


Abstract
P1325
Introduction: Colorectal cancer currently contributes to a significant proportion of cancer-related morbidity and mortality, which is mainly attributed to a notoriously high rate (approx. 25.7%) of local and systemic recurrences. The introduction of chemoradiotherapy (CRT) has dramatically improved the survival outcomes in such cases. Pathological evaluation of the resected specimen with the evaluation of the pathological tumor regression grade (p TRG) is the gold standard for assessing the treatment response of primary tumors after CRT. This takes into account the proportion of residual tumor cells and fibrosis within the resected tumor specimen. Surgical and treatment-related morbidity reduce the feasibility of using histopathology for response assessment in each and every patient; additionally, systemic metastasis is usually not resected or biopsied in the presence of a known primary. In such a situation, imaging plays a central role in the response assessment of such advanced colorectal cancers to adjuvant chemoradiotherapy. Computed tomography (CT) and pelvic magnetic resonance imaging (MRI) provides an excellent anatomical evaluation of locally recurrent cancer, both were initially not able to differentiate between residual tumor and treatment-induced fibrosis. Newer MR imaging techniques like diffusion-weighted imaging (DWI) and dynamic contrast-enhanced (DCE) MRI provide valuable functional information. MRI however has limited availability and suffers from cost restraints. Additionally, systemic evaluation in a single sitting by these modalities is little. 18 F-FDG-PET with CT overcomes these limitations and allows a comprehensive review of the residual tumor metabolic activity with simultaneous anatomical assessment post-CRT. FDG PET CT has previously demonstrated a decent role in evaluating the tumor response to CRT in many cancers. The objective of this study was to evaluate the efficacy of 18F-FDG-PET/CT in the evaluation of tumor response to chemoradiation therapy for advanced colorectal cancer, which included metastatic rectal cancer at primary presentation and recurrent cancers with local and/or distant metastasis.
Methods: Fifty patients with advanced rectal cancer underwent two-point imaging with 18 FDG PET/CT before and after 3 weeks of completion of preoperative/palliative CRT (chemotherapy: 5-fluorouracil, oxaliplatin, and folinic acid; radiation: 45 Gy /25 daily fractions) in between 2016 to 2022. Patients with locally recurrent cancer also underwent radical surgery. The assessment consisted of an evaluation of the following metabolic PET parameters: Standardized Uptake Value maximum (SUVmax), Standardised Uptake Value ratio (SUVratio), Metabolic Tumor Volume (MTV), and Total Lesion Glycolysis (TLG). The response was assessed among the following patients using RECIST 1.1 criteria.
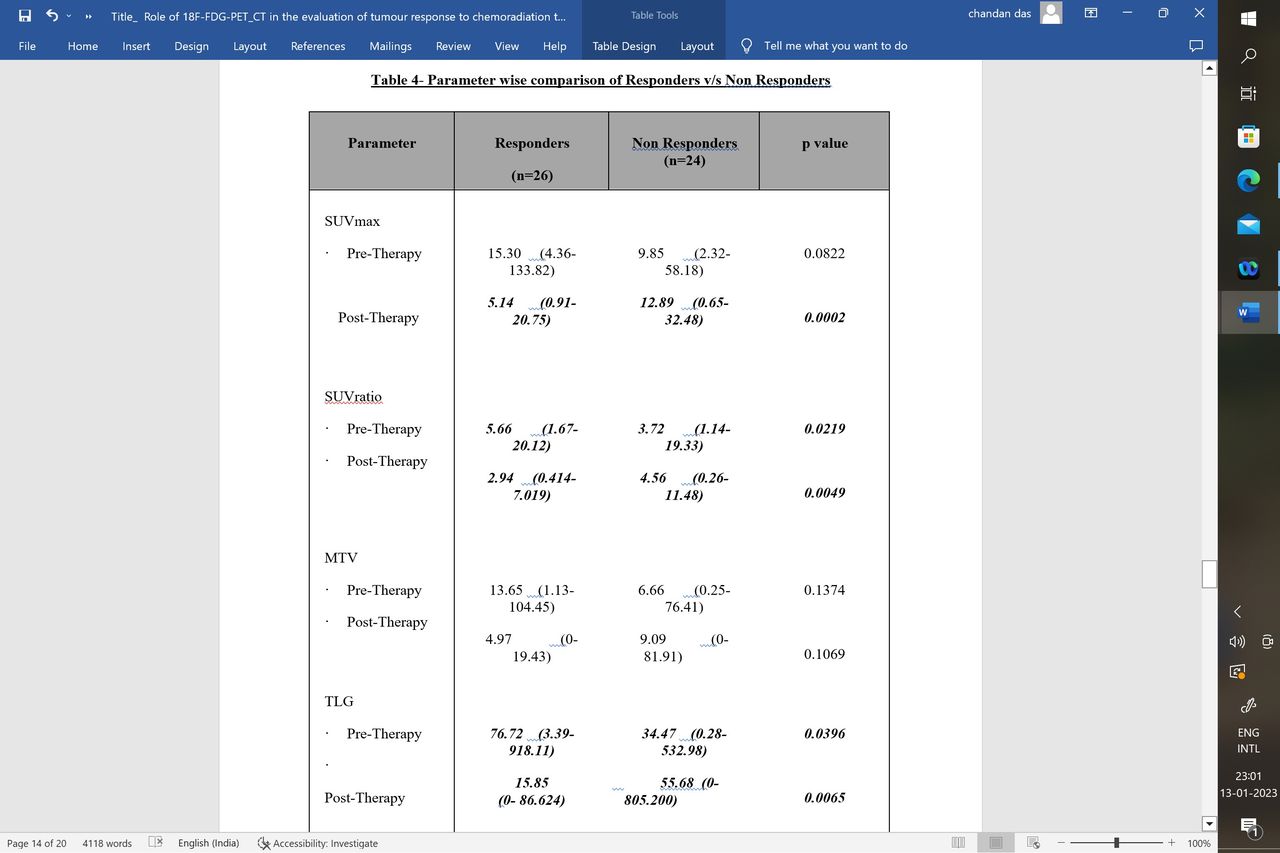
Results: There was a significant decline in the mean post-therapy SUV max and SUVratio compared to baseline (pre-SUV max-2.32-133.82 v/s post SUV max-0.65-32.48, p-value- 0.0001). 26 out of 50 patients (52 %) were classified as responders. A significant decrease in all parameters (SUVmax, SUVratio, TLG, and MTV) from baseline was observed in responders of the study when compared with non-responders (p< 0.05). Besides SUVmax and SUVratio, the mean post-therapy TLG was significantly reduced in responders than non-responders (p-value- 0.0065).
Conclusions: PET-CT is a useful combined anatomic and functional imaging modality in monitoring tumor response to preoperative/palliative CRT in patients with advanced rectal cancer, whether primary or recurrent. Post-therapy SUV and TLG in particular are significantly associated with treatment response.


In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.