


Visual Abstract

Abstract
The aim of this retrospective analysis was to evaluate health-related quality of life (HRQoL) for patients with metastatic castration-resistant prostate cancer (mCRPC) receiving consecutive cycles of 177Lu-prostate-specific membrane antigen (PSMA) radioligand therapy (RLT) using the reliable and validated European Organisation for Research and Treatment of Cancer core quality-of-life (QoL) questionnaire. In addition, differences in HRQoL between patients with early discontinuation of treatment because of disease progression and patients who were defined as eligible for treatment continuation were analyzed. Methods: In total, 60 mCRPC patients were included in this analysis. The European Organisation for Research and Treatment of Cancer core QoL questionnaire was completed at baseline, before each treatment cycle up to the sixth treatment cycle, and at the time of PSMA-ligand PET/CT scans after the second and fourth treatment cycles. QoL assessment included global health status, functional scales, and symptom burden during treatment. Results: Global health was significantly improved at the second and fourth cycles of 177Lu-PSMA RLT (P = 0.014 and P = 0.039, respectively). In line with this, role and emotional functioning showed significant improvements at the second and fourth treatment cycles (role functioning, P = 0.045 and P = 0.048, respectively, and emotional functioning, P = 0.035 and P = 0.007, respectively). In addition, compared with baseline, fatigue and pain were significantly alleviated at the second and fourth treatment cycles (pain, P = 0.035 and P = 0.034, respectively, and fatigue, P = 0.042 and P = 0.041, respectively). Other aspects of HRQoL, even if not significantly improved, remained stable over time, except for deterioration of fatigue at the study’s end (P = 0.014) and reduction of dyspnea at the second treatment cycle (P = 0.012). Patients with early discontinuation of treatment showed a concordant decline in HRQoL. Conclusion: mCRPC patients showed significant improvement in HRQoL in the course of treatment with 177Lu-PSMA RLT. Furthermore, patients with early discontinuation of treatment showed an analogous decline in HRQoL.
- prostate-specific membrane antigen radioligand therapy (PSMA RLT)
- metastatic castration-resistant prostate cancer (mCRPC)
- health-related quality of life (HRQoL)
- EORTC QLQ-C30
In patients with metastatic castration-resistant prostate cancer (mCRPC), radioligand therapy (RLT) that targets 177Lu-prostate-specific membrane antigen (PSMA) has emerged as a promising treatment option and has recently received approval from the U.S. Food and Drug Administration and European Medicines Agency. Patients with metastatic prostate cancer commonly present with bone metastases that potentially lead to severe pain and impaired mobility, which might cause substantial deterioration in quality of life (QoL) (1,2).
Therefore, the assessment of health-related QoL (HRQoL) and its changes during therapy is of major interest when new treatment strategies are evaluated. The recently published prospective phase II and III trials investigated the influence of 177Lu-PSMA-617 RLT on HRQoL for mCRPC patients, reporting improvements in both QoL and symptom control (3–5). A potential tool for the evaluation of QoL in cancer patients is the European Organisation for Research and Treatment of Cancer (EORTC) core QoL questionnaire (QLQ-C30) (4–6). Since its introduction, the EORTC QLQ-C30 has been evaluated in several field studies and appeared as reliable and valid (7). The EORTC QLQ-C30 defines HRQoL as a multidimensional construct consisting of subjectively perceived global health status, different functional scales, and disease-related symptoms. However, despite recent publications investigating the impact of 177Lu-PSMA-617 RLT on HRQoL using small sample sizes over a short treatment period, data on the impact of repeated (≥2) cycles of 177Lu-PSMA I&T RLT on HRQoL using a larger cohort of mCRPC patients are scarce and limited (8). Furthermore, on the basis of our clinical experience, we assumed that patients with treatment discontinuation because of disease progression after the first 2 cycles showed a concordant decline in HRQoL during treatment. Thus, the aims of this analysis were to assess changes in HRQoL with mCRPC during treatment with 177Lu-PSMA RLT and to evaluate potential differences in HRQoL between patients who discontinued treatment because of disease progression and patients who responded and could continue treatment.
MATERIALS AND METHODS
Patient Selection and 177Lu-PSMA I&T RLT
Initially, 92 mCRPC patients with accessible EORTC QLQ-C30 responses who received 177Lu-PSMA I&T RLT in a compassionate-use program between 2014 and 2019 were screened for this retrospective analysis. Of these, 60 patients fulfilled our study-related inclusion criteria and therefore were identified as eligible for our study. The following criteria were used for inclusion: at least 2 cycles of 177Lu-PSMA I&T; completion of 177Lu-PSMA I&T RLT; Eastern Cooperative Oncology Group (ECOG) 0–2; and completed EORTC QLQ-C30 before treatment initiation and at least 12 ± 4 wk after treatment initiation (at PSMA-ligand PET/CT imaging or before the third treatment cycle). The measured time points (e.g., 12 ± 4 wk) were defined retrospectively by the intervals (4- to 8-wk intervals) in which the patients received their treatment cycles or their interim PSMA-ligand PET/CT imaging.
All patients had previously received second-line hormonal therapy with abiraterone or enzalutamide and chemotherapy or were unfit for chemotherapy. Before treatment, sufficient PSMA expression was confirmed by PSMA-ligand PET imaging. Only patients with PSMA-ligand uptake in tumor lesions at least as high as liver background were treated. Data on treatment response and outcome after 177Lu-PSMA RLT of these patients have been previously reported (9,10).
177Lu-PSMA I&T was prepared according to good manufacturing practice and the German Medicinal Products Act (AMG §13 2b). All patients signed informed consent forms and were treated under the conditions of Declaration of Helsinki article 37, “Unproven Interventions in Clinical Practice.” The retrospective analysis was approved by the local ethics committee under reference 115/18 S.
In total, 264 cycles of 177Lu-PSMA RLT with a median of 4 cycles per patient (range, 2–20 cycles) were applied. Patients received intravenous treatment with a standard dose of approximately 7.4 GBq of 177Lu-PSMA I&T every 4–10 wk (median, 6 wk). All patients received at least 2 treatment cycles (n = 60), 2 patients received 3 cycles, and 35 patients underwent at least 4 cycles of 177Lu-PSMA RLT (Table 1). Median time on treatment was 4 mo (range, 2–20 mo).
Baseline Patient Characteristics
QoL Analysis
HRQoL for mCRPC patients was evaluated using the German version of the EORTC QLQ-C30 (version 3.0) (6). The questionnaire was filled out before each 177Lu-PSMA I&T cycle and at the time of PSMA-ligand PET/CT scans after 2 and potentially 4 treatment cycles. Specifically developed for cancer patients, the EORTC QLQ-C30 is a reliable and valid 30-item questionnaire of self-assessed HRQoL. It consists of 1 multiitem measured global health status; 5 multiitem measured functional scales, namely, physical functioning, role functioning (i.e., performance in daily activities and free-time activities or work), cognitive functioning, emotional functioning, and social functioning; 3 multiitem measured symptom scales (fatigue, pain, and nausea or vomiting); and 6 single items (constipation, diarrhea, insomnia, dyspnea, appetite loss, and financial difficulties). According to the standardized EORTC scoring procedure, scores for each multi- and single-item measure were linearly transformed to a score value from 0 to 100 (11). Although high score values in global health and functional scales represent high levels of health status and functional ability, high scores in symptom scales and single items represent worse symptom status.
Statistical Analysis
All analyses were performed using GraphPad Prism version 9.4.1(458) (GraphPad Software) for Mac (Apple). A mixed-effects model that allows missing values was performed to analyze repeated measures data of HRQoL for the total patient cohort and for patients stratified according to their ECOG performance status at baseline (ECOG 0, ECOG 1, or ECOG 2). Questionnaires with a response rate of less than 25% (15%, n = 9) after the sixth treatment cycle were excluded from further analysis. Results were presented as mean changes from baseline scores of HRQoL. A paired t test visualized in Tukey box-and-whisker plots was performed to evaluate differences in HRQoL between patients who were excluded after 2 or 4 treatment cycles (nonresponder) and those who continued treatment beyond 2 or 4 treatment cycles (responder). HRQoL deterioration‐free survival was defined as the time between treatment initiation and first HRQoL score deterioration of at least 5 points compared with the baseline score (without subsequent improvement ≥5 points compared with baseline or improvement to ≥90 if the baseline score was ≥90) or death, whichever occurred first (12). Deterioration‐free survival curves were estimated using the Kaplan–Meier method for estimation of event time distributions, and log-rank tests were used for group comparisons. Patients who were alive were censored at the last HRQoL follow-up (26 ± 4 wk) if deterioration of at least 5 points from baseline was not observed or if a decrease of at least 5 points was present but was followed by improvement of at least 5 points or improvement to at least 90 if the baseline score was at least 90. HRQoL for patients who were excluded from treatment (nonresponder) and in those who were defined as eligible for treatment continuation (responder) was analyzed on the basis of disease progression upon PSMA-ligand PET/CT imaging routinely performed after 2 treatment cycles (at 12 ± 4 wk). The corresponding hazard ratio (HR) and 95% CI are presented. A P value of less than 0.05 was considered statistically significant.
RESULTS
QoL in the Entire Patient Cohort
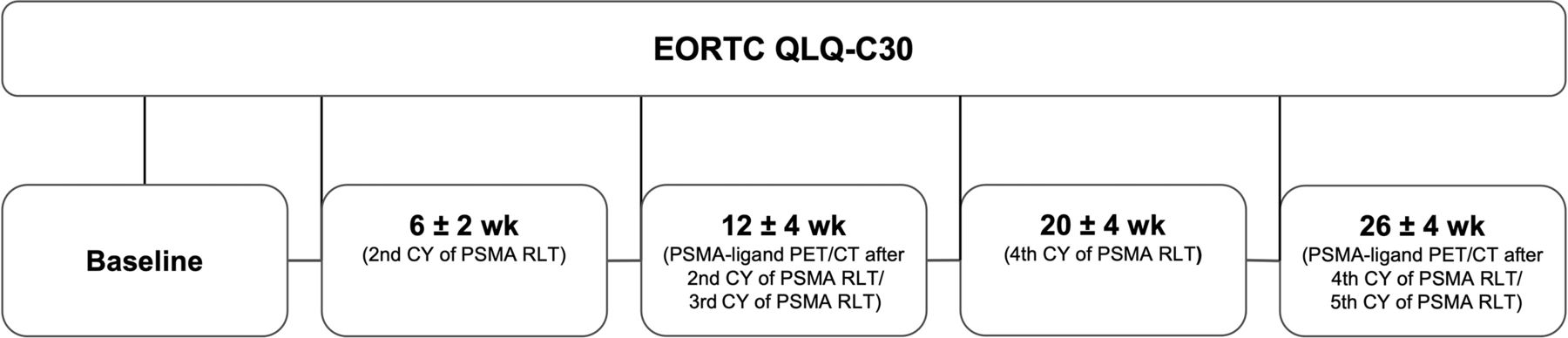
Patient characteristics are shown in Table 1. Before treatment, 32% (n = 19), 57% (n = 34), and 11% (n = 7) of the patients presented with ECOG 0, ECOG 1, and ECOG 2, respectively. At baseline and at 12 ± 4 wk (PSMA-ligand PET/CT imaging after the second treatment cycle or before the third treatment cycle) the questionnaire was available for all 60 (100%) patients (Fig. 1). For 39 (65%), 18 (30%), 16 (27%), and 9 (15%) patients, the questionnaire was available at 6 ± 2 wk (second treatment cycle), 20 ± 4 wk (fourth treatment cycle), 26 ± 4 wk (PSMA-ligand PET/CT imaging after the fourth treatment cycle or before the fifth treatment cycle), and 34 ± 4 wk (sixth treatment cycle) after the first treatment cycle, respectively (Fig. 1).

Study design. CY = cycle.
Compared with baseline, HRQoL improved significantly, revealing elevated global health status at 6 ± 2 wk (P = 0.014) and at 20 ± 4 wk (P = 0.039) after treatment initiation (Fig. 2A; Table 2). In accordance with this, role functioning and emotional functioning demonstrated significant improvements after the first cycle of 177Lu-PSMA RLT and over time (role functioning, 6 ± 2 wk [P = 0.045] and 20 ± 4 wk [P = 0.048]; emotional functioning, 6 ± 2 wk [P = 0.035] and 20 ± 4 wk [P = 0.007]; Figs. 2C and 2D; Table 2). Other aspects of functional ability, namely, physical functioning, cognitive functioning, and social functioning, although not significantly improved, remained constant during treatment (Fig. 2B; Table 2). Moreover, compared with baseline, some symptom scales, such as fatigue and pain, were significantly alleviated at 6 ± 2 and 20 ± 4 wk (fatigue, P = 0.042 and P = 0.041, respectively, and pain, P = 0.035 and P = 0.034, respectively; Figs. 2E and 2F; Table 2). In addition, at 26 ± 4 wk, significant deterioration (P = 0.014) of fatigue was detected (Fig. 2E). Other symptoms, even if not significantly improved (except significant alleviation of dyspnea at 6 ± 2 wk, P = 0.012), showed no deterioration over time (Table 2). Patients with ECOG 0 had higher HRQoL scores and less symptom burden in all domains during the course of treatment, whereas patients within the ECOG 1 and ECOG 2 group had worse HRQoL (Fig. 2; Supplemental Tables 1 and 2 [supplemental materials are available at http://jnm.snmjournals.org]). However, the presented significant effects of 177Lu-PSMA RLT on HRQoL for the total patient cohort were not found within the ECOG-stratified groups (ECOG 0, ECOG 1, or ECOG 2; Fig. 2; Supplemental Tables 1 and 2).

Changes in global health status, selected functional scales (physical functioning, role functioning, and emotional functioning), and selected symptom scales (fatigue and pain) for total patient cohort (blue) and for patients with ECOG 0 (green) and ECOG 1 or ECOG 2 (red) performance status during treatment with 177Lu-PSMA RLT, according to EORTC QLQ-C30. Results are presented as mean changes from baseline and SEM. (A) In total patient cohort, global health status was significantly improved at 6 ± 2 wk (P = 0.014) and 20 ± 4 wk (P = 0.039). (B–D) In total patient cohort, role functioning and emotional functioning were significantly improved at 6 ± 2 wk (P = 0.045 and P = 0.035) and at 20 ± 4 wk (P = 0.048 and P = 0.007), while physical functioning, although not significantly improved, remained constant during treatment. (E and F) In total patient cohort, fatigue and pain were significantly alleviated at 6 ± 2 wk (P = 0.042 and P = 0.035) and at 20 ± 4 wk (P = 0.041 and P = 0.034), whereas fatigue was significantly deteriorated at 26 ± 2 wk (P = 0.014). *P < 0.05. **P < 0.01.
EORTC QLQ-C30 Scores for Total Patient Cohort
QoL for Patients with Early Exclusion from Treatment
Following PSMA-ligand PET/CT imaging after 2 treatment cycles (at 12 ± 4 wk; Fig. 1), 23 patients discontinued treatment because of disease progression and were stratified as nonresponders, whereas 37 patients were defined as eligible for treatment continuation and were stratified as responders (Table 1).
The nonresponder group presented with a lower baseline HRQoL than did the responder group in most assessed domains (Table 3). In addition, significantly worse physical functioning (P = 0.0495) and role functioning (P = 0.011), deterioration of fatigue (P = 0.046), and increased nausea and vomiting (P = 0.008) were detectable at 12 ± 4 wk in the nonresponder group (Figs. 3B, 3C, and 3E; Table 3). In contrast, patients in the responder group showed significantly improved global health status (P = 0.002), alleviation of pain (P = 0.011), and reduced dyspnea (P = 0.047; Figs. 3A and 3F; Table 3). Other aspects of HRQoL, although not significantly improved, remained stable over time (Table 3).
EORTC QLQ-C30 Scores at Baseline and 12 ± 4 Weeks After Treatment Initiation in Nonresponder Patients Receiving 2 Cycles and Responder Patients Receiving More Than 2 Cycles of 177Lu-PSMA RLT

Tukey box plot display of global health status, selected functional scales (physical functioning, role functioning, and emotional functioning), and selected symptom scales (fatigue and pain) for total patient cohort at baseline (black) and at 6 ± 2 wk (light gray) and for patients dichotomized according to number of received treatment cycles of 177Lu-PSMA RLT at 12 ± 4 wk (nonresponder, red; responder, green). (A) Compared with baseline, global health status was significantly improved at 12 ± 4 wk in responder group (P = 0.002). (B–D) Compared with baseline, physical functioning and role functioning were significantly worse in nonresponder group (P = 0.0495 and P = 0.011), while no significant differences were detectable for emotional functioning. (E and F) Compared with baseline, fatigue was significantly deteriorated in nonresponder group (P = 0.046) and pain was significantly alleviated in responder group (P = 0.011). Outliers that differ significantly from rest of dataset were plotted as individual points beyond whiskers on box plot. *P < 0.05. **P < 0.01. ns = not significant.
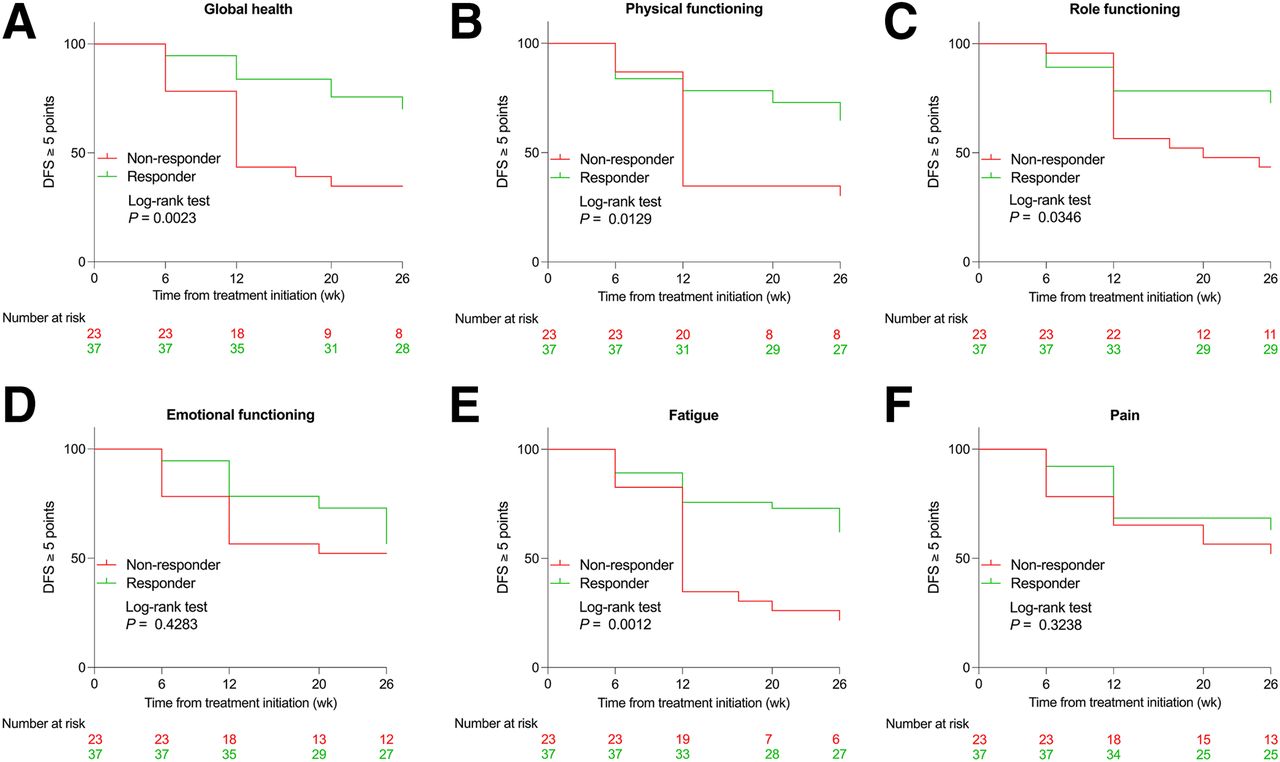
In line with this, the nonresponder group had a significantly higher risk of HRQoL deterioration in global health status (HR, 2.9; 95% CI, 1.3–6.6; P = 0.002), physical functioning (HR, 2.2; 95% CI, 1.1–4.8; P = 0.013), role functioning (HR, 2.2; 95% CI, 1.0–5.2; P = 0.035), cognitive functioning (HR, 2.4; 95% CI, 1.0–6.0; P = 0.035), fatigue (HR, 2.7; 95% CI, 1.3–5.6; P = 0.001), nausea and vomiting (HR, 4.5; 95% CI, 1.6–12.8; P = 0.001), appetite loss (HR, 3.5; 95% CI, 1.3–9.7; P = 0.005), and diarrhea (HR, 3.4; 95% CI, 1.1–10.1; P = 0.017; Figs. 4A–4C and 4E; Supplemental Table 3). Similar trends were observed for most remaining aspects of HRQoL (Figs. 4D and 4F; Supplemental Table 3).

Kaplan–Meier survival curves for HRQoL deterioration-free survival for global health status (A), selected functioning scales (physical functioning, role functioning, and emotional functioning) (B–D), and selected symptom scales (fatigue and pain) (E and F) for patients dichotomized according to number of received treatment cycles of 177Lu-PSMA RLT at 12 ± 4 wk (nonresponder, red; responder, green). DFS = deterioration-free survival.
Differences in HRQoL between patients who discontinued treatment (nonresponder, n = 7) because of relevant disease progression in PSMA-ligand PET/CT imaging after 4 treatment cycles (at 26 ± 4 wk; Fig. 1) and those who continued treatment (responder, n = 9) are given in Supplemental Table 4.
DISCUSSION
The results of our retrospective analysis indicate significant improvements in various aspects of HRQoL (e.g., global health status) during treatment with 177Lu-PSMA I&T RLT in mCRPC. In contrast, patients who discontinued treatment after 2 treatment cycles because of disease progression had a concordant decline in HRQoL and a higher risk of deterioration in QoL than did patients who responded after the initial 2 cycles.
The most affected dimensions of HRQoL were global health status, role functioning, emotional functioning, fatigue, and pain. In these domains, significant improvements were detectable at the second (at 6 ± 2 wk) and fourth (at 20 ± 4 wk) treatment cycles. Our analysis might underline the beneficial impact of 177Lu-PSMA I&T RLT on HRQoL—in contrast to a recently published analysis of mCRPC patients treated with new hormonal agents or first-line chemotherapy, which reported continuous and significant deterioration in, for example, physical functioning, fatigue, and pain (13). However, because our analysis evaluates the impact of 177Lu-PSMA I&T RLT on HRQoL over only a short treatment period, further studies analyzing the long-term impact on HRQoL are warranted.
At PSMA-ligand PET/CT imaging after the second treatment cycle or before the third treatment cycle (12 ± 4 wk) and at PSMA-ligand PET/CT imaging after the fourth treatment cycle or before the fifth treatment cycle (26 ± 4 wk) a slight shift toward HRQoL deterioration was detectable. Similar trends were reported in a previously published prospective phase II trial (4,14). A potential hypothesis for this could be a concordant decline of QoL for patients with relevant disease progression, leading to negative affection of HRQoL at the measured time points. This is supported by our results, which revealed significant deterioration of HRQoL (e.g., physical functioning) for patients who discontinued 177Lu-PSMA RLT after the second treatment cycle because of disease progression (at 12 ± 4 wk), whereas patients who continued treatment showed stabilization or improvement of HRQoL (e.g., global health status). In accordance with this, we could also demonstrate a significantly higher risk of HRQoL deterioration for patients with early treatment discontinuation. This is in line with results from van der Doelen et al., who reported stabilization of HRQoL for patients who completed 223Ra treatment but observed decline in HRQoL for patients who discontinued treatment (15). The same was true for most assessed HRQoL domains for patients who discontinued treatment after 4 treatment cycles compared with those who received more than 4 treatment cycles. However, in this patient cohort, none of the detected differences were statistically significant, which is most likely because of the small sample size.
Two previously published prospective phase II trials analyzed HRQoL using the EORTC QLQ-C30 for mCRPC patients undergoing 177Lu-PSMA-617 RLT (4,5,14). These trials reported higher HRQoL scores and lower symptom burden at baseline in most domains than found in our results (5). The worse HRQoL scores at baseline reported in our analysis might be explained by the more advanced disease stage in our patient cohort, including visceral metastases in 32% of our patients (n = 19) versus, for example, 7% of TheraP patients (n = 7), given the known negative association of visceral metastases with outcome (5,16). In addition, 20% (n = 12) of our patients received pretreatment with cabazitaxel versus none of the TheraP patients, also illustrating their more advanced stage regularly associated with decreased QoL (17). Differences in administered therapies and disease stages should be considered when comparing HRQoL between studies. Furthermore, a recently published prospective phase III trial investigating the impact of 177Lu-PSMA-617 RLT plus standard of care versus standard of care alone reported a beneficial HRQoL for the 177Lu-PSMA-617 RLT group (18). However, because it used “Functional Assessment of Cancer Therapy: Prostate and the Brief Pain Inventory—Short Form” for the assessment of HRQoL and different outcome parameters, a direct comparison with the results of our analysis is not possible (3).
Patients with either slight impairment in physically demanding activities (ECOG 1) or total inability in work activities (ECOG 2) had concordantly lower HRQoL than did patients with fully active performance status (ECOG 0) at all measuring points. This is in line with results from Marinova et al., who investigated HRQoL for patients with midgut neuroendocrine tumors after peptide receptor radionuclide therapy (19). However, the significant impact of 177Lu-PSMA RLT on HRQoL for our total patient cohort was not found within ECOG-divided groups (ECOG 0 vs. ECOG 1 or ECOG 2), although there was a similar tendency detectable (e.g., global health status). This might be explained by the relatively small sample size in each of the analyzed subgroups, which resulted in decreased power of the statistical test. Further studies are warranted to validate our results in larger patient cohorts.
Our study has several limitations, including the single-center retrospective nature of this analysis, which may limit the validity of our results. The small sample size may prevent our findings from being extrapolated and impede the visibility of small effects of 177Lu-PSMA RLT on HRQoL.
CONCLUSION
The results of our analysis indicate a beneficial impact of 177Lu-PSMA RLT on QoL for mCRPC patients. Patients showed improvement in HRQoL and alleviation in relevant disease-related symptoms. In addition, we could demonstrate a significant decline in HRQoL for patients with unfavorable disease progression that resulted in early discontinuation of treatment.
DISCLOSURE
Matthias Eiber reports fees from Blue Earth Diagnostics Ltd. (consulting and research funding), Novartis/AAA (consulting), Telix (consulting), Bayer (consulting and research funding), RayzeBio (consulting), Point Biopharma (consulting), Janssen Pharmaceuticals (consulting and speakers bureau), Parexel (image review), and Bioclinica (image review) outside the submitted work and a patent application for rhPSMA. Robert Tauber reports prior consulting activities for AstraZeneca, Bayer, BMS, Eisei, EUSA, Ipsen, Janssen, MSD, Philogen, Roche, and Sanofi and travel support from Bayer, BMS, Ipsen, Janssen, and Roche. Robert Tauber owns shares of Bayer. Wolfgang Weber is on the advisory boards and receives compensation from Blue Earth Diagnostics, ITG, and Pentixapharm. He has received research support from Blue Earth Diagnostics, BMS, and Pentixapharm. No other potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: Does 177Lu-PSMA I&T RLT have a beneficial impact on HRQoL for mCRPC patients?
PERTINENT FINDINGS: In our analysis, we could demonstrate that 177Lu-PSMA I&T RLT is associated with a beneficial impact on HRQoL. Moreover, we could detect a significant decline in HRQoL for patients who discontinued treatment because of disease progression.
IMPLICATIONS FOR PATIENT CARE: HRQoL is important when it comes to the evaluation of new treatment strategies such as 177Lu-PSMA RLT. 177Lu-PSMA RLT demonstrates a beneficial impact on patients’ HRQoL. However, for patients with early disease progression, the positive impact of 177Lu-PSMA RLT on QoL is limited.
Footnotes
↵* Contributed equally to this work.
Published online Sep. 7, 2023.
- © 2023 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication April 17, 2023.
- Revision received August 1, 2023.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.