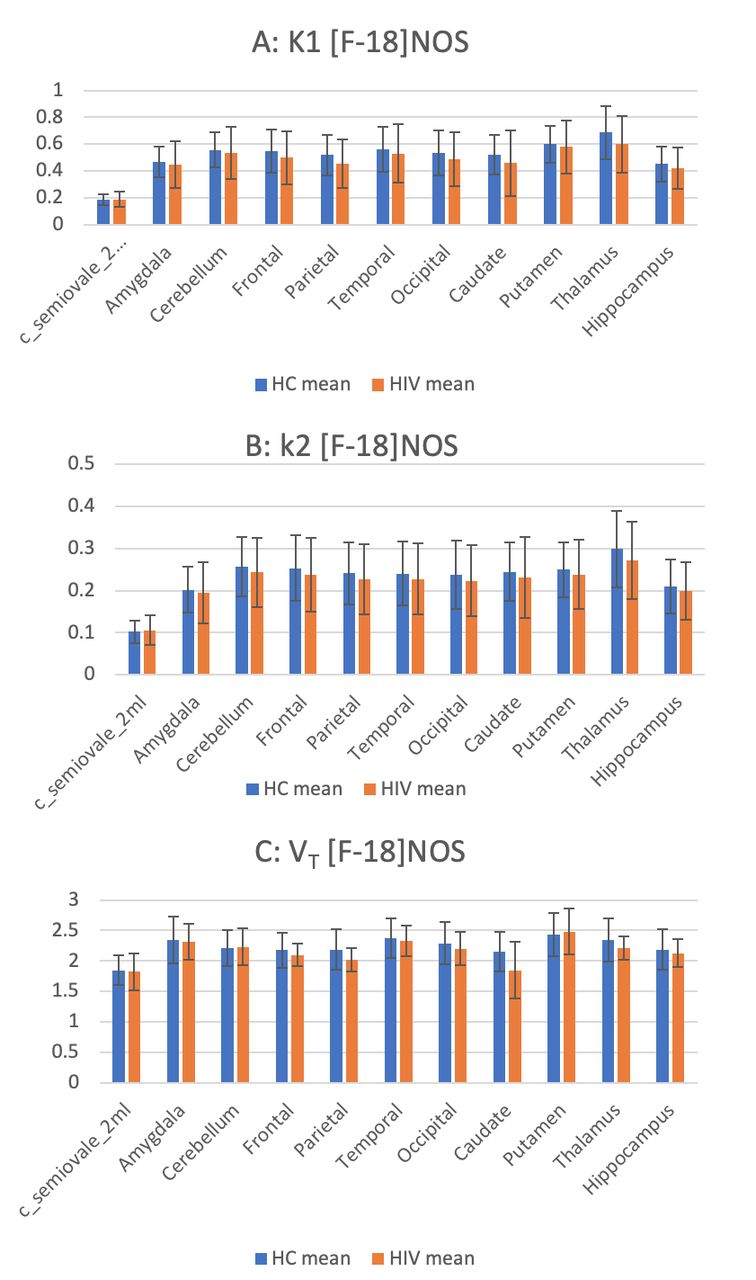
Results: When comparing HIV+ subjects to HCs, [F-18]NOS K1, k2, and VT did not differ in neuroanatomical VOIs. Figure 1 illustrates mean values for each group K1 (A), k2,(B), and VT (C); error bars represent standard deviations. HIV+ subjects showed higher C-reactive protein (CRP) levels than HCs, H(1)=5.77, p=0.016.
Conclusions: In this limited cohort, HIV+ individuals (n=4) did not differ from HCs in their [F-18]NOS brain uptake based on similar levels of iNOS but showed higher CRP levels than HCs. Higher CRP levels in HIV+ individuals are consistent with research showing that CRP increases over time in PLWH and may be a marker of HIV infection. Further studies are needed to ascertain whether PLWH on stable ART demonstrate elevated levels of neuroinflammation.

In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.