


Abstract
3256
Introduction: In its current form, Molecular Breast Imaging (MBI) is limited in its clinical applications because it does not provide absolute measurements of the 99mTc-sestamibi uptake in benign and malignant breast tissues. Because the measured signal on MBI images depends on both the underlying radionuclide distribution, patient preparation, breast positioning, and acquisition parameters, MBI images cannot be used reliably to compare uptake between patients or even between multiple acquisitions of the same patient. Nevertheless, recent studies have shown that, even with these confounding factors, some MBI measurements such as tumor-to-background counts correlate with response to neoadjuvant chemotherapy. Here, we report a methodology to absolutely quantify 99mTc activity in focal breast lesions with the goal of improving the accuracy and reliability of MBI-based metrics in predicting early response to neoadjuvant chemotherapy.
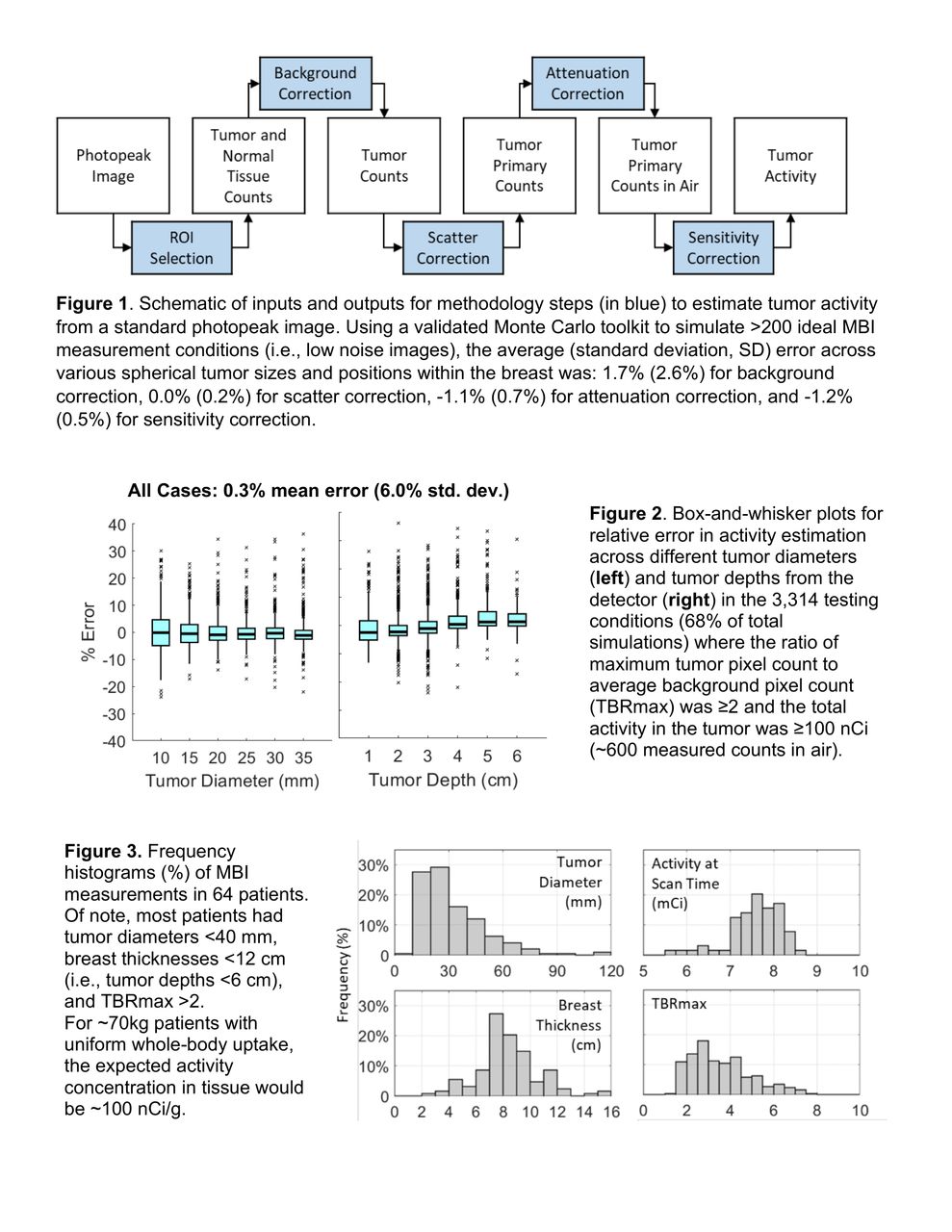
Methods: A 99mTc tumor activity quantification methodology was developed that consisted of 5 steps: 1) tumor delineation, 2) normal tissue uptake subtraction, 3) scatter correction, 4) attenuation correction, and 5) sensitivity correction. A validated Monte Carlo toolkit of the GE Discovery NM750b (https://pubmed.ncbi.nlm.nih.gov/34038878/) was used to image spherical tumors (10-35 mm diameters, 4800 nCi/cm3 99mTc concentration) in air, in “cold” breast tissue (0 nCi/cm3), and “hot” breast tissue (120 nCi/cm3) in order to individually quantify the accuracy and precision of each step. The accuracy/precision of the complete methodology was then tested in a separate independent subset of simulated data encompassing more typical activity concentrations seen in clinical practice (5-90 nCi/cm3 breast, 5-3600 nCi/cm3 tumor).
Results: Tumor activity was estimated as: A = [Ct – (Nt/Nb)*(Cb)] * K * eµz * S, where C and N are counts and number of pixels in tumor (t) and background (b) ROIs, K is a simulation-derived ratio of primary to total counts in the photopeak window, µ is the linear attenuation coefficient of 140 keV photons in tissue, z is the tumor distance from detector, and S is the system sensitivity. Overall, the mean relative error (standard deviation, SD) of each individual methodology step was <1.7% (<2.5%). The mean (SD) relative error in estimated activity was 15.3% (52.0%) in all testing conditions (n=4,877). In preliminary analysis with 64 patient data, most images had measured TBRmax ≥ 2 and had expected tumor activities ≥ 100 nCi (based on administered activities, patient weights, and assuming uniform whole-body distribution). The mean (SD) relative error is 1.5% (18.7%) when the ratio of maximum tumor pixel count to average background pixel count (TBRmax) was ≥2 (n=3,585), but only 53.7% (85.0%) when TBRmax < 2 (n=1,292). However, when TBRmax ≥ 2 and the total tumor activity was ≥ 100 nCi (~600 measured counts in air), the mean (SD) activity error decreased to 0.3% (6.0%) (n=3,314).
Conclusions: This work, to our knowledge, is the first to use MBI Monte Carlo simulations to develop a methodology to quantify absolute 99mTc tumor activity by directly investigating the effects of, and then assessing techniques to correct for, photon scatter and attenuation in tissue, isotropic source emission and detector resolution, and surrounding normal tissue uptake. Evaluation of the methodology with distinct simulated conditions with additional sources of error and the application of this methodology in clinical data is underway.

In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.