


Abstract
4109
Introduction: When an IV needs to be set and an injection is given there is always concern for an infiltration. In molecular imaging, the responsibility for the injection quality falls on the technologist. Although some infiltrations are obvious when they occur, some are more subtle with minor leakage out of the vessel. Until recently, the only way to check for a suspected infiltration after a radiotracer injection was to place the injection site in the imaging system field of view. This type of quality check can indicate some activity was left behind but can only be used when the technologist is aware of the infiltration. This post-injection technique: 1) gives no information on initially retained activity at the injection site, 2) no data on how long the extravasation persisted, and 3) gives no ability to intervene during the injection. For PET imaging, infiltration assessment is especially challenging as patients are typically imaged with their arms outside the field of view and any rescan of the injection site for infiltration confirmation requires a full scan of at least one bed position. It is known that a compromised injection in molecular imaging or a therapy administration can have a big impact on the outcome and can also have lasting effects. The purpose of this abstract is to discuss how an injection monitoring device can be helpful in monitoring infiltrations.
Methods: Over a 6-month period, an injection monitoring device was used to monitor multiple injections in a PET-CT department and multiple Y90 therapy injections in Interventional Radiology.
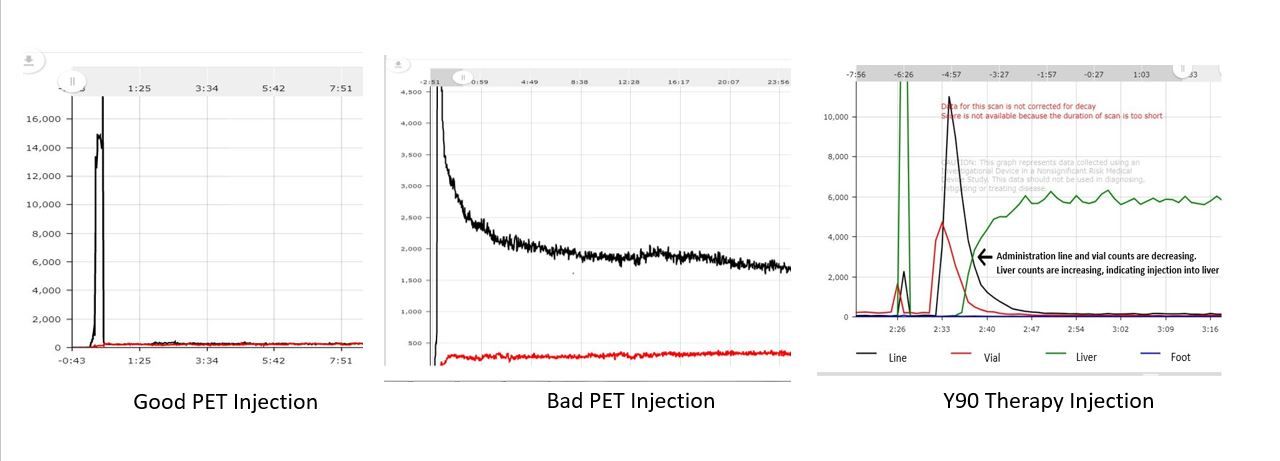
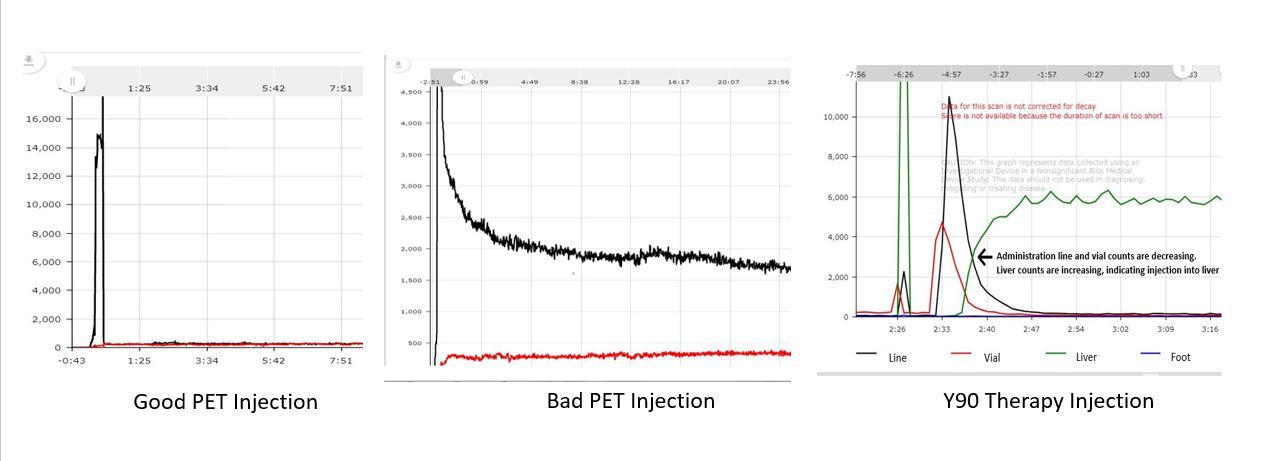
For the PET-CT injections each patient had 2 sensors monitoring the injection. Sensor #1 distal to IV location and sensor #2 on opposite arm in the same location for control. Upon completion of injection, the monitoring system generates an injection curve and score. For the Y90 therapy injections 4 sensors were used. One place on the injection line, one on the dose vial, one on the liver, and one on the patient’s foot. Upon completion of the injection the monitoring system generates an injection curve. No score is given for this type of injection.
A retrospective analysis was completed on both types of injection. In the PET-CT department, the injections were analyzed to see if the administering technologist suppected a comprised injection. In interventional Radiology, the injections were analyzed to see if the monitoring system could detect the therapy leaving the vial and entering the liver for use in real-time confirmation of successful dose delivery.
Results: In the PET-CT department, 590 injections were monitored. 61 injections were flagged by the monitoring system as less than idea injections all falling within minor to major range. Out of those 61 injections only 7 (11%) were noted by the technologist administering the injection to possibly be compromised at the time of injection before seeing the generated curve or score. This indicates that the remaining 89% of injections that were compromised to some degree would potentially have gone undetected without monitoring. In figure1 there is an example of a compromised injection curve and a non-compromised injection curve for reference.
In the Interventional Radiology department, the monitoring system was used on 15 Y90 therapies. The curves generated by the monitoring device indicated that on all 15 therapies the dose exited the vial and entered the liver with the added ability to measure residual activities prior to the patient leaving the procedure room. Figure 1 shows a good injection, bad injection, and a Y90 therapy injection.
Conclusions: Even with years of IV experience, a compromised injection can occur and go undetected. This may be more problematic for injections that take place outside of the traditional Nuclear Medicine setting. Actively monitoring injections can provide timely information on infiltrations and provide physicians with key information regarding possible injection issues to guide clinical decision making.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.