


Abstract
P1191
Introduction: Incidental gallbladder uptake is not an infrequent finding on oncologic FDG PET/CT. It can be challenging for the interpreting physician to determine a diagnosis and decide whether to recommend further imaging. While there are case reports describing false positive findings in the gallbladder on FDG PET, such as adenomyomatosis, no study has systematically evaluated incidental gallladder uptake and its causes. The aim of our study is to evaluate the causes of gallbadder uptake and develop a decision tree algorithm to use in routine clinical practice.
Methods: A retrospective study was conducted of all FDG PET/CT scans performed over 5 years (2014-2019) with gallbladder PET findings in the report impression. Patients with primary gallbladder cancer and CT only findings (i.e. cholelithiasis) were excluded. PET/CT images were retrospectively reviewed and the gallbladder FDG uptake morphology, location within wall or lumen, anatomic location, and SUVmax were assessed. The suspected diagnosis of gallbladder uptake was determined through review of prior and follow-up imaging and classified as either benign (i.e. adenomyomatosis) or malignant conditions. Logistic regression was performed for correct classification of gallbladder uptake into benign vs. malignant conditions. Classification and regression tree (CART) modeling was performed with minimum bucket=1, maximum depth =3, and cross-validation.
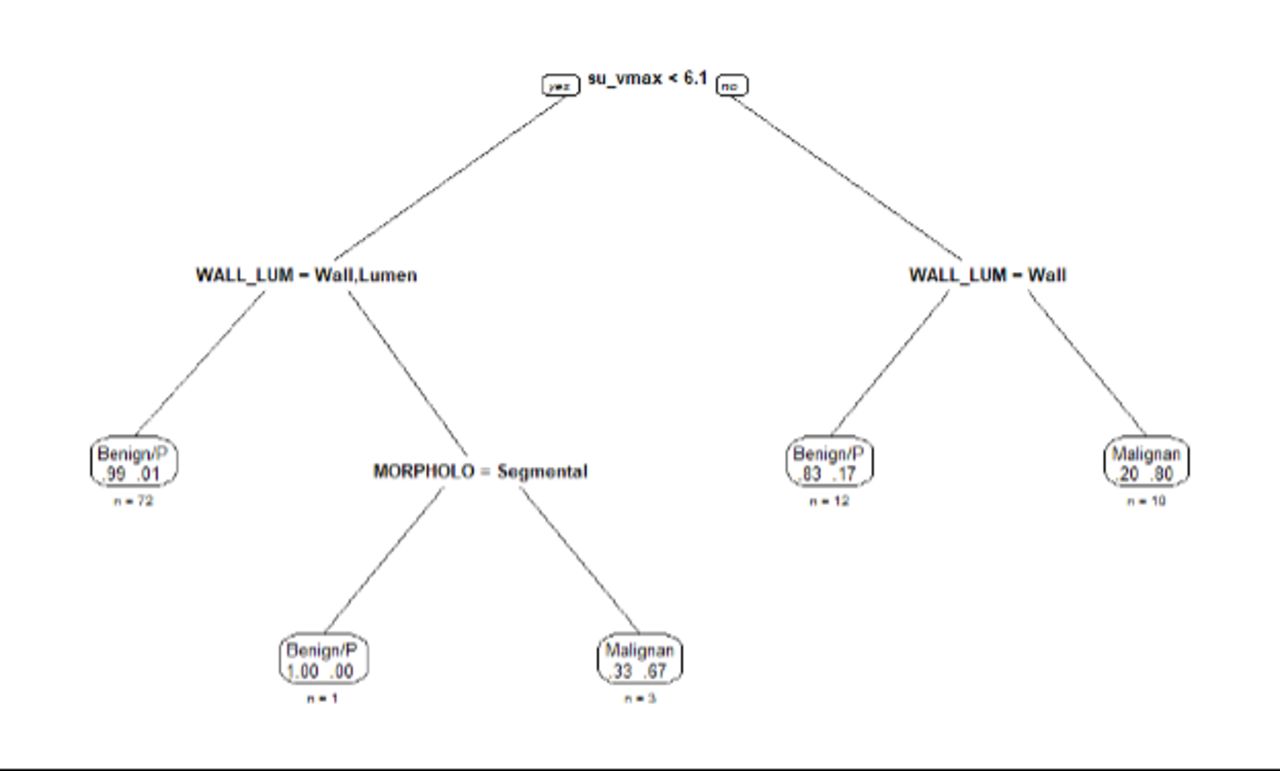
Results: A total of 98 patients were included in the analysis. PET uptake was due to a benign gallbladder condition in 87% of patients (n=62/98) and malignancy in 13% (n=13/98). PET uptake morphology, location within wall or lumen, and SUVmax were statistically significant on univariable analysis (all p<0.05). Only SUVmax remained significant on multivariable analysis, with higher SUVmax associated with risk of malignancy OR =1.33 [1.10 - 1.66 95% CI], p=0.003. ROC curve analysis demonstrated an optimal cutoff SUVmax of 4.7, with AUC=0.88, sensitivity 100%, and specificity 67% (Fig. 1). A decision tree algorithm was created using CART modeling, with root node error = 0.133 and 88.8% prediction accuracy in cross-validation (Fig. 2). In this tree, the first step is to stratify uptake based on SUVmax (<6.1 or >6.1), then location within wall, lumen, or both, and then uptake morphology. On the left side of the tree, all patients have SUXmax <6.1 and if PET uptake is in the wall or lumen, then it is due to a benign condition. If PET uptake is found in the both wall and lumen, then the diagnosis depends on segmental morphology. On the right side of the tree, all patients have SUVmax >6.1 and if PET uptake is in the wall, then it is benign, whereas if it is in the lumen or both, then it is malignant.
Conclusions: The majority of incidental gallbladder uptake on FDG PET/CT scans are due to benign gallbladder conditions. Higher SUVmax is associated with higher odds of malignancy versus benign conditions. Our PET gallbladder uptake decision algorithm can be easily implemented to facilitate reader interpretation, improve diagnostic accuracy, and decide appropriate management.


In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.